Article Text

Abstract
A 7 year-old twin girl with hypophosphataemic rickets was evaluated for a recent onset of mild strabismus.
She was a homozygous twin sister with hypophosphataemic rickets diagnosed at the age of 2 years, with a mutation in intron 21 of the PHEX gene, which was also present in her sister.
The girls’ clinical histories were remarkable for an important lower limb varus that progressively improved after starting phosphate supplementation with a galenical solution (Joulies solution 1 mmol phosphate/ml) and vitamin D 1,25 OH.
During the examinations, both girls were in good general condition. Physical examinations were unremarkable, except for tibial varus, bilateral fifth finger clinodactyly and bilateral syndactyly of the third and fourth foot fingers. No major head shape abnormalities were noticeable except for a high forehead.
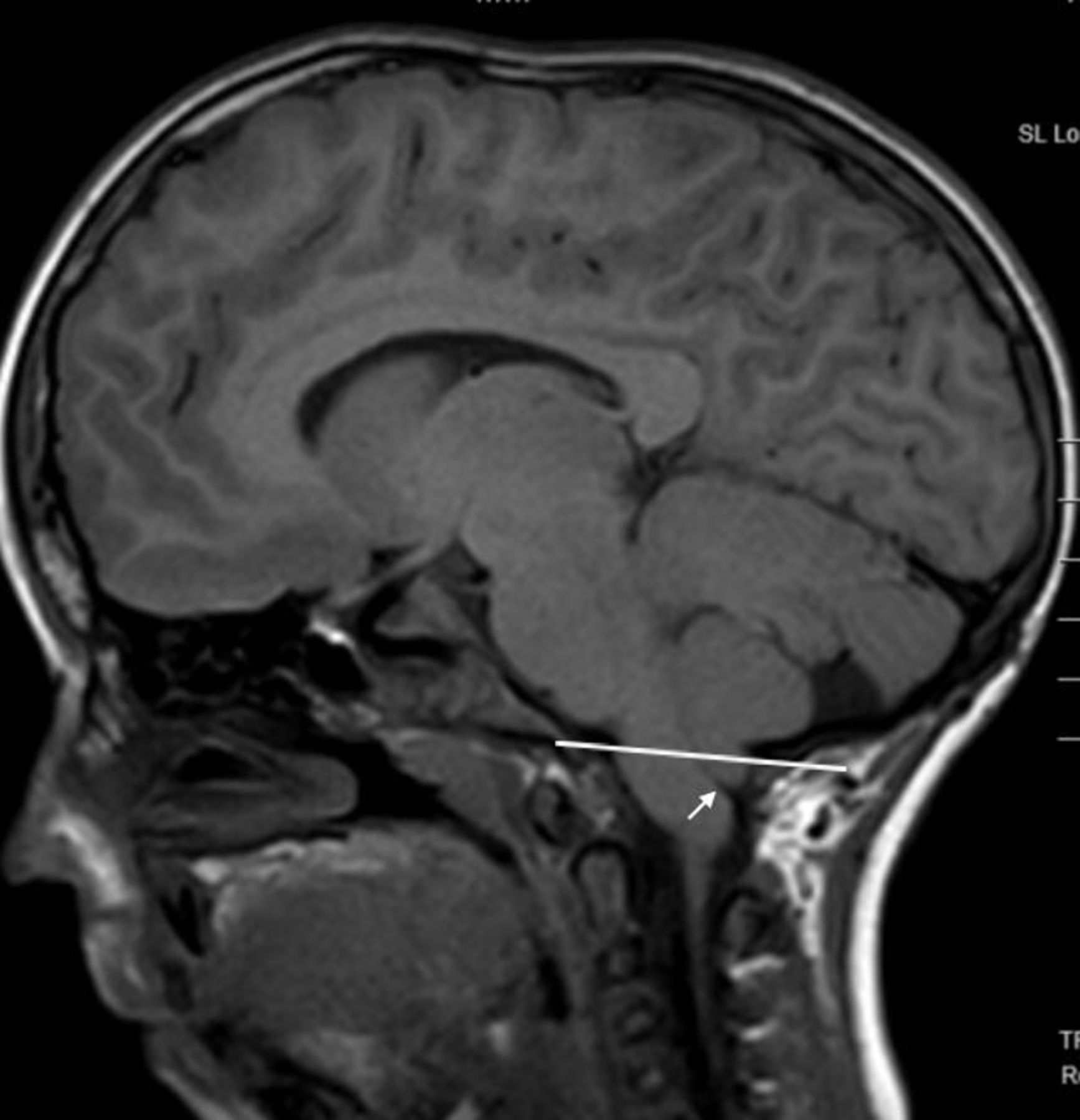
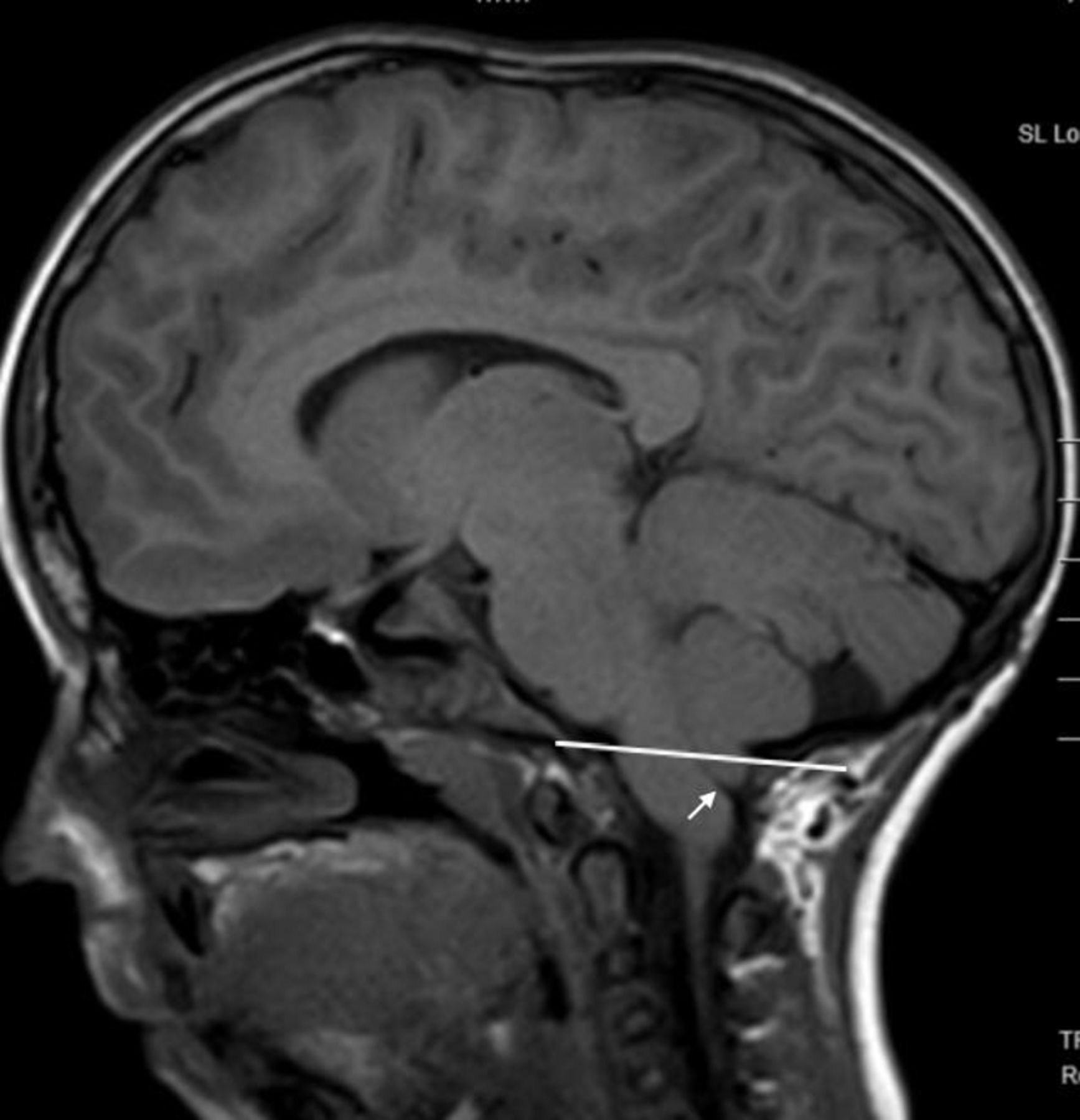
One patient presented with a slight strabismus, normal isochoric isocyclic and reactive pupils, no signs of cranial nerve deficit, and no alterations in the rest of the neurological examination. An ophthalmological evaluation showed bilateral papilloedema. A cerebral MRI scan was then performed, suspecting elevated intracranial pressure (figure 1). The same examination was performed on the asymptomatic sister which also demonstrated papilloedema with similar findings on cranial MRI too.
{kind=link}
Which is the most likely diagnosis?
Craniosynostosis
Pseudotumor cerebri
Drusen
Arnold-Chiari malformation
How should these patients be managed?
