Article Text

Abstract
Objective Kawasaki disease (KD) is an increasingly common vasculitis with risk of coronary artery aneurysms (CAAs). The last UK survey was in 1990, whereas current epidemiology, treatment patterns and complication rates are unknown. The aim of this study was to address this knowledge gap.
Methods A British Paediatric Surveillance Unit survey in the UK and Ireland from 1 January 2013 to 28 February 2015 ascertained demographics, ethnicity, seasonal incidence, treatment and complication rates.
Results 553 cases were notified: 389 had complete KD, 46 had atypical KD and 116 had incomplete KD; 2 were diagnosed at postmortem with an incidence of 4.55/100 000 children under 5 years, with a male to female ratio of 1.5:1 and a median age of 2.7 years (2.5 months–15 years). Presentation was highest in January and in rural areas. Most were white (64%), and Chinese and Japanese Asians were over-represented as were black African or African mixed-race children. 94% received intravenous immunoglobulin (IVIG). The overall CAA rate was 19%, and all-cardiac complications affected 28%. Those with CAA received IVIG later than in those without (median 10 days vs 7 days). Those under 1 year had fewer symptoms, but the highest CAA rate (39%). Overall 8 of 512 cases (1.6%) had giant CAA, and 4 of 86 cases (5%) under 1 year of age developed giant CAA. Mortality from KD was 0.36%.
Conclusions The UK and Ireland incidence of KD has increased and is more frequently seen in winter and rural areas. Delayed IVIG treatment is associated with CAA, suggesting earlier and adjunctive primary treatment might reduce complications to prevent CAA, particularly in the very young.
- kawasaki disease
- cardiology
- epidemiology
- paediatric practice
Statistics from Altmetric.com
What is already known on this topic?
Kawasaki disease (KD) is the most common acquired heart disease in the Western world, with the highest incidence in North-East Asians and with unknown aetiology.
Seasonal variation, with peaks in winter and spring, and reported epidemics suggest that there are environmental factors that trigger the condition.
The original British Paediatric Surveillance Unit study in 1990 suggested that UK patients might have high coronary artery aneurysm (CAA) rates despite intravenous immunoglobulin (IVIG).
What this study adds?
There is a rising incidence of KD , with increased incidence in Asians and Black Africans , and increased incidence in rural populations.
Children under 1 year are at highest risk of CAA (39%), are more likely to present with atypical KD. Late diagnosis is associated with CAA
The overall frequency of CAA remains high at 19% despite more widespread use of IVIG, although mortality is now tenfold lower than documented in 1990.
Background
Kawasaki disease (KD) is a self-limiting medium-vessel vasculitis of unknown aetiology that typically presents in children and adolescents with fever and mucocutaneous changes. If left untreated, 15%–25% of children will develop coronary artery aneurysm (CAA); 2%–3% of untreated cases die as a result of coronary vasculitis causing myocardial ischaemia, sometimes many years later.1 The incidence of KD varies from 308 per 100 000 children under 5 years in Japan, to about 5–8 per 100 000 in England.2 3 The high rate in North-East Asians, which persists after migration to countries with low incidence,4 is strong evidence for a genetic factor, and there is clear evidence from genome-wide association studies of an important role of genetic variants in determining susceptibility. The aetiology of KD is unknown, but seasonal variation, occurrence of epidemics and association with wind patterns would be compatible with an infectious or toxic trigger.5 6
KD is the most common cause of acquired heart disease in children in the UK and USA.7 8 Prompt diagnosis is essential to minimise complications. Intravenous immunoglobulin (IVIG) has formed the mainstay of primary treatment following publication of a seminal clinical trial in the 1980s.9 However, IVIG resistance occurs in up to 20%–40% of unselected cases and is associated with increased coronary complication rates.1 10 Recent studies and meta-analyses of all published studies have suggested that addition of corticosteroids to IVIG reduces the risk of CAA, particularly in high-risk patients.1 10 11 However, there is currently no reliable method to predict which patients are at risk of CAA and thus require additional treatment, as scoring systems that predict IVIG non-response in Japan have not been reliable in studies in the UK and North America.
The last comprehensive epidemiological study of KD in the UK was undertaken by the British Paediatric Surveillance unit (BPSU) in 1990.12 This revealed an incidence of 3.4/100 000 children under 5 years from 1 January to 31 December 1990, and a higher than expected coronary complication rate of 29% in those children who had received IVIG, comparable with those patients who did not receive IVIG. More recent epidemiological studies noted a higher UK incidence of 8.39–9.1/100 000 children under the age of 5,3 8 but both were limited by indirect retrospective epidemiological methodologies and thus may not be accurate. Moreover, 24% of children with KD are older than 5 years,13–15 but accurate UK epidemiological data are lacking in this age group.
