Article Text

Abstract
Major incidents are rare but require a large amount of preparation, co-ordination and communication across different emergency services and specialities. This ensures that casualties are efficiently managed within the constraints of limited clinical resources. This article aims to provide a brief understanding of what constitutes as a major incident, how it is declared and the chain of command in communication and action, focusing specifically on the paediatric process. It also aims to highlight important considerations that could potentially be missed (eg, the mental health impact, forensic evidence and so on).
- Paediatric Emergency Medicine
- Paediatrics
- Child Health Services
Statistics from Altmetric.com
Introduction
Major incidents are defined as specific events (or series of events) causing multiple casualties which exceeds the normal capacity of the NHS and/or other emergency services. A major incident tends to involve many people with varying degrees of severity of injuries and usually occurs in a sudden manner. However, numerous smaller-scale events in combination or anything which could overwhelm capacity can be classified as a major incident.
Major incidents can range from transportation accidents, natural disasters to acts of terrorism or violence. Approximately 14 000 people from across the UK attended a concert at the Manchester Arena in 2017 when it was bombed killing 22 people (including children). Over 1000 were physically injured with many more suffering psychological and emotional trauma.1 Other forms of major incidents may have a smaller media presence but can be just as impactful. In 2020, the Centre for Research on the Epidemiology of Disasters recorded a total of 389 climate-related disasters resulting in 15 080 deaths worldwide.2 These will likely become more common globally with an increase in the frequency of extreme weather events.3
It is a government regulation that all hospitals must have a mass casualty incident plan and provide training and learning exercises to its staff to be prepared for a major incident.4
An overview of a major incident
As these events are uncommon, it is understandable to have a heightened level of concern and anxiety around what is expected from us and what happens throughout this process. Being preinformed is vital as the quality of our response can be critical to the outcomes for patients.
The specialist nature of paediatric care can mean that even a relatively small number of paediatric casualties can quickly overwhelm the usual capacity of a local health system. These are stressful, busy and emotionally challenging events, and being prepared may improve your ability to cope in the moment. Co-ordinating an effective response to a major incident requires everyone across the healthcare system to participate and this may mean that you could be asked to perform tasks outside of your routine practice. Attending major incident training and reviewing local guidelines will invaluably prepare you for such situations. Some hospitals will also have additional plans for managing mass paediatric casualty events.
This consultation will aim to further discuss how a major incident can be managed effectively through this specific paediatric event:
Case scenario
During your shift you hear from the nurse in-charge that a local school bus, with 20 children on-board, has collided with a truck on the motorway. Your hospital is the local unit and emergency services have arrived at the scene, with multiple causalities being reported.
Who decides if this situation is a major incident?
Major incidents can be versatile in clinical presentations. in many different situations that can potentially overwhelm current services/capacity can be considered as a major incident. A major incident can be declared within or outside of a secondary care setting (figure 1).
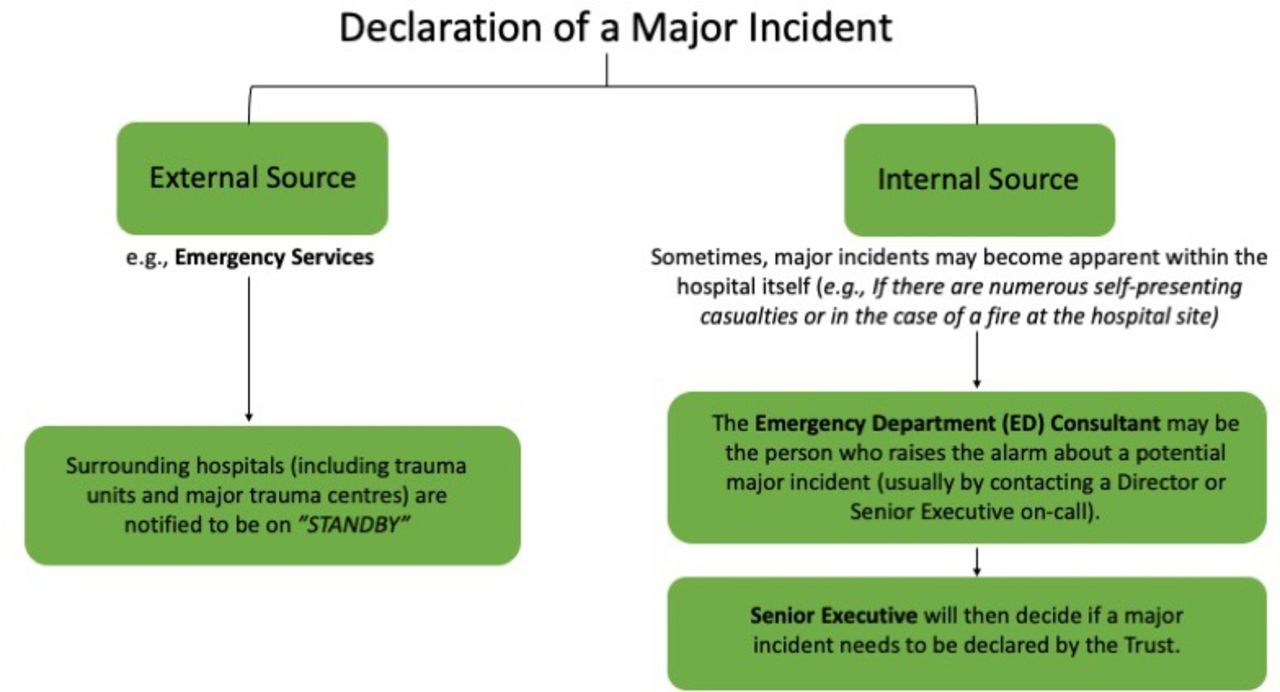
A major incident can be declared through an external source or internally by the hospital itself (usually by the ED consultant who raises it to the Senior Executive).6
When a major incident has been confirmed, the status shifts to ‘Declared—Activate Plan’. This sets in motion a whole cascade of pre-agreed actions, outlined in the local major incident plan.
How is key information communicated?
Given the scale of this event, critical information relayed between the local/regional hospitals, emergency services and the Regional/National Command Centres (set up for individual incidents) needs to be succinct and informed. The current structured format indicates time, location, type of incident, hazards, approximate number and severity of casualties, in which emergency personnel are already at the scene and if more or different expertise is needed. This is summarised in the acronym METHANE (see table 1). This information should be recorded in a place where staff can see and update it in the hospital (eg, white board in ED resus). As shown, our incident has also been relayed in this manner.
A METHANE approach to the example scenario (adapted from ‘Clinical Guidelines for Major Incidents and Mass Casualty Events’ Version 2, September 2020, NHS)6
How is this incident being commanded, controlled and co-ordinated?
Our major incident will draw the attention of multiple emergency services including police, fire service, paramedics and motorway services. These teams individually provide excellent specialist services; however, effective collaboration is critical to successfully manage a major incident. JESIP (Joint Emergency Services Interoperability Programme) was established in 2012 to ensure the emergency responders are trained and exercised to work together as effectively as possible, at all levels of command.5
During any major incident there is a three-tiered command structure; Gold (strategic), Silver (tactical) and Bronze (operational), for each emergency service responding. Gold and silver commanders are not typically located on scene, rather they formulate and strategise the wider implications of a major incident (allocation of resources and media information). Bronze (operational) commanders, directly and collaboratively work at the incident site with their respected staff members. These operational commanders will appoint a lead agency and communicate using the joint decision model throughout the incident to ensure a coordinated and informed response (figure 2).
