Article Text

Abstract
This article suggests communicative steps and strategies to help healthcare professionals achieve the ideals of child-centred care, which place children and young people at the centre of policy and practice. For those with 15 s, not 15 min, our suggestions can be summarised like this: help children be active agents in their own care by asking, listening well, being curious and explaining things clearly in an accessible but not condescending way.
- paediatrics
- child health services
Statistics from Altmetric.com
Introduction
‘Child-centred care’ (CCC) means centring our thoughts and actions on the children and young people (abbreviated to children) we care for.1 It means having the humility to be outsiders to their worlds and gaining the right of entry by being sensitive to and thoughtful about their experiences, perspectives and priorities.2 It means tailoring the care we offer to their needs. For care to live up to this ideal, we need to help children be active agents in their own care.3 This is easier said than done because power is unequally distributed in paediatrics: our status as adults with professional authority can prevent children from engaging authentically with us.1 This can make children overly obliging or distant rather than frank about their needs.
The need for child-centred communication has been on the political agenda for two decades.4 Clinical priorities take centre stage though, so any of us might still be caught ignoring or objectifying a child. Clinicians have tended to use biopsychosocial models to structure histories and frame questions.5 Although these models are useful, they rarely incorporate insights into how children experience communication. We, in contrast, want to help healthcare professionals (HCPs) express their latent child-centredness by practising, reflecting on and refining child-centred communication.
Clinicians’ basic humanity is the single most important ingredient of CCC. We have published some additional ingredients in the form of a philosophically guided analysis of more than 600 verbatim quotations from children.6–8 The article you are reading translates that rich qualitative synthesis, collated from patients aged 5–18 years, into generic principles (in the form of steps and strategies), applicable across the paediatric age range. We provide, also, concrete examples to showcase how you may exercise each step. We intend these to help you tailor your everyday clinical communication to a child’s age, level of development, illness and context of care.
Steps and strategies for child-centred communication
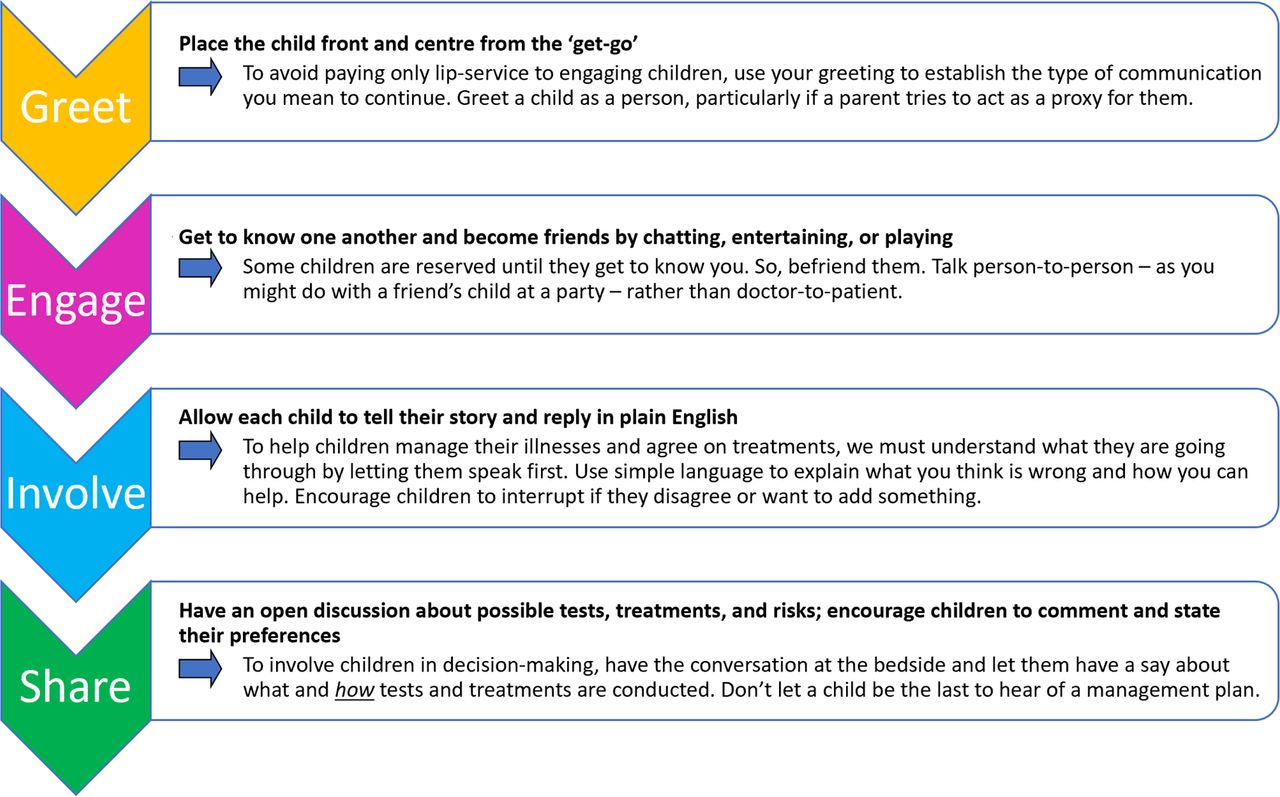
Figure 1 turns the principles of child-centred communication into four consecutive steps, which can help build trusting relationships that get children involved. The text then discusses each of these in greater detail. You can follow the steps in different orders depending on the situation you are in.