The incidence of KD has been reported to be increasing in many countries. Furthermore, the population demographics are changing, and there is therefore a need for updated information on KD in the UK.1 16 17 The purpose of this study was to establish the current incidence of KD in the UK, noting the seasonal variation; to assess complication rates and the factors influencing these; and to shape future management practice based on these data (box 1). Areas of particular interest included the potential influence of ethnicity, urbanisation and disease outcomes in the light of recently updated clinical guidance regarding the use of corticosteroids for KD.1
Summary of the British Paediatric Surveillance Unit Kawasaki disease (KD) research questions
Incidence
What are the demographics (sex, age, ethnicity, area of residence) of those diagnosed with KD in the UK and Ireland less than 16 years old?
Has the incidence changed since the last survey in 1990?
Clinical presentation and cardiac complications
How does KD first present, and what is the interval between first presentation and diagnosis?
What is the frequency and nature of cardiac complications detected using echocardiography within 30 days of developing KD?
Clinical management
What acute treatment is being given to patients during their initial hospital presentation with KD?
Are treatments other than aspirin and intravenous immunoglobulin being used, and if so, have these impacted on outcome?
Other outcomes
What is the frequency of non-cardiac complications within 30 days following KD?
How are patients with KD being followed up within the UK and Ireland?
Methodology
The study used the BPSU methodology for the epidemiological research surveillance, similar to the 1990 BPSU KD survey.12 Each month all paediatricians and paediatric cardiologists (list available from the Royal College of Paediatrics and Child Health and the British Congenital Cardiac Association) were contacted by email to report if they had seen a case of KD (box 2). If notified, the BPSU would then make the research team aware and a questionnaire was posted. This surveillance methodology provided an active, real-time quantitative portrait of KD in the defined population. All of the UK and Ireland were included in the study. Also included were the Channel Islands and Isle of Man. Incidence was calculated by applying the most recent resident population data from the 2011–2015 Census of Population18 and their equivalents from Ireland.19
Inclusion criteria
In the first year, the protocol requested the reporting of only complete KD cases, but in the second year all cases of KD (ie, including atypical and incomplete KD as per the aforementioned definitions) were included. Where the interpretation of clinical features was uncertain, expert panel review (RMRT, RM-W, AVR, EJT, DS, PAB) of the case was undertaken to ascertain by consensus (defined as 100% agreement among experts) if the diagnostic criteria for KD had been fulfilled, and if so how to classify the subtype of KD (complete, atypical or incomplete) for inclusion in the study.
Exclusion criteria
The exclusion criteria were patients older than 16 years, outside the predefined study period and those with alternative final diagnoses. In addition, for the first year of the study, those with streptococcal infection were excluded, but not in the second year of study, since it is now recognised that streptococcal infection (and other infections) may be associated triggers for responses resulting in KD.20
Cardiac involvement
We defined CAA as a Z score of ≥2.5 internal diameter.21 The Z scores were checked or completed, using the Cardio Z software, based on the data supplied by Dallaire and Dahdah.22 Those with aneurysms were referred to as CAA+ and those without were CAA−. In addition, there were some children with bright coronary artery walls, dilated (but non-aneurysmal) coronary arteries, pericardial effusion or myocarditis. These were recorded as cardiac involvement, but not CAA. We recorded the early presence of CAA at diagnosis, and also in some cases later echocardiographic data were also presented. Giant aneurysms were defined as ≥8 mm or Z score ≥10.23
Duration of the study
In accordance with the most recent BPSU methodology, data collection was over a 25-month period, January 2013–February 2015. All data were collected and retained in accordance with the Data Protection Act 1998.
Data management, analysis and security
As approved by the ethics committee, parental consent was not obtained as the identity of the cases was known only to the reporting clinician. Anonymous questionnaires were sent from our study centre after case notification. Use of the National Health Service number and date of birth allowed checks for duplication. Using the first four components of the postcode, the population density was estimated by area where each patient lived in the UK and by area in Ireland. As most of the data were categorical or not normally distributed, statistical methods based on the χ2 test were used. Statistical analysis was undertaken at Heriot-Watt University (MD, RS) using SPSS V.24. A p value of <0.05 was considered significant. The distribution of numerical values was summarised as medians and ranges; the Wilcoxon-Mann-Whitney test was used for group comparisons of those with or without CAA. A complex system-level security protocol was used and was risk-assessed on an annual basis.
