Article Text

Statistics from Altmetric.com
Bowel gas is usually confined to the lumen of the gut, but owing to a variety of pathological processes, gas may escape into the peritoneal cavity. It is important to recognise the radiographic signs of pneumoperitoneum because bowel perforation usually requires surgical intervention. Patient morbidity and mortality is often significantly increased if this is delayed.
Sub-diaphragmatic air is usually easy to identify on an erect chest radiograph (CXR) and appears as a dark crescent of gas under each hemidiaphragm, provided the patient has remained erect long enough for free air to rise, and there is a sufficient volume of air to allow identification (fig 1A⇓). Free gas is best seen on the right side above the distinct dome shaped outline of the liver (fig 1B⇓). In sick patients, particularly those on ventilatory support, it is not possible to obtain an erect CXR when bowel perforation is suspected. Free intraperitoneal air can also be identified on abdominal radiographs (AXR), the majority of which are taken supine in both adults and children. A careful inspection is required in order to identify the signs associated with free intraperitoneal air, particularly if there is clinical suspicion of perforation or the patient has risk factors such as necrotising enterocolitis (NEC) or steroid treatment. Remember that no free gas may be seen if a bowel perforation has been sealed off by the omentum.

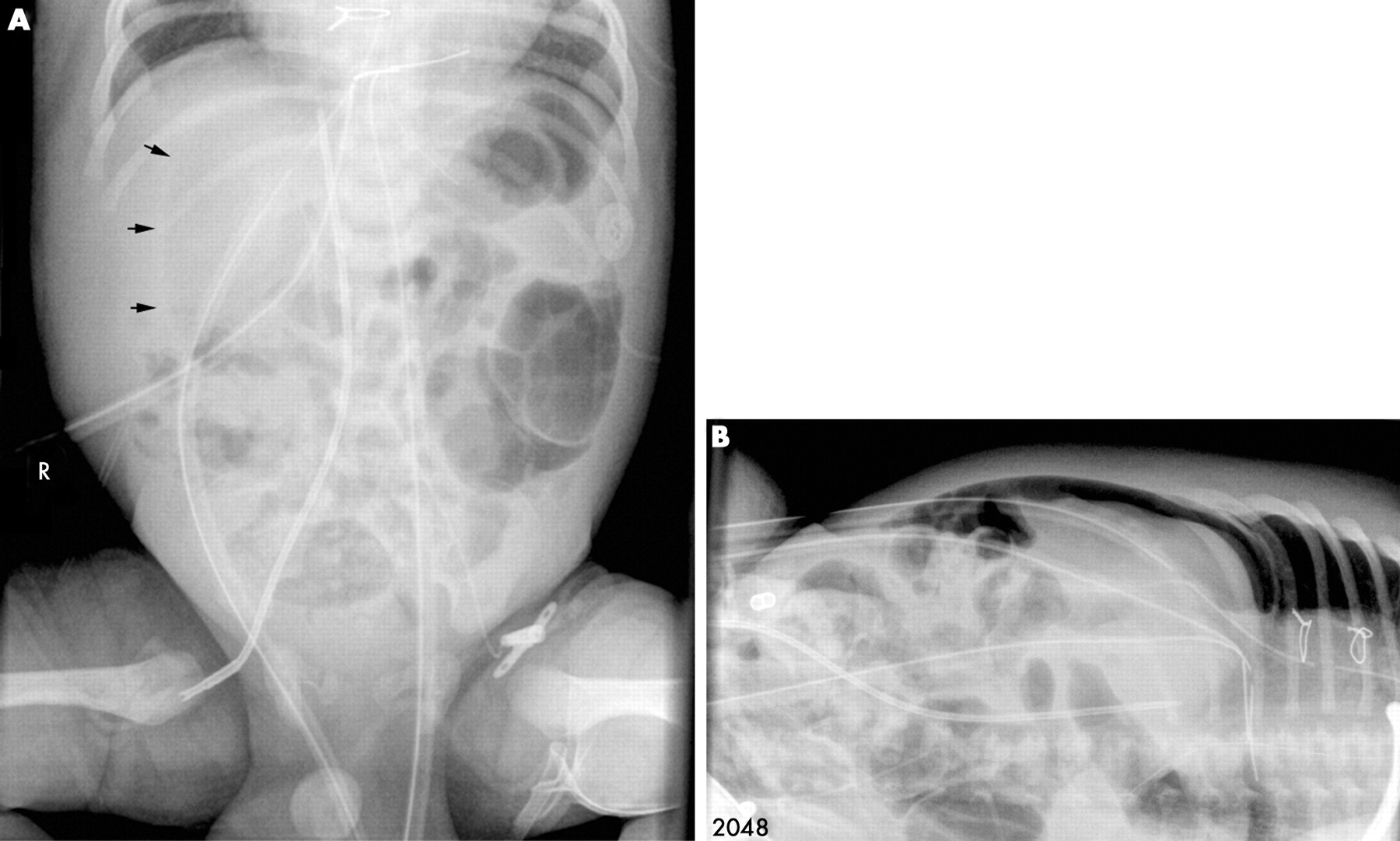
(A) Free air under both hemidiaphragms on erect chest radiograph (CXR) in an infant who had closure of a stoma 24 hours previously. (B) Free intraperitoneal air seen predominantly under the right hemidiaphragm on erect CXR.
APPROACH TO INTERPRETING THE ABDOMINAL RADIOGRAPH
It is helpful to have a routine checklist when reviewing an AXR requested because of abdominal symptoms or signs. This should include checking the bowel gas pattern—is there too much or too little gas, abnormal distension of bowel loops, or a gasless abdomen? Abnormal gas collections outside the bowel may indicate abscess or perforation. Gas within the bowel wall itself (pneumatosis) is seen in NEC and other conditions including gastrointestinal infections (especially in the immunocompromised patient), connective tissue disorders and inflammatory bowel disease. Pneumatosis can also be idiopathic. Gas may also be in an abnormal