Acetazolamide treatment
Third to fourth ventricle cystostomy
Wait and see with periodical visual evoked potential follow-up
Neurosurgery
How should patients with X linked hypophosphataemic rickets (XLH rickets) be managed for the risk of craniosynostosis?
Monitor cephalic anthropometric measures
Perform a MRI scan if clinical signs of craiosynostosis or intracranial hypertension are present
Perform a skull X-ray every 2 years
Perform an MRI scan every 2 years
Answers can be found on page 02.
- ophthalmology
- neurology
- neurosurgery
- twins
Statistics from Altmetric.com
Answers to the questions on page 01
Answer to question 1: A
The MRI scan showed a 12 mm cerebellar tonsillar herniation, due to intracranial hypertension, and the bulb-medullary junction was herniated too. The apex of the epistropheus tooth almost reached the occipital clivus and imprinted the bulb. The physiological liquor film around the encephalic trunk and the herniated tonsils at the foramen magno was not visible (figure 1). A CT scan showed a complete sagittal suture fusion related to scaphocephaly. The epistropheus tooth appearance and the CT scan ruled out an Arnold-Chiari malformation. The MRI abnormalities ruled out a Drusen or a pseudotumor cerebri.
The reason why craniosynostosis occurs in XLH rickets is not clear. A possible explanation may be that usually bone abnormalities in rickets preferentially occur at sites of rapid bone growth, and the skull has a rapid growth in the first years of life.
Answer to question 2: D
Both girls underwent parietal plastic surgery to separate the fused sutures, which reduced the entity of cerebellar tonsils herniation to 6 mm and reduced the bulb-medullary junction herniation, with the restoration of adequate flow of liquor in the space between the epistropheus tooth and the encephalic trunk. Even if one of the twins was completely asymptomatic, surgery was indicated due to the risk of long-term neurocognitive outcomes, even though further studies are needed to assess better the short-term and long-term clinical impact of this complication.1
Burosumab therapy has been introduced recently in patients with XLH rickets and it is at the moment indicated in children over 1 year of age. In the available clinical trials the association between craniosynostosis and XLH rickets in patients that are taking burosumab therapy has not yet been investigated.
Answer to question 3: B
XLH rickets is described as the most frequent metabolic cause of craniosynostosis. Craniosynostosis rarely presents before 18 months of age in children affected by XLH rickets because low levels of plasmatic phosphorus usually develop after 3–4 months of age2 in these patients. On the other hand, XLH rickets should be ruled out in any late-onset craniosynostosis by dosing serum and urine phosphate concentration. Low levels of serum phosphate and reduced tubular resorption of phosphate corrected for glomerular filtration rate are cardinal features of XLH rickets.
According to a 20-year retrospective multicentre case series involving 10 patients with XLH rickets, unusual head shape or findings suggesting elevated intracranial pressure, like frequent headaches, papilloedema, strabismus, are all useful elements to diagnose craniosynostosis associated to XLH rickets.3 Remarkably this condition may be asymptomatic, as in our patients, and in accordance with other reports.4 Craniosynostosis should always be considered a possible complication of XLH rickets. In 1966 Willis et al 5 recommended a radiography of the skull every 2 years during infancy until patients are asymptomatic. Jaszczuk et al suggest that all patients affected by XLH rickets with altered anthropometric measures as cephalic circumference, cephalic index, bone elevation over the anterior fontanel should be investigated with a cranial computed tomography scan.4
Skull X-ray is no longer considered the gold standard to study a craniosynostosis because it is a two-dimensional examination, tridimensional reconstructions are not possible and cranial sutures are not well seen. MRI is recommended to search for alterations of the parenchyma, usually associated with craniosynostosis. A CT scan is necessary before the neurosurgery is undertaken.
Actual clinical practice recommendations for the diagnosis and management of X linked hypophosphataemia recommend monitoring for craniosynostosis and intracranial hypertension. Clinical and neurological signs (head circumference, head shape, headache and vomiting) must be investigated with cerebral and/or spine MRI. To avoid excessive irradiation from radiography or CT, the use of ‘black bone sequence’ in MRI is suggested since it permits an elevated image contrast between bone and soft tissue.6
We suggest that a paediatric ophthalmology evaluation should be also performed yearly to detect signs of intracranial hypertension.
Remarkably craniosynostosis can recur in these patients, so a continuous follow-up is mandatory even after surgery.3
Patients outcome
A year and a half after surgery, both twins are well; strabismus subsided in the symptomatic one.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Martina Bradaschia for the English revision of the manuscript.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.