Results
Between 1 January 2013 and 28 February 2015, 601 reports of KD were received by the BPSU, with 38 duplicates, 9 other diagnoses and 1 with no clinical information. Of the remaining 553, there were 389 cases of complete KD; 46 atypical cases with fewer than 4 clinical features but with abnormal echocardiograms; and 116 cases of incomplete KD. Two cases were diagnosed retrospectively at postmortem without any clinical data to allow KD subtype categorisation (table 1).
Demographics of Kawasaki disease in the UK and Ireland
Boys comprised a significantly greater proportion of the cases, and the proportion of Black and Asian patients was increased relative to the expected proportion of these groups in the population (table 1).18 There were significantly more children under 1 year old with atypical or incomplete KD (45/95; 47%), compared with children over 1 year old (102/428; 24%) (χ2=21.31, p<0.0001).
The annual incidence was estimated using the 257 cases that had been diagnosed between 1 February 2014 and 31 January 2015. Only those whose ages were reported are included. Only in the second year were all subtypes of KD reported. The age-specific annual incidences were 4.55/100 000 at age 0–4 years, 1.26/100 000 at 5–9 years, and 0.08/100 000 at 10–14 years.
Date of diagnosis
Based on 479 cases reported between 1 February 2013 and 31 January 2015, more cases occurred in the winter (defined as December–February) and spring (March–May) than in the summer (June–August) and autumn (September–November) months (figure 1) (χ2 tests for monthly and seasonal variations were significant at p=0.08). These results controlled for length of month and confirmed the appreciable peaks in January in both ‘all’ and ‘complete’ cases.
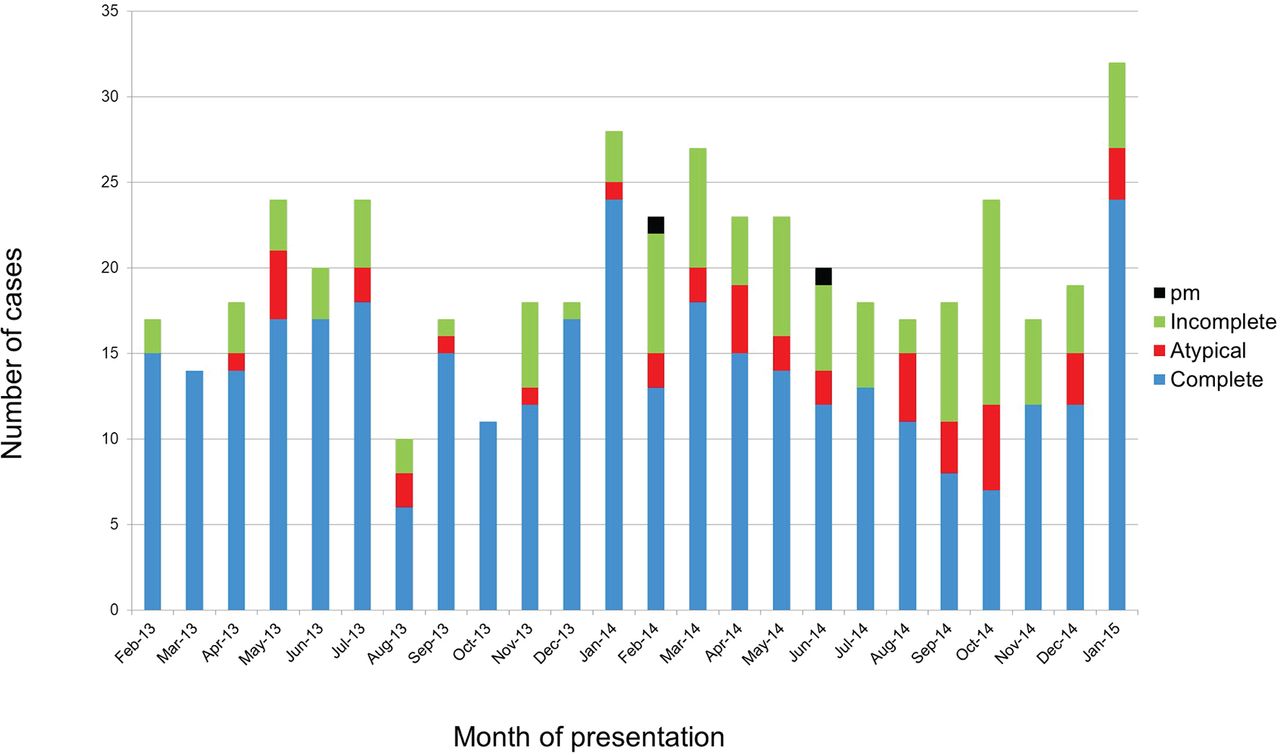
Incidence of Kawasaki disease by month at diagnosis showing breakdown into complete, atypical and incomplete cases. PM was diagnosis at postmortem.
