Article Text

Abstract
A 7-year-old boy with a background of autism presented to the paediatric emergency department with his left arm ‘feeling strange’ then became difficult to rouse. On examination, he was found to have left arm weakness and a left-sided facial droop without forehead muscle involvement. Three hours later, his symptoms had completely resolved and he was suspected to have had a first seizure. He was admitted for observation and an electroencephalography which showed slower rhythms in the right posterior quadrant, which was reported as within normal appearances for his age. He was discharged home the following day. Three days later he became lethargic and vomited. His parents reported dysphasia with use of single-word phrases only, he also appeared confused. He re-presented to the paediatric emergency department, where he was found to have increased tone in the left arm, ankle clonus and an upgoing plantar reflex on the left hand side.
Questions
What are the differential diagnoses and what investigations should be considered?
What type of imaging modality has been used for figures 1 and 2 and what do they show?
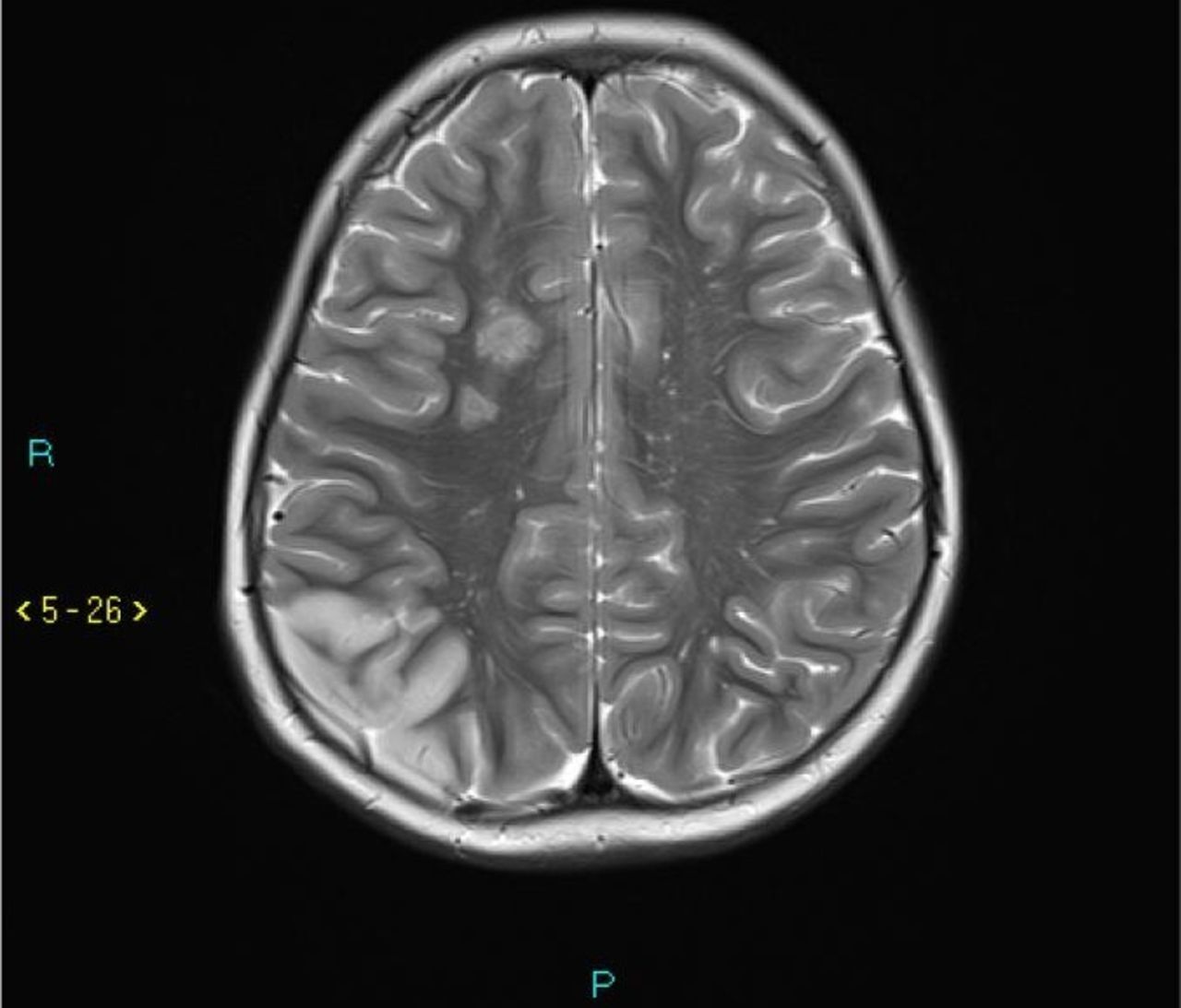
What type of imaging is used in figures 3 and 4 and what do they show?
