Article Text

Statistics from Altmetric.com
Introduction
Postmortem examination remains an important investigation in perinatal, infant and child deaths, with additional findings provided in 30–40%.1 Though additional investigations, including genetic testing, are now available, until recently the autopsy procedure had evolved little over centuries. However, the combination of advances in imaging technology, development of less-invasive sampling techniques and expansion of ‘omic’ approaches for fluid and tissue samples, together with reduction in parental acceptance of traditional autopsy are likely to change the way paediatric deaths are investigated.2 It is important that clinicians are aware of changes to postmortem practice, since requests for minimally invasive approaches from bereaved parents and religious communities are likely to become increasingly common. The aim is to appropriately consent for the investigation after death that will best answer the clinical question while being acceptable to parents. This article summarises current and future areas of paediatric autopsy research, including postmortem imaging, molecular biology and discovery-based laboratory approaches such as proteomics and transcriptomics.
Current challenges: evolution of the postmortem examination
Current trends in autopsy research focus on improving acceptability of the postmortem examination, empowering parents who do not accept traditional autopsy for various reasons. Postmortem MRI (PMMRI) shows the greatest promise, as part of a minimally invasive approach; PMMRI with placental examination and other adjunctive investigations (without incisions) demonstrates overall concordance with standard autopsy of >90%.2 PMMRI may be combined with laparoscopic examination to facilitate direct organ examination while minimising incisions. Although PMMRI can provide detailed images of internal structures, tissue is still required for some investigations, and its utility is greatest when combined with a less-invasive sampling approach.3
Developments in percutaneous ultrasound guided needle biopsy sampling may lead to truly ‘incision-less’ autopsy in combination with cross-sectional imaging, genetic and other laboratory studies. These alternative investigations will greatly expand the range of postmortem approaches available to pathologists, clinicians and families and ‘investigation after death’ will better serve to represent this future process (figure 1).

Schematic of current and future themes in postmortem research. Less-invasive targeted tissue sampling will remain important as the range of investigations broadens to include ‘omic’ techniques to further research poorly understood pathologies, for example, in sepsis-related deaths, where proteomic analysis reveals a change in the glycosylation profile of A1AT (red arrows) when compared with non-infective deaths. PMMRI, postmortem MRI.
Developments in postmortem imaging
Research imaging techniques such as high field (9.4 T) MRI and microfocus CT (micro-CT) may lead to step-changes in this field. These potentially allow improved investigation of early gestation miscarriages (<18 weeks’ gestation), in which current MRI cannot provide the necessary resolution for diagnosis.4 In addition, micro-CT has potential utility for ex vivo specimen imaging, where volumetric data sets facilitate virtual dissection and re-examination of organs, allowing diagnosis, teaching and review without need for organ retention. Such an approach may be comparable, or even superior, to traditional macroscopic examination, with the ability to evaluate structures in intact organs and provide accurate measurements (figure 2). Newer phase contrast (rather than density contrast) radiographic approaches are also being evaluated to allow rapid, high-resolution internal visualisation without the need for exogenous contrast or tissue preparation.