Time to first point of clinical contact and diagnosis
Four hundred and forty-three (80%) children saw a general practitioner (GP) at a median (range) of 2 (0–27) days from the first onset of symptoms. The time from first GP consultation to hospital admission was 1 (0–32) days; the time from disease onset to formal diagnosis was 7 (0–36) days; and the time to diagnosis following admission to hospital was 1 (0–25) days, with 50 cases being diagnosed on day of admission.
We used the first four components of the postcode of patients in the UK to assign cases as resident in urban or rural areas and compared the proportion of cases occurring in rural or urban areas. Relative to the population density, we found significantly more cases occurring in rural areas (applying a non-linear cubic regression offered best fit with r2=0.867, F=30.290, p<0.005) (figure 2).

{kind=link}
{kind=link}
Plot of urbanicity (as assessed by population per postcode, per square kilometre) against the number of cases of Kawasaki disease.
Clinical features
Coronary artery status
The results of the initial echocardiograms were available for 523 of 553 children. There were 11 children in whom the weights and Z scores were missing, so these have been omitted from the analysis. Overall, 123 of 512 (24%) had abnormal coronary Z score (Z score >2) at echocardiography within 30 days of diagnosis. Of these, 95 of 512 had coronary Z score ≥2.5; thus, the overall CAA rate within 30 days of diagnosis was 19%.
In 25 children, there was a pericardial effusion recorded, and in 7 there was either valve regurgitation or depressed ventricular function. Taking these into account, the all-cardiac complication rate (coronary Z>2, or any other cardiac complication) was 28% within 30 days of diagnosis (table 2). It is of note that a much higher proportion of children under the age of 1 year had CAA+ (39%) compared with those over the age of 1 (13%, p<0.01). Overall, 8 of 512 cases (1.6%) developed giant CAA, and 4 of 86 cases (5%) under 1 year of age had giant CAA.
Echocardiographic data showing cardiac complications
Variables associated with CAAs
We reviewed the association of CAA status with features highlighted in previous publications (table 3) to determine whether there were any associations with CAA.24 25 In addition, we explored if there were any differences in coronary outcomes between 2013 and 2014 which may have been influenced by the publication of a new UK clinical guideline paper at the end of 2013.1 In 28 cases, we did not know the coronary artery status, and in both of the postmortem cases there were CAAs.
Association of coronary artery status with individual variables
The presence of fever plus four diagnostic features of KD at the time of diagnosis (complete KD) was associated with a lower rate of coronary artery involvement. Younger age at presentation, longer time to receive treatment, and presentation between December and May were all associated with increased risk of CAA. Additional factors associated with the presence of CAA were lower albumin and higher corticosteroid use in those with CAA (table 3).
Treatment with IVIG and aspirin
Excluding the two cases diagnosed after death and excluding the 20 cases with incomplete data, 502 of 531 received IVIG (95%), with the recommended dose of 2 g/kg (97%). Twenty-nine of 531 (5%) did not receive IVIG: 20 with complete KD, 0 with incomplete KD and 8 with atypical KD (one not classified). The usual reason for not giving IVIG was delayed diagnosis, but in one case the parents refused therapy (table 3). Anti-inflammatory dose aspirin (30–50 mg/kg/day, divided into four daily doses) was given to 472 of 537, while 41 did not receive any aspirin; data regarding aspirin were missing for the other cases. Following this, an antiplatelet dose of aspirin (3–5 mg/kg once a day) was given to 460 (83%) children. As shown in table 4, the proportion of patients with CAA was lowest in those treated with IVIG within 7 days of onset and increased progressively in the group treated between 7 and 10 days and above 10 days.
Association of time of treatment with intravenous immunoglobulin (IVIG) with coronary artery aneurysms
Adjunctive therapy
Overall, corticosteroids were used in 49 of 512 (10%) cases where CAA status was documented, either as primary adjunctive (4.6%) or as late rescue therapy (4.8%) (table 3). Infliximab was given to 10 of 551 cases (1.8%). Many children were commenced on antimicrobials (n=73) before the diagnosis of KD was made. No other treatments were reported.