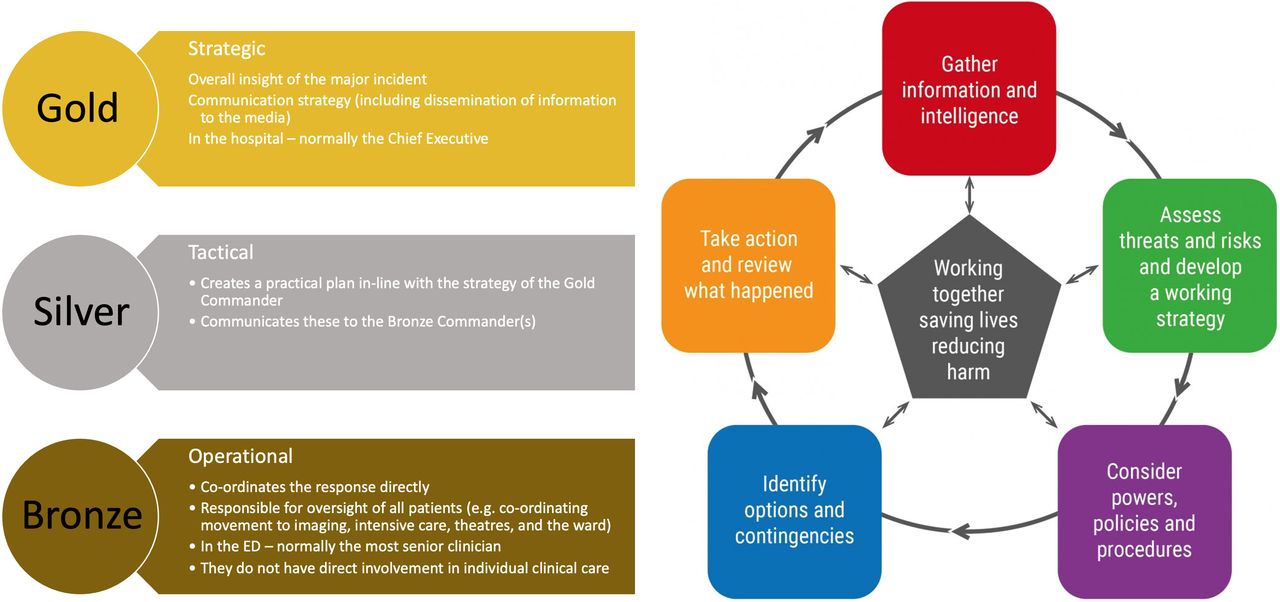
Three-tiered command and control structure to a major incident (left) and JDM from JESIP (right). Adapted from JESIP.15 JDM, joint decision model; JESIP, Joint Emergency Services Interoperability Programme.
For our incident, given the number of potential casualties, it is important that multiple hospital sites are activated, as attendees could quickly overwhelm a single unit. This overview of resource allocation will help ensure the injured children and adults, at the incident, are diverted to the most appropriate centres based on the extent of their injuries while continuing to manage the normal daily influx of admissions.
Most hospitals will have ‘action cards’ which are handed out to key members of staff to allocate roles and duties. These cards normally state your allocated role at the top, followed by a checklist of responsibilities and actions (table 2, box 1).
Examples of ‘action cards’ that might be used in a major incident
Example of tasks paediatricians might be involved in
As paediatricians, depending on our current role/ rotation, given the scale of potential influx, we might be involved in:
Discharging current inpatients.
Preparing the ward to receive patients.
More direct assistance in the emergency department (eg, reviewing medical patients and/or helping paediatric and adult emergency clinicians manage the influx of minor and major injuries).
Who is triaging these patients?
On scene, the ambulance service is responsible for triaging and escorting of all casualties to the hospital safely, if indicated. The triaging system they use consists of four categories (table 3).
