Article Text

Abstract
We used quality improvement (QI) methodology in the acute paediatric setting to develop clinical screening tools and local resources for addressing child poverty in practice in a London district general hospital between March and August 2019.
- social determinants of health
- professionalism
- social paediatrics
- quality improvement
- child poverty
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
Problem
Poverty is the most important determinant of child health in the UK, associated with adverse health, developmental, educational and long-term social outcomes.1 Acute hospital services are increasingly the site where poverty in families is encountered2—and yet clinicians often feel powerless, with training gaps and underdeveloped pathways leading to missed opportunities to help poor families address the social determinants of their health presentations.3
Although screening for social needs has proven valuable for certain age groups, including children during well-child visits,4 this is still not a widespread practice in the UK. Our baseline survey performed in March 2019, in district general hospital, serving a population with 21% of children living in poverty,5 revealed that no doctors or nurses in the acute paediatric unit asked about child poverty or signposted to relevant local resources.
Aims
By August 2019, for >80% of paediatric doctors in the paediatric assessment unit to discuss child poverty as part of routine clinical assessment and to signpost to local resources for child poverty when appropriate.
Making a case for change
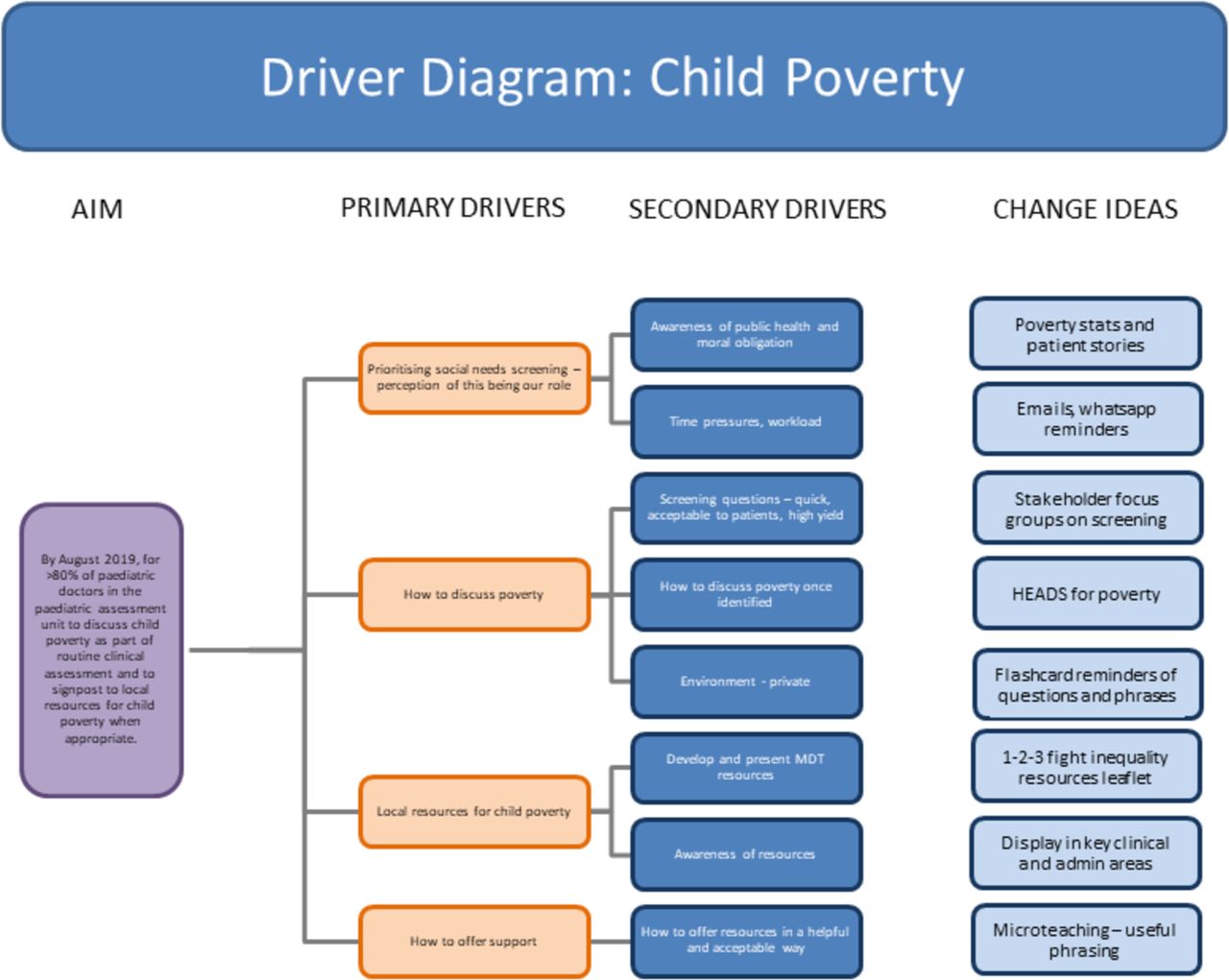
In our department, targeted training for social needs screening and social prescribing had not been developed; a strategy was needed to involve all the stakeholders in the process (families, nurses, doctors, social workers, family support workers and GPs) and to ensure clear communication and feedback of any improvements (figure 1). Through this process, we learnt that while most clinicians appreciated the importance of the social determinants of health,3 barriers to addressing poverty included not knowing how to ask, anxiety about offending families, not having helpful resources to offer, time pressure and the perception that this was not our role in acute paediatrics.
