Article Text

Statistics from Altmetric.com
Introduction
Submitting your project for ethical review and the comments or even criticisms that may follow can be irritating or even painful. There are many stories that recite and relive the difficulties some have experienced, but we do not believe it need be so. There may be some eye-rolling at this, but we ask you to delay judgement until you have read the article, a description of how reviewers tend to approach the process and, from this, we propose a practical approach for researchers.
Contents
Do I need to submit my project for review?
What are reviewers trying to do?
What are the reviewers’ likely concerns and questions in this area?
How can I make my project easier to review?
How can I analyse contentious or ‘tricky’ issues?
What should I do when/if I attend review?
What shouldn’t I do?
A checklist.
Lessons from survivors.
Encouragement.
1. Do I need to submit my proposal for review?
Generally if your work is ‘research’, you will need to submit your project. Audit, service evaluation or quality improvement do not require this. Usually it is easy to distinguish these (if it looks like a duck, swims like a duck and quacks like a duck, it IS a duck). But sometimes judgement is needed. In the UK, the Health Research Authority (HRA) provides a leaflet ‘Defining research’, which tries to differentiate audit, research, service evaluation and public health disease management (http://www.hra-decisiontools.org.uk/research/docs/DefiningResearchTable_Oct2017-1.pdf).
If in doubt, it is worth talking to others and your relevant authorities may provide a helpline. Key discriminants for clinical research are: (1) it may change treatment or intervention according to a protocol not by choices made by a healthcare professional, child or young person (CYP) and parent, (2) allocation to treatment may be randomised and (3) patient and/or healthcare professionals may be ‘blinded’ to a treatment. In other types of work, there is: (1) no change in treatment, (2) treatment is chosen by the healthcare professional, CYP and family and (3) they all know the chosen treatment.
2. What are reviewers trying to do?
Global guidelines1 2 expect reviewers to protect the rights, safety and well-being of trial participants, but in reality, there is a broader agenda that includes consideration of patients and the public. Broadly, review will consider3 the anticipated therapeutic and public health benefits taking account of:
The relevance of the clinical trial.
The reliability and robustness of the data generated in the clinical trial.
The risks and inconveniences for the subject.
Compliance with the requirements for informed consent.
Arrangements for rewarding or compensating subjects.
Recruitment of subjects.
Confidentiality arrangements and data protection.
Researcher and trial site suitability.
Collection, storage and future use of biological samples.
Even then there will be national variations, but the core elements above are fairly constant across jurisdictions and review can be expected to include consideration of any, if not all of these.
3. What are the reviewers’ likely concerns and questions in this area?
Likely key questions (addressed in other article in this series) are:-
How do you justify recruiting children?4
How have you involved families and CYP?5
Is the balance between possible benefits, harms and burdens of any extra tests and research visits) reasonable?6
Are consent, assent and dissent procedures adequate?7
Researchers should therefore be able to address and answer these questions.
4. How can I make my project easier to review?
A logically structured, well-written proposal befriends the reviewer so ensure they have an outline of your proposal early on, maybe in the covering letter. Many research ethics committee members start with the participant information sheet so this should be clearly written in lay language. Once the overall purpose and structure of the study is understood, further reading is easier, and the reviewer will be thinking ‘Ah yes, great, I understand the outline and purpose so now I can explore further with questions in mind’, rather than ‘Oh dear (or worse), I‘ll have to scour all this paperwork to see what is actually going on’.
Write a title that says ‘what’s in the tin’
Basing this around the acronym ‘P.I.C.O.’, Population to be recruited, Interventions (the research methods), Comparator (if there is one) and Outcome (the measures being recorded and studied) is one possible way to do this. It also helps to have a clear ‘research summary’ addressing ‘Why?’ (are you doing the study and what’s the question you hope to answer?), ‘What?’ (area is being covered, what is the intervention being studied?), ‘Who?’ (would be eligible?) ‘Where?’ (is the study taking place?) and ‘How?’ (will the study be conducted and what will participants have to do?). It is crucial this describes the study, particularly what will be expected of participants. Any of these will also serve many different audiences beyond review.
Have a very clear research question and purpose
These are central to any study and must be explained very clearly. Then ensure there is an explanation as to how the method is the best way to answer the question. (If you have) Lay out how you have involved CYP or families in this.
Write in plain English and explain jargon and acronyms
All ethics reviewers expect submissions that lay members on the committee will be able to understand. Failure to do this is one of the most common criticisms of applications.
See the study from the participants’ point of view
This is what the REC does and good research practice requires researchers to consider consequences of participation. One of the best ways to do this is to involve patients and public in design, conduct and dissemination of your project.
If there are key, important issues you think participants must know think through all parts of the consent procedures and consider:
Enrolling an independent clinician to ensure these are explained.
Writing a summary front page.
Setting a short questionnaire after the study has been explained to test understanding.
Recording the consent discussion.
More detail on this specific issue is on http://www.reviewingresearch.com/consent/.