location within other organs such as the liver, either in the portal system or biliary tree. The soft tissue shadow of the solid abdominal organs may indicate enlargement and abdominal masses may be seen as an abnormal soft tissue density. The location of abnormal calcification can give clues to diagnosis—for example, peritoneal calcification following intrauterine perforation, or suprarenal calcification in a neuroblastoma or secondary to previous haemorrhage. Finally, do not forget to assess the position of any support lines, catheters or drains. It is not unusual to see free intraperitoneal air after laparotomy or laparoscopy and during peritoneal dialysis.
RECOGNISING THE SIGNS OF PNEUMOPERITONEUM
Under normal circumstances only the inner surface of the bowel wall may be defined by gas, but when there is pneumoperitoneum, both sides of the wall may become visible so that the bowel wall looks thinner and very sharply defined. This is called Rigler’s sign, sometimes referred to as the “double wall sign” (fig 2⇓). When there is notable gaseous distension of the bowel it can appear that both sides of the bowel wall are visible when two loops of dilated gas-filled bowel are adjacent to one another producing a pseudo-Rigler’s sign. In association with Rigler’s sign, free air often assumes abnormal triangular of rhomboidal shapes when it becomes trapped in the potential space between adjacent loops of bowel. The presence of intraperitoneal gas can also lead to visualisation of structures that are not normally seen such as the falciform ligament (Silver’s sign) (fig 3⇓) and lateral umbilical ligaments which are peritoneal reflections in the lower abdomen, because of air being present on either side of them. As a general rule, air rises to the least dependent part of the body, so that if a patient is lying supine, free air should rise to the uppermost part of the peritoneal cavity. It may be seen as an abnormal lucency over the liver or in the central part of the abdomen where it often assumes an ovoid or circular lucency which is referred to as the “football sign” (fig 4⇓). This sign is most frequently seen in neonates. Air can also collect in Morrison’s pouch (the hepatorenal recess) which is inferior to the liver and above the right kidney, often making the free edge of the liver visible (fig 5⇓). Occasionally a patent processus vaginalis allows free air to enter the scrotum.