Four steps for child-centred communication (created by the authors).
Step 1: greet children
The following are the ways to achieve this:
Make and maintain good eye contact.
Use welcoming hand gestures, such as a wave (especially when wearing face masks).
Tailor speech intonations to individual children and circumstances. (An upbeat, friendly, tone of voice is usually appropriate, although highly distressing or emotive situations may require a softer approach.)
Check you are pronouncing a child’s name correctly. (This may also include, especially with older children, checking which pronouns they prefer.)9
Be patient.
Acknowledge, for example, that you have kept them waiting a long time.
How you introduce yourself—your name and title—is a personal preference, but children tend to remember first names better than surnames. First names also narrow the power gap between you and a child. Common sense dictates that the name you use should be easy for a child to understand, say and remember (“Call me Dr Debbie because nobody can remember my full name”). If children make any distinctions between job roles, they tend to make simple ones: for example, doctor or nurse. An example of how you might approach a child is shown in figure 2.
{kind=link}
{kind=link}
Exemplar approach to greeting children (created by the authors).
Toddlers and children who find it hard to communicate (eg, due to autism or learning difficulties) may disengage if they are put on the spot. To get around this, you could take a cautious, steady approach, use toys to spark their interest, and gauge their response. Arranging your consulting room to suit individual children’s needs and interests can help them feel more at home. Sometimes, it is not what you say, but how you say things—the words you emphasise and the way you move your body—that create meaning for children. This is more important when children have hearing difficulties or when a mask hides your face and muffles your speech.
Step 2: engage children
Our hospitals or health centres can be scary and unpredictable places, especially for children who are not used to them. But we can make places better, simply by being friendly. Chatting casually about non-medical things and playing help to make children happier and more relaxed and breaks down conversational barriers before you start asking about symptoms and concerns. It also builds friendships and trust, which is really important for children. We acknowledge that the idea of friendship between clinicians and children may challenge clinicians’ assumptions on the nature of relationships. It is quite different from traditional doctor–patient relationship models,10 but research shows this is reality for many children.7 11 12 They speak favourably about professionals who they come to know as friends, especially during long-term care. Friendship helps children open up about concerns and engenders trust needed for asking more intimate questions or performing unpleasant examinations.