Spend time on your participation information sheet: This is often the first thing reviewers turn to. They read it to get to grips with your application, so it is the first impression they will get of your study. The reality is also that RECs go through information sheets in great detail.
When writing an information sheet8:
See it as a friendly but respectful invitation.
Seek input from CYP or their families. Show it to/involve others, particularly people who might join your study and incorporate their ideas. Point this process out to the reviewers. This could be via groups such as GenerationR Young Persons Advisory Group (www.generationr.org.uk); patient support groups; disease-specific groups; and charities linked to the disease/condition being researched.
Be proportionate. One size will not fit all types of research and guidance recognises this (HRA ref). A study exploring treatments that may never have been used in humans previously, for example, will need very different consent to one where you’re offering a postcard survey about anxiety prior to receiving scan results.
If the PIS is lengthy, write an introductory summary.8
Do not write it at the last minute. Give the writing of a PIS time (and effort). Time invested will save time later and reduce the number of comments from RECs.
Write it with a copy of a popular newspaper by your side. The language used should be no more difficult than that used in these.
As you write or review a PIS, have in mind the question ‘What does participation mean for me (the research participant?’.
The benefits, harms and risks are central, these need to be well described, along with any uncertainties.
A table of what the extra procedures in the research are and also what is to be withheld can be helpful.
Diagrams, pictures or other media can be used to clarify issues.
Think how your PIS fits into your ‘consent process’—evidence indicates the most important part is the discussion, which the PIS can support and frame.
5. How can I analyse contentious or ‘tricky’ issues?
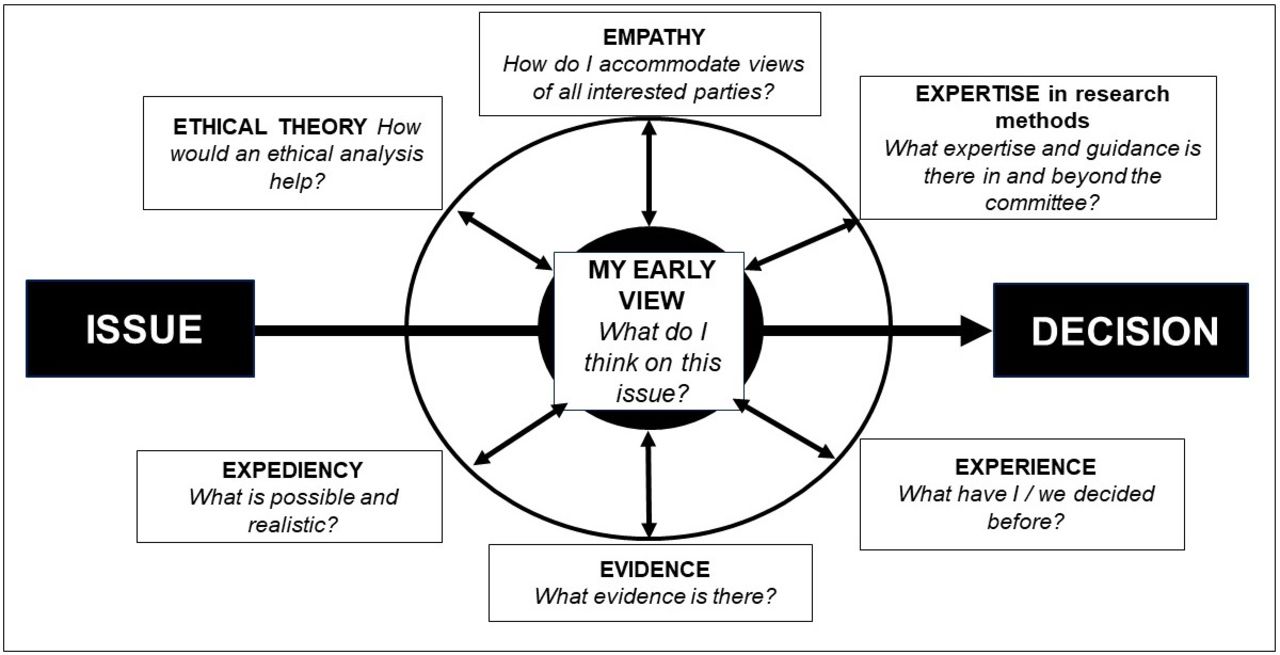
Sometimes the best (most ethical) way to do something is not so obvious. In such circumstances, reviewers will be more sympathetic to researchers who have grasped and analysed ethical difficulties in their study and very cautious of those who deny or duck them. Think about such issues, reason them out with others, draw your conclusions and record such deliberation. More detail is available in the website http://www.reviewingresearch.com/realistic-decisions-making-judgements-in-committee/ and in the figure 1 below.
{kind=link}
Framework for ethical thinking
What are my own views and importantly what are they based on?
How might ethical theory help?
(‘I’ve chosen this design as it fits with my understanding of ethical models and requirements’.) Detailed ethical knowledge is not required. If interested, we would suggest familiarity with the ‘consequentalist’ and ‘duty based approaches’9 would suffice to set out a framework.
How might participants (or others with an interest in the study) think about this issue?