Same patient as fig 1B⇑. This child had a ventriculo-peritoneal shunt in situ following removal of a posterior fossa tumour. His abdominal radiograph (AXR) was done for abdominal pain and demonstrates Rigler’s sign. It was thought that the distal tip of his shunt may have eroded through the bowel wall and he underwent laparotomy. No perforation was found but there was pneumatosis of the sigmoid colon. Presumably one of the “blebs” on the sigmoid had ruptured allowing air into the peritoneal cavity—a non-surgical cause of pneumoperitoneum.

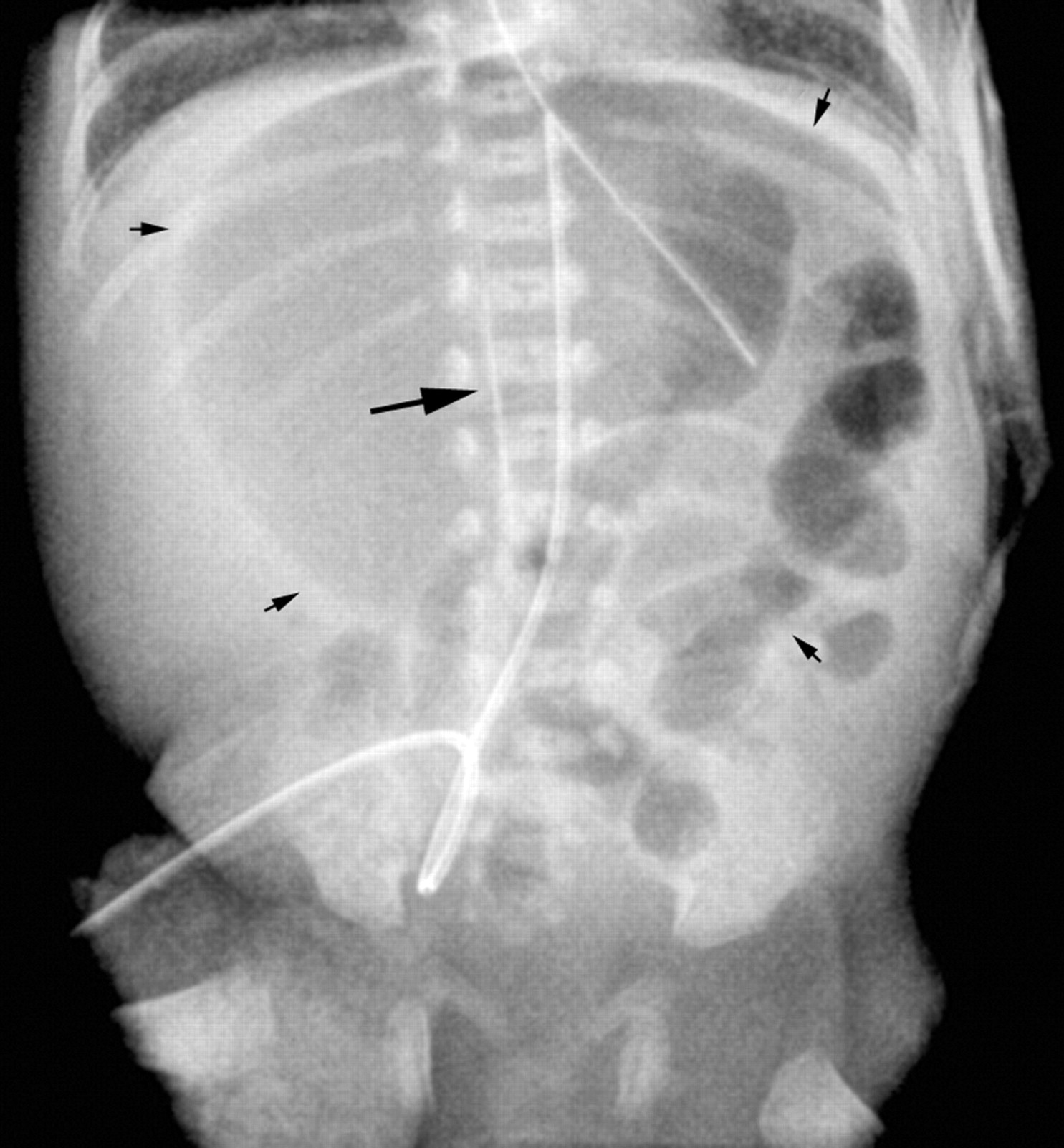
Neonate with necrotising enterocolitis (NEC) and a large pneumoperitoneum. There is Rigler’s sign in the right side of the abdomen (white arrows), the falciform ligament is visible (black arrow), and free air is seen over the liver and under the diaphragm. Note the mottled appearance of bowel in the left side of the abdomen caused by intramural gas.
There is a football sign in this neonate with bowel perforation secondary to NEC (small arrowheads). The falciform ligament is also visible (large arrow).

Another neonate with NEC and pneumoperitoneum secondary to perforation. There is lucency over and around the right side of the liver, and the liver edge is outlined by a triangular collection of gas in the hepatorenal recess.
Free intraperitoneal air on AXR: key points
Rigler’s or double wall sign—the bowel wall is sharply defined because there is air on both sides
Triangular or rhomboidal shaped gas collections that are not intraluminal
Visualisation of structures not usually seen—for example, falciform ligament, peritoneal reflections or the liver edge
Abnormal lucency projected over a solid organ such as the liver
Football sign—non-dependent air in a ovoid/round bubble in the centre of the abdomen
If in doubt or for confirmation request left side down decubitus or lateral shoot through AXR
If the diagnosis of pneumoperitoneum is not clear on the supine AXR, particularly if there is a high clinical suspicion of perforation, a decubitus view should be requested with the patient lying on their left side, right side uppermost. In this position, free air is clearly seen between the lateral ribs and the liver (fig 6⇓). The patient often needs to remain in this position for up to 15 minutes to allow the air to rise before the image is taken. If the patient is too unwell for supine positioning, pneumoperitoneum may be demonstrated by a “lateral shoot through” AXR, where a horizontal x ray beam is directed across the patient lying supine. Free air is seen uppermost in the peritoneal cavity below the abdominal wall. Again, the free air seen anteriorly in this position often has a triangular or rhomboidal shape trapped between loops of bowel.

(A) Subtle lucency with slightly curved edge (small arrowheads) over the right side of the abdomen. (B) Pneumoperitoneum was confirmed on the decubitus film.
Finally, even on a supine CXR taken in a very young or sick patient a large amount of free intraperitoneal gas may be seen as an abnormal lucency beneath the diaphragm with a convex upper border—this is the top of the football sign or bubble of air that would be seen on the supine AXR (fig 7⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Supine CXR showing a large amount of free air under the diaphragm in a neonate with NEC.