Article Text

Statistics from Altmetric.com
In January 2020, the British Society for Paediatric Endocrinology and Diabetes (BSPED) published new guidance for the management of children <18 years with diabetic ketoacidosis (DKA).1 Fluid management is significantly different from their previous guideline2 and current National Institute for Health and Care Excellence (NICE) guidance.3 The 2020 guideline moved away from the concept of cautious fluid replacement towards a liberal approach for resuscitation and maintenance fluids. It recommends that all patients receive an initial 10 mL/kg bolus and those presenting with shock receive a 20 mL/kg bolus. Concerningly, delayed capillary refill time is used to define shock; however, in DKA this sign is confounded by hypocapnoeic vasoconstriction, which is common.4
A 20 mL/kg fluid bolus is also recommended for ‘reduced conscious level/coma’, without considering that this may indicate cerebral oedema which can be aggravated by additional fluid administration. Junior staff are enabled to give boluses of up to 40 mL/kg, contrasting starkly with NICE guidance, which recommends a single 10 mL/kg bolus only in those who are shocked. Full maintenance fluid is recommended in addition to replacing estimated losses, further increasing the volume of fluid administration. Figure 1 demonstrates the increase in 24-hour fluid administration, which is precisely the time when a child is at greatest risk of cerebral oedema. The percentage increase is greatest in younger patients who are again at the greatest risk. Cerebral oedema remains the leading cause of death in paediatric DKA, with a mortality of 25%. The pathophysiology of cerebral oedema is poorly understood, with debate as to whether it is due to hypoperfusion or fluid shifts. However, the likely exacerbating effect of rapid fluid administration was accepted previously by BSPED and NICE.5 Changes made between their 2009 and 2015 DKA guidelines prevented routine fluid boluses and reduced maintenance fluid rates significantly.