(‘I’ve chosen this method because I think possible participants and patients would support it and I’ve gathered evidence to support this’.) Seek views of those whom you might invite or ideally contact local/national young persons groups.5 This website might also help: http://www.healthtalk.org/young-peoples-experiences/clinical-trials-medical-research/topics.
What expert guidance is there?
(‘I’ve chosen this design as it fits with current guidance I’ve looked up’.) A small library or folder on your PC could help. The Royal College of Physicians Guidelines on the practice of ethics committees in medical research with human participants10 is a good start. It is the most widely quoted guidance from a professional body. Admittedly, it covers all (adult) research, but there is much overlap with research involving CYP. The 2000 guidance from the Royal College of Paediatrics has stood the test of time.11
What have I/we decided before?
(‘I’ve chosen this design as it fits past precedent that has been agreed or deliberations’.) Keep precedent to hand (but present it carefully). As an example of this, this article12 lays out possible questions to address and necessary considerations when waiving consent and consultation in emergencies.
What published evidence is available?
(‘I’ve chosen this design as it fits with current evidence I’ve looked up’.) Have such evidence available to support your position.
What is possible or realistic?
(‘I’m working under some constraints and while I understand this doesn’t justify the unethical, the design means I will be able to complete the study’.) But remember expediency does not justify the unethical.
6. What should I do when/if I attend review?
Attend review (if you are allowed) and even ask if you can’t. If you are a student, come with your supervisor if at all possible. Attendance at a REC meeting in the UK is not compulsory, but it is strongly encouraged. You stand a better chance of explaining your study, resolving misunderstandings and getting a favourable opinion if you are there when the committee reviews it. Many small issues can be resolved speedily in committee.
If you are asked to start the discussion (or you could offer to), we would suggest you start by very briefly describing your study. You could try starting with the ’PICO' and moving into a short 300-word or so summary of your study (‘Who, What, Where, When and How?’). Then you can follow up with the exact research question or purpose you have set and how your method will address this. This should highlight the ethical issues in your study and how you have addressed them. But be succinct.
7. What shouldn’t I do?
Say ‘Well, I didn’t write the protocol’.
Question the reviewers’ authority.
Question their competence.
Fail to complete the application form.
Expand and expand your application.
Say I have just cut and pasted…
Write your application in American, failing to adapt it to UK healthcare.
Use jargon.
Tell the reviewer that science is not their business.
Deny conflicts of interests (or imply you are above them).
Do not turn up when you have said you will.
Send the wrong person.
8. A checklist
Questions that applicants need to be able to answer:
Is there purpose defined by a clear research question, built on what is known already?
Will the method provide meaningful and, if a quantitative project, statistically valid answers to the research question?
Will there be fair, open access to design and results?
Will all the research team have appropriate experience, training, probity and accountability to carry out their tasks?
Is there appropriate patient/participant involvement in the project from its inception?
Is there realistic and fair balance of benefits and harms for all parties with an interest in the project?
Is there valid consent, assent and accommodation of dissent?
Does access to and handling of personal information meet current standards?
Is payment and recompense fair?
When relevant, are there fair post-trial arrangements?
9. Lessons from past experience
We finish with a quote from those who have managed to get their research through REC, of two researchers who have been in the lion’s den and survived!12
Don’t assume detailed knowledge of law or codes of practice [by the REC]. Providing these in advance and quoting relevant sections verbatim may help the committee, which will consist of lay members, clinicians and scientists.
Take great care explaining methodology, especially if you diverge from the dominant paradigm of clinical trials into areas where the committee may have less experience.
Consider whether or not to attend alone. Novice researchers may feel more confident defending their protocols to a committee of 12 members (the norm for a UK NHS REC) if they are accompanied by an advisor or supervisor.
Keep an open mind. A divergence in values between you and the committee is not a personal attack on you. Their opinions are valid and deserve consideration.
Don’t give up. Although only a minority of protocols receive approval on first consideration, the majority are approved following amendments; we have both now had projects successfully approved.
10. Encouragement
When you design your study, involve CYP and/or their families, keep a record of this and also a record of your participants’ experiences—what they liked, what they didn’t and what they found difficult. At the end, ask for their views on their ‘research experience’. You will then double your output and be able to publish two papers at least—your study and an article on the partnership that research should be. You will also probably hear some nice stories about yourself as most enjoy research participation (and if they don’t, you need to change your design). Such evidence is one invaluable foundation (evidence) on which to build future research and its review. It is also a great way of demonstrating that children, young people and families have shaped the research.
And from an experienced paediatrician13:
Sometimes we think that little changes, but in retrospect, the dogged determination of all those researchers has its due effect. I salute them, their perseverance, their endless redrafts and their quiet successes.
Footnotes
Contributors All authors designed and debated the series of articles, made editorial comments and assure the validity of the content. HTD drafted this article initially, with comment and involvement from all authors.
Funding This paper was not specifically funded by any public or charity body. BP is funded by the NIHR Research Trainees Coordinating Centre (PDF 10872).
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Patient consent for publication Not required.