What is the difference between moyamoya disease and moyamoya syndrome?
Histologically in what way does MMD affect the cerebral vasculature?
What are the different types of MMD?
What are the management strategies used in MMD?
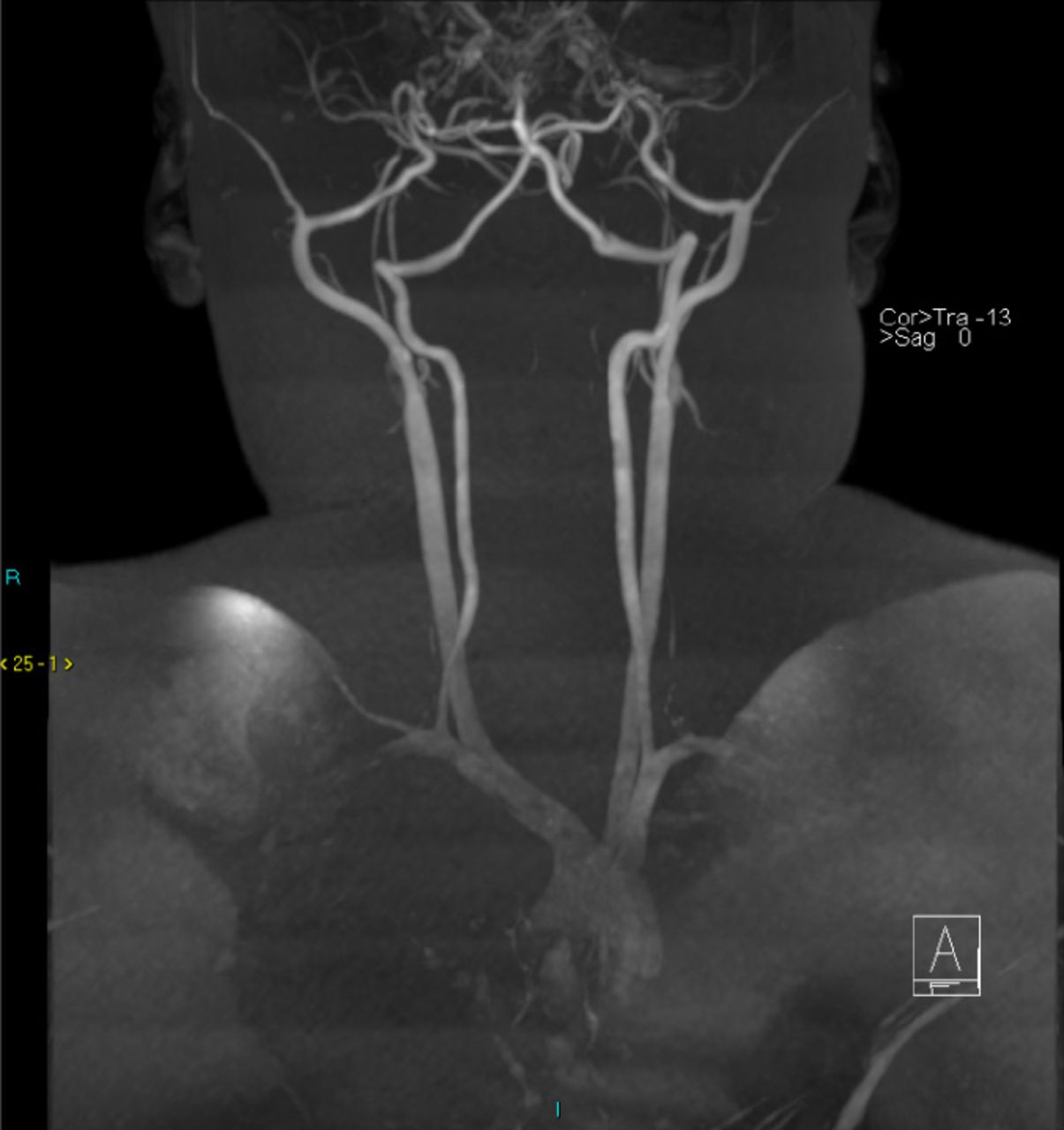
MRI angiogram (MRA) showing the internal carotid arteries (ICA). The left ICA is extremely stenotic at the skull base. The right ICA is occluded at the skull base. The basilar artery is occluded.

MRI angiogram demonstrating extensive reconstitution of the intracranial internal carotid arteries via collateralisation from recurrent facial, orbital and skull base branches of the eonline xternal carotid arteries. Supply to the posterior circulation is via the posterior communicating arteries, and also via multiple small collaterals arising from the distal vertebral arteries, the posterior inferior cerebellar arteries (PICA) and deep cervical branches.