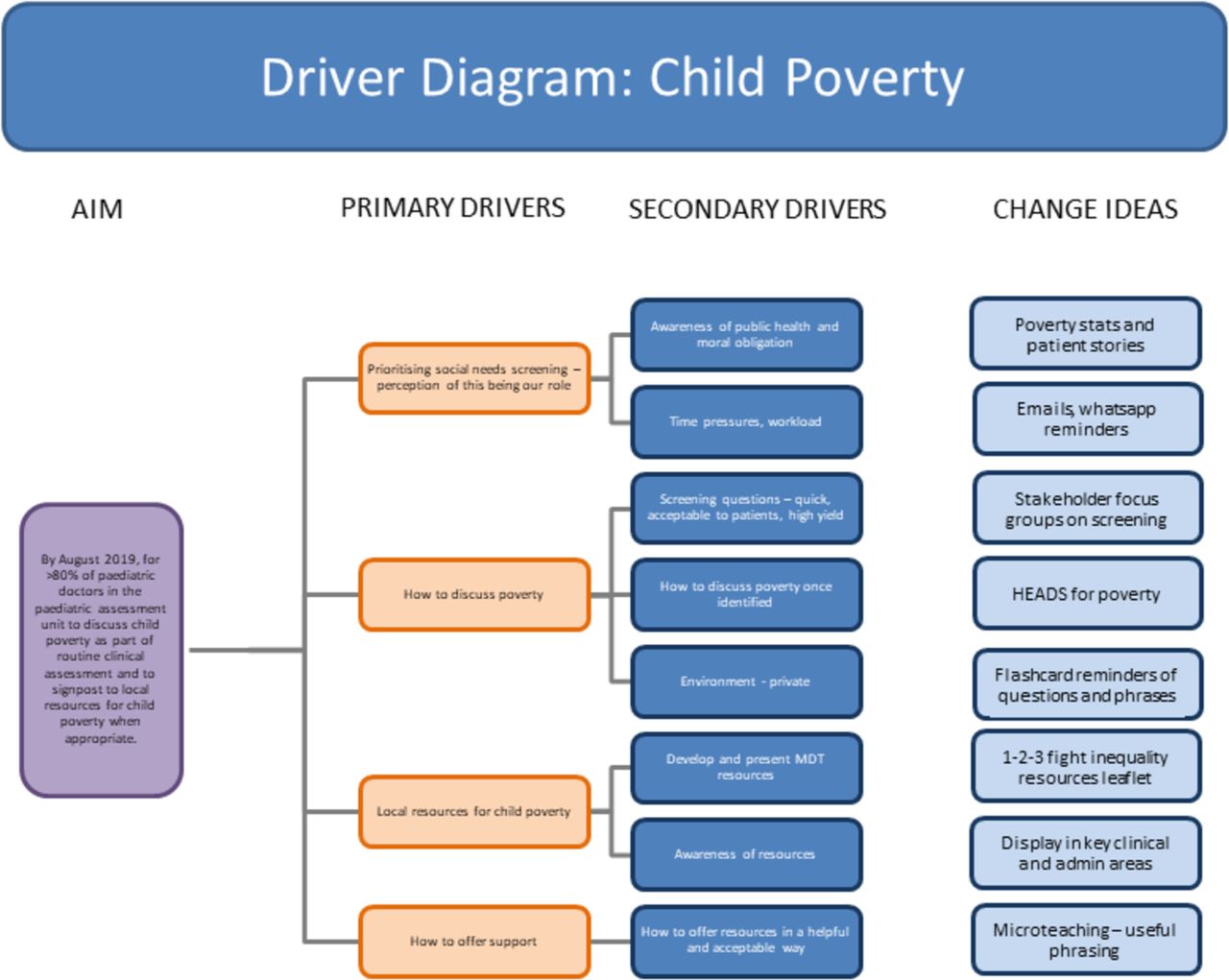
Driver diagram for addressing child poverty in clinical practice.