Categorising children based on the triage criteria to their appropriate priority level. adapted from ‘clinical guidelines for major incidents and mass casualty events’ version 2, September 2020, NHS6
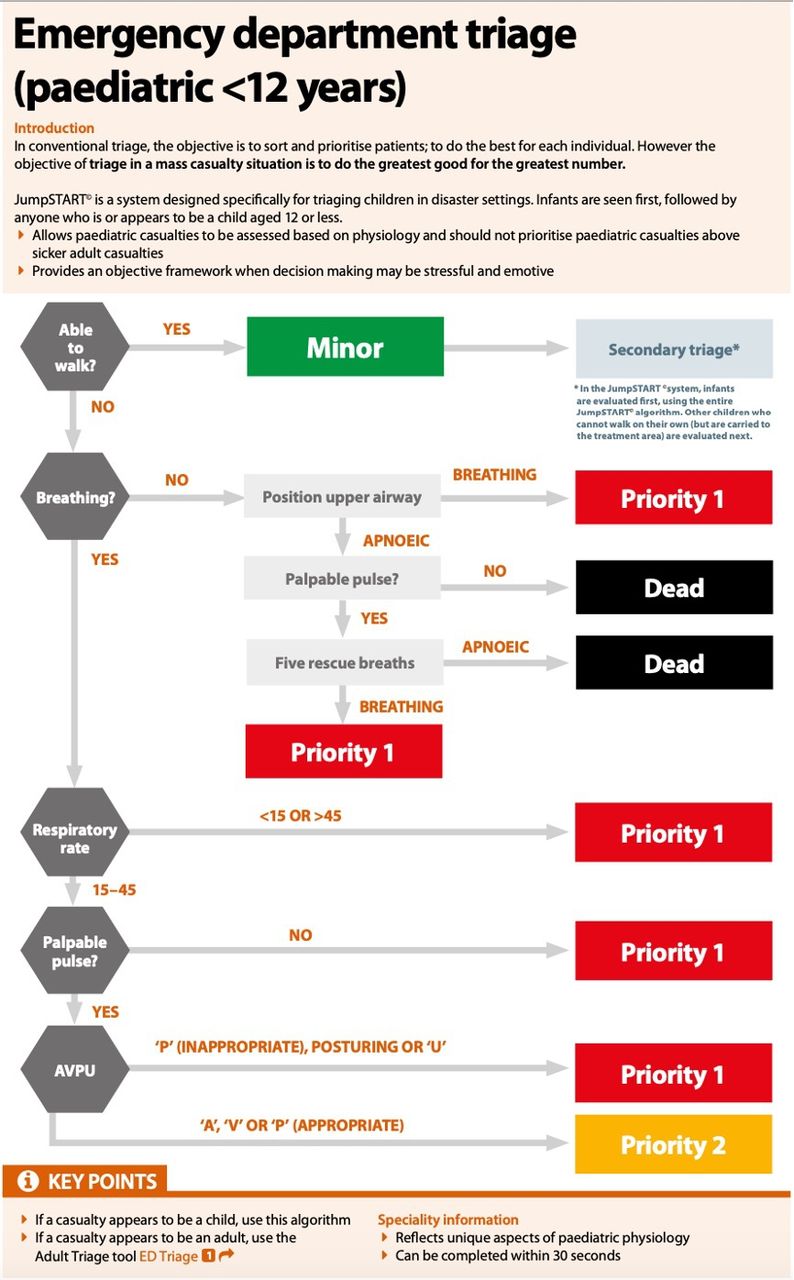
National guidance suggests the use of JumpSTART, a dedicated triage tool for children under 12 years (figure 3).6 However, a study conducted by Malick et al looking at retrospective data in a trauma registry suggested that JumpSTART had a low sensitivity in predicting P1 status. Instead, using the Battlefield Casualty Drills triage system universally for all patients could simplify processes, minimise confusion and allow for standardised training.7 Standardised training and application of a universal triage system could also simplify the process and minimise confusion.8 Figure 4 further elaborates on NHS triaging system for major incidents and mass casualty events, highlighting differences in adult and paediatric triage.

JumpSTART triage used to triage children at the scene of casualty. NHS. Clinical Guidelines for Major Incidents and Mass Casualty Events (Internet). 2nd ed. NHS England; 2020. Available from: https://www.england.nhs.uk/wp-content/uploads/2018/12/B0128-clinical-guidelines-for-use-in-a-majorincident-v2-2020.pdf (accessed 19 February 2022).6

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further elaboration on triaging system from NHS. Clinical Guidelines for Major Incidents and Mass Casualty Events (Internet). 2nd ed. NHS England; 2020. Available from: https://www.england.nhs.uk/wpcontent/uploads/2018/12/B0128-clinical-guidelines-for-use-in-a-major-incident-v2-2020.pdf (accessed 19 February 2022).6
Who should attend the hospital to help with a major incident?
Following this incident, your local major incident plan would have been executed, including specific instructions for switchboard about who to contact. If you have learnt about the incident from colleagues or the media, it is important not to attend the hospital unless you have been asked to do so or would normally be on shift. Remember, the response to a major incident and the additional work in returning to normal afterwards can take days or weeks and it is important that staff are kept in reserve for this.
What else should be considered during a major incident?
Forensic evidence
It is important for the police to investigate how the incident unfolded. Any personal belongings or clothing removed from patients should therefore be minimally handled and while wearing gloves, before placing in individual plastic bags and keeping a note of what has been removed and where it is stored. As with safeguarding incidents, medical photographers may also be present to record injuries or body maps used to depict injuries.
