Article Text

Statistics from Altmetric.com
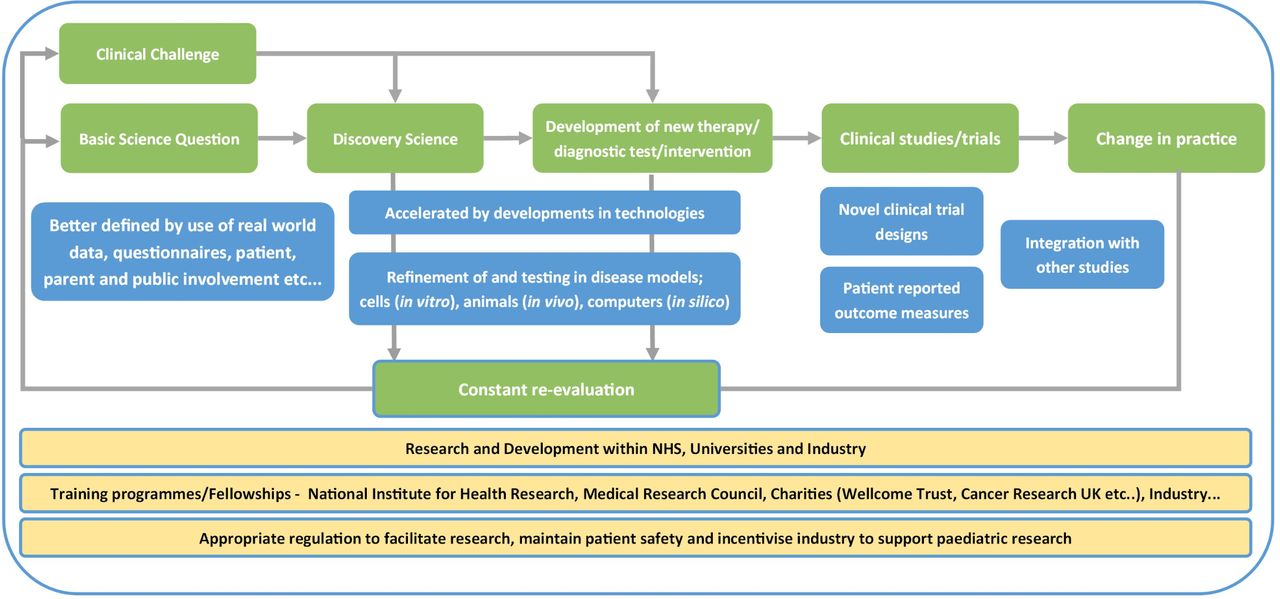
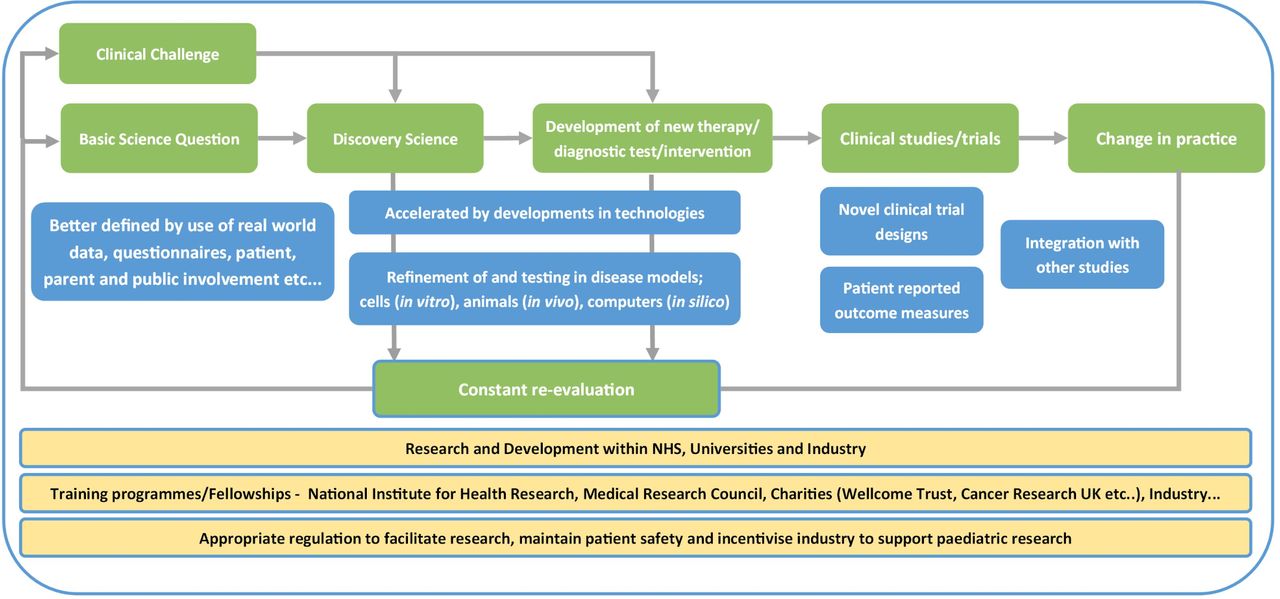
Over the last few years, the Research in Practice section of Archives of Disease in Childhood, Education & Practice has published papers covering a range of methods from basic science to clinical trials as well as initiatives developed to improve implementation and education of research skills. This article attempts to show how such diverse approaches fit together to work to improve patient care. Figure 1 provides a visual representation of how the different aspects, types and components of research work together. In the following sections, we explore how advances in different areas are transforming our understanding of disease and how we look after and treat patients.