We engaged stakeholders in the paediatrics unit though multidisciplinary teaching sessions with key champions present at each session (senior nurses, advanced nurse practitioners, consultants). Through this process, we co-designed screening questions suitable for the local area and a ‘HEADS for poverty’ guide for discussing child poverty (table 1). We inserted questions into the existing HEADSSS model, an established tool for adolescent health discussions which expands the social history.6 We advocated that this could be used to frame a discussion about poverty and social determinants in families with children of all ages. Microteaching on poverty questions and local resources was delivered on each paediatric assessment unit shift to the team after performing our process measures. Our ‘HEADS for poverty’ guide and bespoke, local child poverty resources leaflet (figure 2) was emailed to the whole paediatric department and resources were offered to patients when appropriate.

Bespoke local child poverty leaflet with resources that increase income, provide essentials and improve participation.
Your improvements
Teaching sessions and plan-do-study-act (PDSA) cycles (table 2) tested questions and resource leaflets (figure 2) while improving stakeholder buy-in. Identification of child poverty increased from 0% to 89% in just 8 weeks, with resource awareness increasing from 0% to 100% in the same period (figure 3A–C). Qualitative patient feedback has been positive: “Felt cared for, I remember you—thank you so much for considering this part of our lives too.” “Thanks, this is great, our social worker never told us about these resources, great that we can do something ourselves.” “Thank you, this is so helpful.” "Oh yes, I heard of Relate, that will be really useful for X with everything going on and he finds it really hard since we split up.”
PDSA cycles

{kind=link}
{kind=link}
{kind=link}
A–C: Run charts showing progress in screening for child poverty, resource knowledge and number of resource leaflets given per shift. Number of doctors per shift=2–6.
Learning and next steps
While clinicians are busy and juggle many responsibilities, we can all play a role in helping families living in poverty. This QI project demonstrates how to ask about child poverty in routine clinical assessment and offer local resources to help families living in poverty, triggering referral to health visitors, school nurses and/or social services when appropriate. Signposting to local resources is the start of routine social prescribing; our aim locally is to formalise referral pathways with some key resources, such as food banks. Success of the project lay in engaging key multidisciplinary stakeholders early on and co-designing questions and resources with stakeholders who had lived in the local area for many years and understood the local population. An important learning point, demonstrated in the run charts, is the variability in screening depending on staff turnover (dips when new staff started at the hospital and when local champions are not around to ‘push’ the initiative). In addition, while our resources represent an improvement from what was available at baseline, we are fully aware that these are merely one solution to a problem which could be approached in different ways. In particular, we feel a more nuanced understanding of how clinicians ask about poverty and how these questions are received by families is needed, and is an angle that the authors are actively exploring in further QI work.
Despite the challenges of using QI to address the wider social determinants of health such as poverty, this project has generated much interest and shown great promise. From the initial starting site (Kingston General Hospital), this project has been trialled and developed in North Middlesex, Hackney and Newham, with different populations and different screening questions. Further work is required to better understand the contextual factors that can help or hinder such QI initiatives—not least the role of multidisciplinary and interprofessional working as well as integration between primary and secondary care, social care, education and the third sector—with a view to ensuring long-term sustainability.
Data availability statement
Data are available on reasonable request.
Ethics statements
Footnotes
Twitter @DrGuddiSingh
Contributors GS: conceived the idea for the project and supervised HZ, who implemented the project and collected data locally. GS and HZ co-wrote the article and both contributed to manuscript review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.