Documentation
Documentation is crucial for recording what decisions were made and why, including the date, time and location of the patient. This is critical for individual patient care and because it may be used as evidence in a subsequent inquiry. All patients will be given temporary hospital numbers on arrival, and these must continue to be used until they are on the ward, even if their real identity is known later.
Mental health impact
As with any other major incident or traumatic life events, staff involved are likely to be impacted emotionally. Effective ‘hot debriefs’ immediately following the incident, provide a safe space to reflect on the incident: answering any concerns and highlighting any immediate lessons that have arisen. Poorly executed debriefs have the potential to cause more psychological harm.9 Subsequent formal multiagency debriefs following the event provide opportunities to review the JESIP principles applied, what worked well and what could be improved for future incidents.10
There is an obvious immediate impact for children and families who have been involved in a major incident and responding to their psychological distress with compassion in the acute phase is a key part of the emergency response.11 We also need to prepare families for the ongoing impact following discharge. Children involved in any major incident can be affected in several ways, and it is important to talk to families about what to expect (see box 2 for examples). Parents can support children by encouraging a return to their routine (including school) and being available to talk about the event and to listen to their child’s feelings. An information leaflet for members of the public about dealing with the mental health impact of a major incident can be found in the NHS document ‘Clinical Guidelines for Major Incidents and Mass Casualty Events’.
On arrival into hospital, a second triage is then performed. This can be emotionally challenging to triage patients to priority 4. The use of objective triage tools can help staff to make these difficult decisions. In these cases, it is important to remember that, although incredibly difficult, finite staff and resources should be prioritised for patients that are likely to survive given any intervention. Children who have been triaged will have a tag with their triage category. Patients for whom a trauma tourniquet has been applied to manage life-threatening limb haemorrhage should have a ‘T’ and the time it was applied written on their forehead (and/or over the tourniquet strapping) to minimise complications from prolonged application.
Examples of how a child can be affected following a major incident
Some examples of what a child can present with due to the psychological distress following a major incident:
Nightmares.
Difficulty sleeping.
Difficulty concentrating.
Physical symptoms (eg, headaches or abdominal pain).
Regression of previous skills (eg, toileting).
Media interest
There is likely to be media interest in the incident in which you have been involved and there may be members of the press attending the hospital to get information. Be wary of the press’ attempts to obtain information or access the hospital and do not offer any interviews or comments of your own. Avoid posting anything on social media about the incident. This is crucial because of the potential impact on friends or family of those involved and also to ensure that any police investigations into the incident are not jeopardised.
Training and exercises
Who would have thought that you would be managing a major incident today? Uncertainty is the greatest challenge in the face of a mass casualty incident. It therefore becomes more difficult to plan and distribute critical resources. Although there will never be a point in time that there is sufficient information in a mass casualty incident, there are ways of mitigating the uncertainty including, preparation for such large-scale events through training.12 This can involve a variety of methods: discussion-based exercises such as workshops, seminars and lectures to operation-based exercises that simulate a scenario, drills and more recently the use of virtual reality.13 14
Making sure that you have read through your trusts local major incident plan will leave you feeling more prepared in the event of one taking place. They are lengthy documents and not intended to be read once a major incident has been declared!
Training exercises should aim to test different aspects of the response system including the clinical issues, command and leadership tactics and the communication system. The aim of these exercises is to identify the strengths and limitations of the current system. As shown however, each incident is unique, and every plan will inevitably have to be adapted to accommodate the situation.
Conclusion
Major incidents are rare; however, they require a great deal of coordination, adaptability and communication between multiple service providers. This multiagency collaboration ensures that all patients are treated appropriately, while accounting for the limited resources and situational uncertainty. Frequent effective training (involving all the relevant departments) is an essential component that is required for each hospital, to ensure their staff are familiar with their roles in a major incident. Moreover, particular attention and training, through JESIP and major incident resources, towards paediatric major incidents will help to build a network of systems that is more adaptable and ready to manage such events.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Correction notice This article has been updated since it was first published. Table 2 and boxes 1 and 2 have been moved closer to their citations.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.