Other outcomes
Of the 523 cases with echocardiography performed within 30 days of diagnosis, data on follow-up echocardiography beyond 30 days were available in 49 of 523, of whom 40 had persistent CAA. Overall, 8 of 49 had persistent giant CAA, including the 4 cases of giant CAA under the age of 1 year. Three had arthralgia, one had anaemia, one had hypertension and one had lethargy. In addition to the two cases who were diagnosed after death, a third child with pre-existing neurological disease died from intractable seizures, providing an all-cause mortality rate of 3 of 553 (0.54%), and mortality directly attributable to KD of 2 of 553 (0.36%).
Discussion
This prospective UK population-based study shows that the incidence of KD as reported by paediatricians in the UK and Ireland has risen since the last survey in 1990 (from 3.4 to 4.55/100 000 children under 5 years, with a male to female ratio of 1.51:1). It is noteworthy that estimates of KD incidence based on hospital admission or GP database statistics previously reported more than double the number of cases in our survey.8 26 This BPSU survey used rigorous diagnostic criteria to ensure accurate case inclusion. In contrast hospital admission data are not based on strict epidemiological KD case definitions, usually relying on diagnoses assigned by junior doctors or coding clerks, and are thus likely to significantly over-record KD cases. Conversely, the voluntary reporting system used by the BPSU could under-record cases, as busy paediatricians may not respond or recall all the cases or may believe their colleagues are doing the reporting. Therefore, our BPSU data are likely to provide a minimum estimate of annual incidence. Many features observed in this UK and Ireland study are also seen in studies from other countries, including the majority of cases being less than 5 years old, seasonal occurrence with more cases in winter and spring, and increased proportion of Chinese or Japanese Asians and black Africans relative to their proportion in the general population. We found an increased proportion of cases lived in rural areas relative to the population distribution. The early (within 30 days) all-cardiac complication rate for this unselected treated UK population was 28%; 19% had CAA at 6 weeks, based on a coronary Z score ≥2.5 (table 2). Worryingly, 39% of patients with KD under 1 year of age developed CAA despite IVIG, and the mortality rate at 0.36% was approximately tenfold lower than the last BPSU study.
We were surprised that residence in urban areas was associated with lower incidence of KD than rural residence. There might be many different explanations for this finding, including greater exposure to toxins used in farming, agriculture-associated micro-organisms or increased exposure to pollens.3 The suggestion that wind patterns could propagate triggers might be of relevance in this context.6
There was a change in the case ascertainment protocol from the first year of the study to the second. We were obliged by the BPSU reporting restrictions to have a small number of cases (less than 300 in each year), and there was concern that including all cases of KD would make the total number too large. However, it was clear, during the first year of study, that we were being notified of incomplete cases and that we were not going to exceed 300 cases per year. In addition, there was a new guideline that was published during the time of the study advising steroids in high-risk cases. We wished to capture both of these pieces of information. Clearly, the incidence of all cases of KD could therefore only be based on the second year of study. Despite this, we saw little difference in the demographics between the 2 years.
We found that the frequency of CAA (19%) is lower than the 29% observed in the treated cases in the original 1990 BPSU study,27 but significantly higher than CAA rates previously reported from other countries23 and comparable with reported coronary sequelae rates for untreated cases.1 17 This adds weight to our belief that the rise in observed incidence is not due to better case ascertainment, but due to a real increase in the number of cases and also case severity. Similarly high CAA rates have now also been observed in Sweden28 and Russia,29 with delayed diagnosis cited as a likely explanation for high coronary complication rates in the latter study. We found that the proportion with CAA was lowest in patients treated within 7 days, and this increased with later treatment. Our data therefore strongly suggest that delayed diagnosis and treatment is a significant factor contributing to the high incidence of CAA in the UK. Furthermore, the low numbers of patients receiving adjunctive treatments such as corticosteroids or antitumour necrosis factor, which are associated with more rapid resolution of inflammation and reduced CAA risk, suggest many UK patients with KD are not receiving optimal therapy advised in national and international guidance.1
Our study confirms that children under 1 year are more likely to have atypical KD and higher rates of coronary sequelae (39%), as reported in other series.1 Diagnosis of KD is difficult in the absence of all the typical features. As a high proportion of infants under 1 year of age do not fulfil the KD diagnostic criteria, there is a need for increased awareness of the possibility of KD in any infant with evidence of persistent inflammation (raised C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) or white cell count) and no response to antibiotics. In these infants, echocardiography is an urgent investigation required as part of the diagnostic work-up of suspected incomplete KD. A high index of suspicion is thus required, and early treatment with IVIG and additional anti-inflammatory agents, and referral to specialist units for suspected atypical KD cases in view of the high risk of CAA are advised. Our findings also support the previous suggestion that children under 1 year should be regarded as high risk for coronary sequelae,1 and therefore be targeted for more aggressive primary treatment. It is also of note that there was a higher rate of CAA in children in the second half of the study, after 1 February 2014. The most likely reason for this is that we included atypical KD in the second half of the study, which has CAA by definition.