{kind=link}
{kind=link}
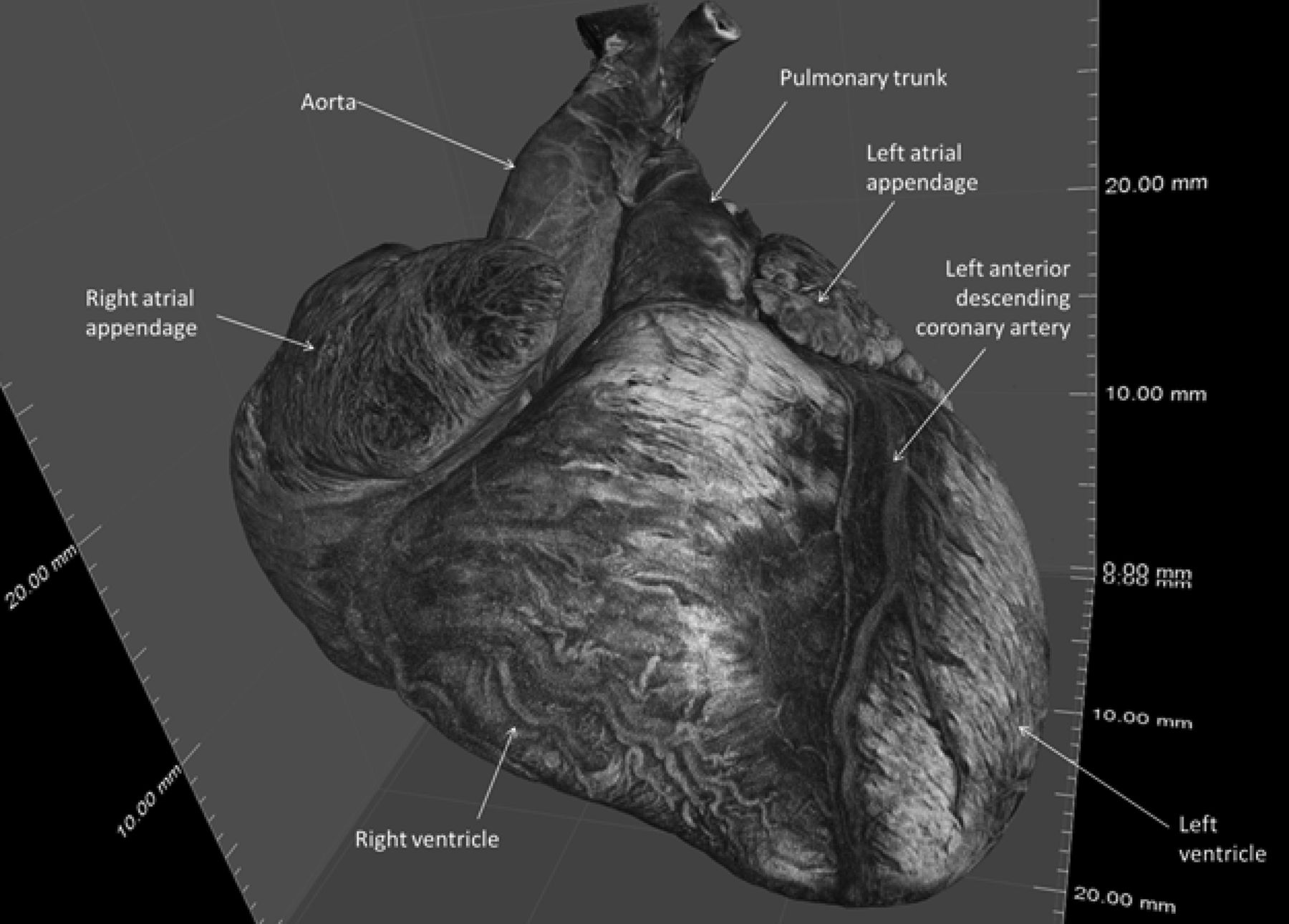
A micro-CT image of a normal 23 weeks gestation fetal heart (weight 5.1 g). The spatial resolution achieved is 21 μm. This facilitates demonstration of coronary artery anatomy without the need for injected contrast medium.
Research-led approaches and ‘omic’ techniques
Further progress in discovering the mechanisms of poorly understood conditions, such as sudden unexpected death in infancy and stillbirth, are unlikely to be made through continued conventional autopsy, but require novel tools based on ‘-omic’ technologies (genomics, transcriptomics, proteomics, metabolomics), since these potentially allow identification of non-hypothesis driven pathways and mechanisms.
To this end, biological samples obtained at autopsy will be increasingly required. The ultimate aim is that knowledge of such dysregulated pathophysiological pathways will lead to development of diagnostic tests for use in the living to prevent such deaths. For example, next generation sequencing (NGS) facilitates analysis of the entire human genome, and can be applied to investigate germ line, pathogenic and disease-specific processes, such as cancer. The UK 100 000 Genomes Project is an ongoing collaborative programme to evaluate genetic components of many rare diseases, including fetal and paediatric conditions, with increasing interest in developing methods of integrating data from genomics and other omic approaches.5 The potential availability of samples from multiple tissue types from the same patient means that postmortem cases may represent an important cohort for understanding organ and disease-specific genotype-phenotype relationships that are not available in life. However, appropriate interpretation of postmortem ‘omic’ data, accounting for changes occurring after death, will require studies of tissue-specific effects, representing a future distinct area of postmortem bioinformatics and biological research.
Finally, it should be emphasised that existing autopsy archives represent a unique and potentially hugely valuable source of material for many diseases, which can be interrogated by these new techniques. Technical developments in omic research are beginning to enable the use of this formalin-fixed paraffin-embedded material to ‘unlock’ this resource.
Conclusions
While the traditional ‘autopsy’ is in decline, many advances are being made in ‘investigation after death’, specifically incorporating imaging and less-invasive tissue sampling with development of novel investigations based on new laboratory techniques. These approaches are likely to be more widely accepted, and yield important novel data, which will ultimately lead to improved understanding of paediatric diseases and changes in clinical practice to prevent such deaths. Since paediatric and perinatal postmortem examinations represent the largest group of consented autopsies, paediatricians represent an important professional group discussing these developments with parents and obtaining consent for personalised investigation after death.
Acknowledgments
The authors are grateful to Nikon Metrology and Volume Graphics GmbH for their support. Nikon Metrology advised on acquisition and reconstruction of CT volumes. Optimal analysis and display of CT images was assisted by Volume Graphics GmbH.
Footnotes
Funding NJS is supported by an NIHR Senior Investigator award and OJA by an NIHR Clinician Scientist fellowship award (grant number NIHR-CS-012-002). NJS and JCH are partially funded by the Great Ormond Street Hospital Children's Charity and the NIHR Biomedical Research Centre at Great Ormond Street Hospital.
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Ethics approval Local Research Ethics Committee.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Epistle