Comparison of potential fluid volumes administered over the first 24 hours to a child presenting with DKA. Assumptions are pH <7.1, 10% dehydration, and maximum fluid bolus administered as 10 mL/kg in the NICE guideline compared with 40 mL/kg in the new BSPED guideline. Total fluid administered (L) in 24 hours is shown on the left y-axis (BSPED and NICE guidelines), and fold increase in BSPED compared with NICE two fluid regimens shown on rightward y-axis (dashed line). BSPED, British Society for Paediatric Endocrinology and Diabetes; DKA, diabetic ketoacidosis; NICE, National Institute for Health and Care Excellence.
The BSPED guideline authors admit this ‘permissive’ regimen is ‘a significant change’, but has been recommended without presenting evidence for its benefit. The International Society for Pediatric and Adolescent Diabetes consensus guideline referred to by BSPED also concludes that current evidence is lacking.6 The Paediatric Emergency Care Applied Research Network (PERCAN) Fluid trial, comparing fast and slow rates of DKA rehydration in a population where the average pH was 7.2, showed no difference in neurological outcome between the regimens; however, concerns remain over the effect of administering more fluid in the sickest patients.7 Caution about overliberal fluid replacement has recently been raised in other settings; in fact, the current Surviving Sepsis fluid recommendations are now more conservative than the BSPED guideline.8
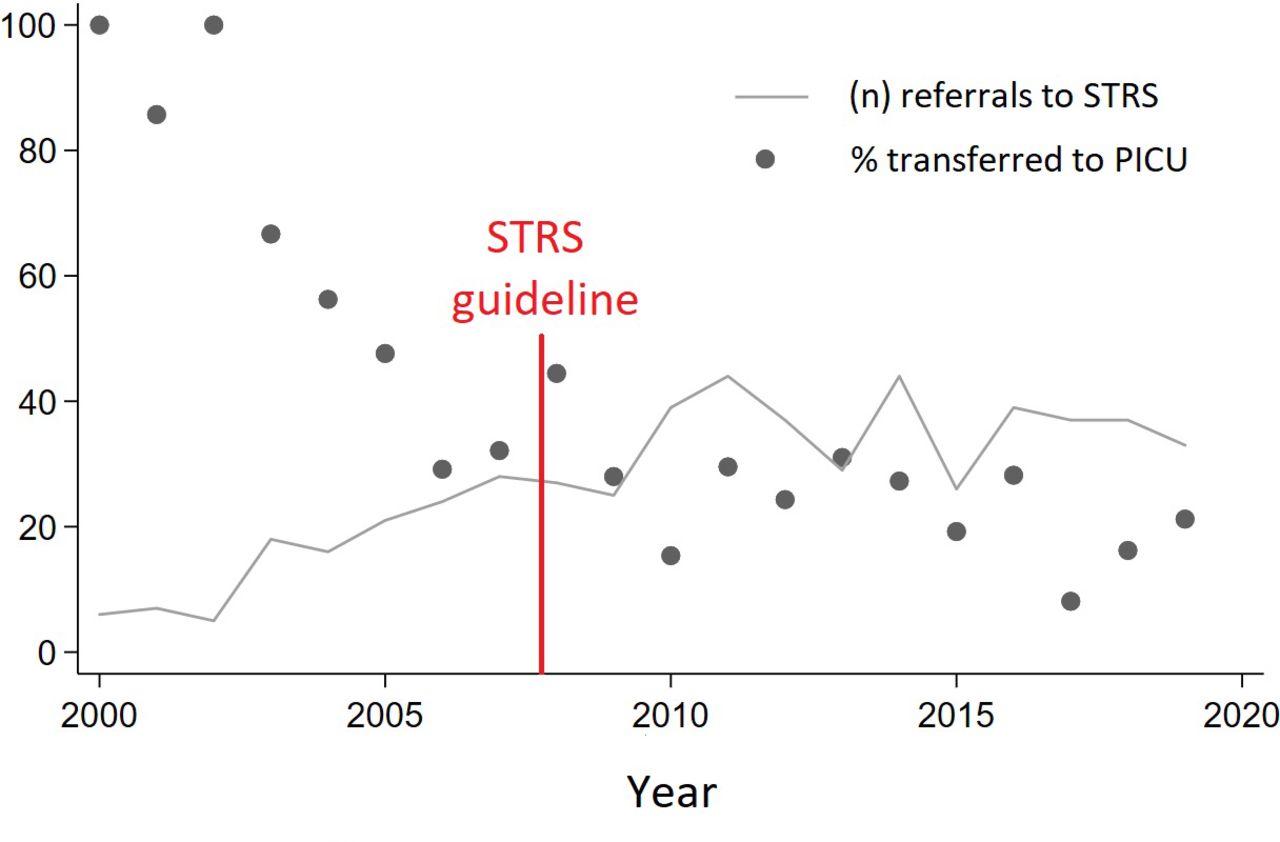
The South Thames Retrieval Service receives critical care referrals from 20 district general hospitals (DGHs) serving a population of 2.4 million children. Our 2008 ‘restrictive fluid’ DKA guideline9 was introduced following three deaths from cerebral oedema in our region (figure 2). Since this time the percentage of DGH DKA referrals requiring admission to intensive care has remained constant, at approximately 20% (figure 2), and there have been no deaths. Of note, the DGHs are now comfortable managing severe DKA (table 1), with the most common indications for paediatric intensive care unit (PICU) admission being lack of neurological response to osmotherapy, need for mechanical ventilation and suspected coexistent pathology (eg, sepsis). We have concern that the major differences in the new BSPED guideline will produce confusion and treatment inconsistencies for our referring clinicians, without apparent benefit.

{kind=link}
{kind=link}
Total annual referrals (line) and subsequent percentage requiring PICU admission (dots) for diabetic ketoacidosis to the South Thames Retrieval Service (STRS). PICU, paediatric intensive care unit.
Demographic, biochemical and therapeutic variables at presentation to the DGH, 2016–2019
Footnotes
Twitter @DrJonLillie, @docmcdevelina, @finegoulden
Contributors All authors contributed to the acquisition of DKA data for the South Thames Retrieval Service. All authors were involved in drafting or revising the letter and have given approval for this final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.