Some of us might be a dab hand at small talk, while others may need a few cues. A child’s clothing or belongings, for example, may give you clues about their enthusiasms and interests and provide ‘conversation starters’. You can also establish common ground by saying a bit about yourself—your childhood, interests, family or other experiences. While getting to know children, we should, of course, respect professional boundaries,13 being careful not to divulge anything confidential or inappropriate. Some examples of ‘conversation starters’ and ‘common ground builders’ are outlined in table 1.
Tips for engagement: conversation starters and common ground builders
Children say that we are better at asking questions than listening to their answers. Pausing to hear what they say is only the first step. They want us to do more than listen passively. You can become an active listener by taking onboard what children say: pondering what a child’s experience (or lifeworld) is like and how their illness or healthcare affects them. You can show children you are listening by being responsive. Children will also like it if you are enthusiastic about their experiences and achievements.
You may be able to engage toddlers or less vocal children better by using age-appropriate activities. This is because doing something fun, together, reduces anxiety. Activities like playing (with toys, bubbles or play-dough), drawing, colouring, painting, singing (eg, Baby Shark or Doc McStuffins), role-playing (children using the stethoscope/pen torch or bandaging teddies) or reading activity books (eg, Usborne Publishing’s ‘Look Inside’ series or ‘Where’s Wally?’) can get two-way conversations flowing.
Step 3: involve children in conversations about their care
Even when we have engaged children in small talk, we are then inclined to turn to the parents to discuss the real business of problematising, diagnosing and managing the illness. This can make children feel left out and unimportant. Of course, we must listen to and respect parents, but parents might have a different take on the issue—possibly one that their child neither shares nor wants to contradict. Steps 1 and 2 can kick-start conversations with children, who may then clam up for fear of speaking freely, misunderstanding medical talk and looking silly. To provide CCC, we therefore need to help children be involved and participate, as far as they are happy to. Box 1 presents some suggestions. You may be pleasantly surprised by how much relevant information children can provide when given opportunities, and parents are usually willing to wait for their child’s response, corroborating the information and filling in important gaps in the history.
Suggestions for involving children in clinical conversations
Talk to children first and ask their permission: “May I ask you a few questions about why you are here today?”
Try not to arouse anxiety: “Don’t worry if you’re not sure. It’s not a test, so there are no wrong answers. […] Mum can fill me in if you’re not sure.”
Start with open-ended (easy) questions: “What has brought you here today?”, “How have you been feeling?” or “Tell me how I can help?”
Speak in a child-friendly way: use non-technical information or explain medical words, speak slowly, pause for a response, fully explain illnesses or treatments (using pictures, drawings or metaphors, where required), and listen. Visual aids or prompts providing step-by-step descriptions are especially useful for younger children.
Some children (older or more experienced) might use technical language when speaking with you. In this case, you might like to check their understanding of terminology, allowing you to pitch communication at their level.
Ask about other people involved in their care (general practitioners, pharmacists or paediatricians, for instance) or settings where difficulties may arise (such as in school, university or the workplace).
Ask permission to question parents, but advise children that they can interrupt: “Your mum might have some other things that she wants to tell me, so is it ok if I speak to her and ask her some questions? […] But, if there’s anything that you want to add or if there’s something that you don’t understand, then you can just interrupt.”
Try to avoid, where possible, conducting private conversations with parents without knowing a child’s information-sharing preferences.
When parents are providing information, involve children too. For example, Mum states “she vomited five times this morning.” Clinician looks at Sarah, makes eye contact, smiles and states, “that must have been awful Sarah, are you feeling any better now?”
Ask (in this case, Sarah) if there is anything she does not understand and if she has any questions or concerns, then thank her.
Step 4: share decision-making with children
Steps 1–3 will allow children to open up about their illnesses and concerns, giving us the best chance to make decisions together. For children to contribute meaningfully, you need to include them in every step, from start to finish. This may not come naturally. After all, our actions are guided by best practice guidelines, hospital protocols, decision-making tools, advice from experienced colleagues and other professional imperatives. The lay perspective of adults, though, can take the blinkers off clinicians and help them to rethink their professional decisions. Why then should we not let children (who can be more perceptive than adults) have a say? Children can be perceptive enough to spot when being involved tokenistically, so even if a course of action is unavoidable its outcome may be improved by partnership rather than diktat.