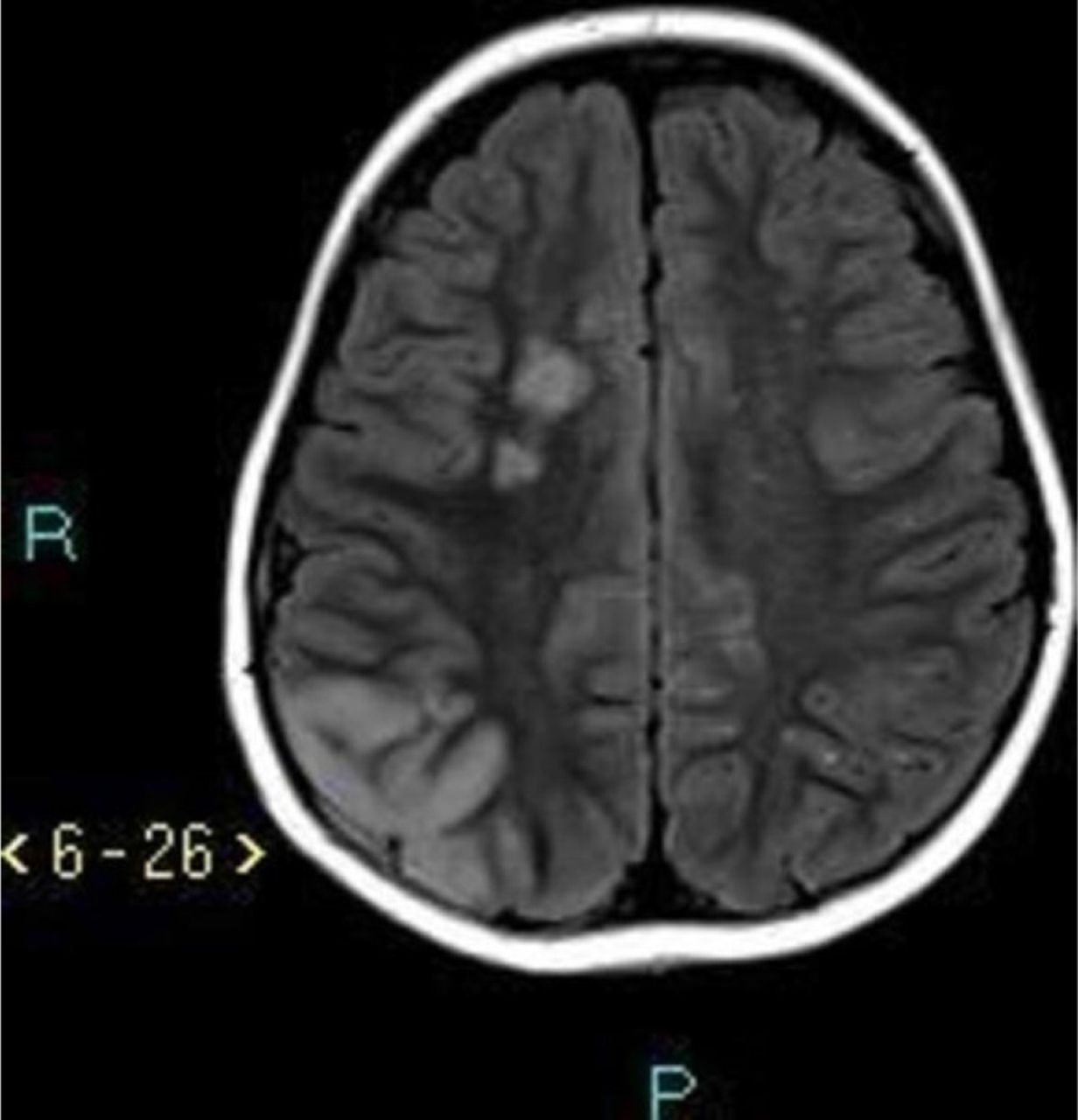
Fluid-attenuated inversion recovery (FLAIR) MRI image demonstrating multifocal bilateral acute infarcts of varying sizes, the largest of which affects the posterior right hemisphere. Many of the infarcts are watershed in distribution.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
T2 MRI image demonstrating multifocal bilateral acute infarcts of varying sizes, the largest of which affects the posterior right hemisphere.
Questions Answers can be found on page 2.
- moyamoya
- angiography
- stroke
- TIA
Statistics from Altmetric.com
Footnotes
Contributors DM wrote the manuscript. JM contributed to the writing of the manuscript. DM reported the images. KH edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.