{kind=link}
Visual representation of translational medical research. In green boxes are different stages and types of research from the original question/challenge to change in practice. In blue are highlighted advances and in yellow the infrastructure facilitating improved research for children.
Understanding disease pathogenesis
The last two decades have seen an explosion in technologies and methodologies, enabling us to further understand the pathophysiology of disease. Most notably, the development of ‘omic’ technologies has enabled high throughput analysis of the genetic, transcriptomic, proteomic and microbiomic landscape of patients and their diseases (see, eg, What is next generation sequencing?1–4). We will see below how this is impacting on diagnostics and treatments for patients. These technologies, at the most, provide a profile of a given disease or state; however, it is through functional evaluation in model systems, such as cell culture and animal models that we begin to further understand their functional significance. The ability to manipulate the genome using technologies such as CRISPR/Cas95 has greatly advanced our ability to generate and test hypotheses with such models. It is in these models that many therapies are first conceived and tested. In the article, using animal models to improve care of neonatal encephalopathy,6 the authors elegantly show how use of animal models was critical in the developing and translating therapeutic hypothermia from a research hypothesis to standard clinical care for neonatal encephalopathy.
Understanding clinical challenges
In addition to the biology, understanding the clinical presentation, current treatments and infrastructure is also essential. In neonates, the neonatal national research database7 perhaps gives us a gold standard of how routine care and data collection can be combined giving us ‘real world’ data of patient characteristics, current management and outcomes. Improved questionnaire-based and qualitative approaches8 are also a key component to getting a full picture of how diseases affect patients, and the challenges they face, helping keep research relevant to patients ideas, concerns and expectations.
Improving diagnostics
The molecular approaches described in the papers above are now in routine practice for many patients. Targeted sequencing is commonly used (eg, in patients with diabetes and epilepsy), in many places replacing previous single gene tests. In microbiology, 16S and 18S rPCR is used in patients to identify micro-organisms.4 In addition, whole exome and whole genome sequencing approaches are being introduced in, rare disease, critically ill patients in paediatric intensive care units, and routine whole genome sequencing of all childhood patients with cancer is due to start in the NHS in 2020. How to validate such tests, best use such information, counsel patients and characterise the impact on patient outcome, is an active area of research. In other cases, genes, signatures and proteins identified by high throughput technologies have led to the generation of specific cheap tests, such as immunohistochemical stains, to quickly evaluate for certain markers of disease and in areas such as paediatric brain tumours, advanced molecular profiling has revolutionised both the classification and diagnosis of some tumour types.9
However, it is not just molecular testing, advances in imaging, such as MR spectroscopy,10 enable us to understand more and get greater precision with non-invasive tests. Neonatal MRI is giving us new information and becoming more widespread, though how best to use this in the ‘real world’ remains a challenge.11 The use of MRI micro-CT postmortem is enabling non-invasive evaluation of autopsy to the histological level.12 With such rapid advances in technologies, the challenge for the paediatrician is in understanding the relative benefits, limitations and costs of this extensive array of novel diagnostic tests.
Improving therapies
Along with advances in technologies and improved understanding the biology comes the development of new therapies and therapeutic strategies. Notable examples include the development of genetically engineered CAR-T cell therapy as a strategy to cure relapsed acute leukaemia13 as well as disease modifiers in cystic fibrosis, both now with established uses in clinical practice. With such therapies, such as CAR-T cells, there has been a need to study, understand and develop appropriate management strategies for different patterns of side effects, such as the use of anti-IL6 agents to treat cytokine release syndrome/storm. Other new therapies we have covered include oncolytic viruses, a novel approach to specifically targeting cancer cells.14
The evaluation of many of these advances, as well as the refinement of existing approaches, is dependent on high quality clinical trials. Novel trial designs15 16 and the use of harmonised outcome measures17 are helping more efficiently translate these. Importantly, a focus on what are important outcome measure are important for patients18 will be essential for both engagement with and the success of future clinical trials.
Improving infrastructure
To maximise the opportunities of all this work requires good infrastructure. The 100K genome project,19 institutions such as clinical trials units20 and research networks form centres of expertise to support trials. There are now a multitude of training opportunities for trainees in the UK to gain experience in research, from the formal NIHR programmes,21 to specialty led22 to trainee led research networks and ‘virtual academic units’.23 24 At the centre of all care and research is the patient, and ongoing engagement of, and partnership with patients25 26 in driving and delivering research is an essential component to ensure that these advances lead to the improvements in health and quality of life that are required for by our patients. Alongside this, regulations and ethical frameworks ensure that patients are kept safe, research facilitated and incentives to promote industry to engage in paediatric research.
Conclusion
This article provides a brief taster of the diverse types of research, methodologies and advances currently occurring in paediatrics. While paediatric oncology and neonatology have often led the way, advances are accelerating across all areas of child health. As often highlighted, engagement with research is not an ‘optional extra’ for paediatricians, rather a core component of working for the best for our patients. How to deliver this, including navigating the ethical frameworks and a framework to design and review research involving children, is outlined in a recent series of articles in Archives of Disease in Childhood.26–29
Data availability statement
There are no data in this work
Ethics statements
Acknowledgments
JA would like to thank all the authors and reviewers who have contributed to the Research in Practice section over the last few years in providing and/or critiquing such relevant and useful articles.
References
Footnotes
Funding JA is funded by a personal Clinical Trials Fellowship from Cancer Research UK.
Competing interests JA is associate editor of Archives of Disease in Childhood, Education & Practice, with responsibility for the Research in Practice section.
Provenance and peer review Not commissioned; internally peer reviewed.