A child’s age and maturity can give you rough guide to how they want to be involved, but past experiences and personal preferences also play a part. Research has provided some useful additional guidance. Children describe two types of decision: technical ones, such as whether to proceed with a test or treatment, and practical ones, such as how the test or treatment should be carried out. Naturally, both are required. Children tend to look to their parents and HCPs for guidance on technical decisions but feel more confident making practical decisions independently. You can help children share decision-making, therefore, by facilitating discussions with parents, speaking about the practicalities of treatment (eg, the timing of procedures, form of medication or which vein you should take blood from) and asking their preferences. Box 2 offers some suggestions for practising sharing decision-making.
Suggestions for shared decision-making
Ask children if they fully understand clinical concerns or diagnoses.
Advise children what the options are, what treatments may involve, the pros and cons, and likely effects.
Try not to undermine trust by giving children absolute assurances which may not come true (eg, about how many attempts will be needed to perform a procedure or how much it will hurt).
Give children trustworthy information about what you are proposing, the likely benefits, problems that may arise and how these can be overcome.
Tell children how other children experienced a procedure, what worked best and how pain could be prevented or relieved (without, of course, divulging confidential information).
Make it a genuine choice by asking children’s preferences as early as possible and being open to adapting care based on individual needs and preferences (ie, timing, persons present, etc).
Advise children of your intentions (eg, personally overseeing procedures, recording preferences or communicating with colleagues) and of the limitations, where applicable.
Summarise for children what you have discussed: checking their understanding, emphasising key details, reiterating the plan you agreed with them and providing safety-netting advice.
Ask children if they have any questions.
Involving a child, listening attentively to them and identifying their wishes and needs can help them, their families and clinicians find the best course of action. Circumstances like administering a life-saving treatment or being concerned about a child’s safety may, of course, force you to act against their wishes because you judge it to be in their best interests. The General Medical Council’s guidance is helpful when this situation arises.14
Challenges in delivering child-centred communication
Our task, as children’s healthcare providers, is not an easy one. Our personal opinions about children’s rights and capability to shape their own care have an inevitable influence on how we communicate with them. Children’s views and preferences will undoubtedly challenge your preconceptions and the status quo of practice. Yet they can provide a unique perspective on children’s healthcare which you may find insightful and advantageous. There is evidence that parents’ preferences tend to be more conservative. They may prefer to protect their child from, for example, being told they have cancer or being involved in important treatment choices.15 Children, though, are very perceptive and pick up non-verbal cues and what adults do not say. If we keep them in the dark, they tend to think the worst. The authors’ opinion, backed up by evidence, is that keeping secrets from children is futile; it is better to be honest than make them think twice about trusting you again.7 15 16
Conclusion
You can overcome barriers to involving children in their own care and make your care more child-centred by practising, reflecting on and refining child-centred communication. You can do this by placing children at the centre of your practice: putting them first, listening attentively, embracing their world and speaking plainly about their care to support them in making decisions.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Christine McAleavy (RBHSC play specialist), in addition to Daire and Grainne Kielty (RBHSC patient and parent), for their comments and suggestions.
Footnotes
Twitter @GailDavison9, @richardlconn, @No twitter, @ProfTimD
Contributors GD wrote the first draft and managed the revisions. MAK, RC, AT and TD provided critical reviews and contributed to revisions. All authors read and approved the final version.
Funding This work was funded by the Charitable Funds Department, Royal Belfast Hospital for Sick Children, by award of a PhD Research Fellowship received by GD (grant number 71817005).
Disclaimer Funders had no direct involvement with conceptualisation or completion.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.