Ninety-four per cent of children received IVIG in line with current guidance, along with high-dose aspirin in almost all, although as previously highlighted those children with CAA+ were treated later (median 10 days) than those without CAA (7 days), highlighting the importance of instituting treatment as early as possible (ie, not just within 10 days) to improve outcomes.30
Corticosteroids were only used in 10% of cases (table 3): 4.6% of cases as primary therapy and 4.8% as rescue therapy. This overall relatively low use of corticosteroids, combined with delay in initiating treatment, could explain the high CAA rates we observed, since a recent meta-analysis of 2746 patients has now demonstrated that early addition of corticosteroids is associated with reduced risk of CAA compared with IVIG therapy alone, particularly for high-risk cases (OR 0.424; 95% CI 0.270 to 0.665).30 Arguably, however, all UK patients with KD could be deemed ‘high-risk’, since 19% developed CAA within 30 days despite IVIG treatment, with even higher risk for children under the age of 1 year, of whom 39% developed CAA, and of which 5% had giant CAA with poor prognostic outcomes. We would have liked to have had follow-up on the CAA after 30 days, but we were obliged by our protocol approval by the BPSU and National Information Governance to keep this within the acute phase. We hope to be able to return to these patients and obtain ethical approval and consent for a follow-up study in the future.
Limitations
The BPSU methodology relies on busy doctors to complete data entry, and thus a surveillance-based study of this nature is limited since it is entirely dependent on the entry of data and case ascertainment for completeness. Therefore, although ours was a prospective study, it is expected that there will be a small proportion of cases that are not reported, as evidenced in a recent German study suggesting that up to 44% of cases can be missed.31 This will only serve to increase the incidence of KD above that in the present reported study. Also, by the nature of the BPSU study methodology, follow-up data examining late cardiac sequelae are limited.
Conclusions
KD has a rising incidence in the UK and Ireland, and cardiac sequelae are higher than reported for other countries despite most patients receiving IVIG therapy. Treatment delay is likely to have been contributory to high CAA rates. A future national UK comparative clinical trial of corticosteroids as primary adjunctive therapy for unselected patients with KD is now planned. In the meantime, GPs and paediatricians should be aware that treatment to completely ablate systemic inflammation as early as possible is required to prevent lifelong cardiac sequelae, and that the historic KD therapeutic adage of ‘treatment within 10 days’ is no longer fit for purpose.
Kawasaki disease (KD) case definition
Any infant or child up to the age of 16 years presenting for the first time in the UK or Ireland with fever of 5 or more days duration, plus 4 of the following (complete KD), or plus any 3 of the following (incomplete KD), or plus 2 or 3 of the following with coronary artery changes (atypical KD):
Conjunctivitis: bilateral, bulbar, non-suppurative.
Lymphadenopathy: cervical >1.5 cm.
Rash: widespread, polymorphous, not vesicular.
Lips and mucosa: red cracked lips, ‘strawberry tongue’, erythematous oral cavity.
Changes in the extremities: erythema, oedema of palms and soles initially, later peeling of skin.
References
Footnotes
Contributors RMRT, AH, RM-W, PAB and RML designed the project. Cases were assessed by the expert panel review (RMRT, RM-W, AVR, EJT, DS, PAB), and PC collected and recorded the data. SD provided patient participation support and informed families involved in the study of the ongoing progress. CAM, AH and ODF provided local support and assisted with recruitment. RM-W, RS and MD undertook statistical analysis.
Funding Kawasaki disease parent support group and discretionary institutional academic funds from each of the authors.
Competing interests None declared.
Ethics approval National Research Ethics Committee 11/SW/0310 and NHS Sponsorship CS/20113847.
Provenance and peer review Not commissioned; externally peer reviewed.