Article Text

Abstract
Positive blood culture is the gold standard for diagnosing bacteraemia and fungaemia, yet there is significant variability in aspects of performing and interpreting the test in children and neonates. Processing a blood culture can take several days, and includes use of semi-automated incubation with growth detection and a broad range of laboratory techniques such as Gram staining, phenotypic or molecular identification and antimicrobial susceptibility testing on a cultured isolate. Sensitivity and specificity of a blood culture and time-to-positivity depend on a number of factors related to host/pathogen interaction, collection and transport of the specimen to the laboratory and methods employed to process the specimen. Interpretation of a positive result relies on correlation of the identity of the cultured microorganism with the clinical assessment of the child.
- Microbiology
- Infectious Diseases
- General Paediatrics
- Neonatology
Statistics from Altmetric.com
Introduction
A blood culture is one of the most frequent diagnostic procedures undertaken in the unwell child or neonate. Although understanding of surrogate biochemical markers of sepsis, such as C-reactive protein, has improved, a positive blood culture, defined as the growth of microorganisms from a sample of a patient's blood, remains the gold standard for the diagnosis of bacteraemia and fungaemia.
Despite the universality of the taking blood cultures, there is significant variability in aspects of performance and interpretation of the test. Of importance are the technique of taking the blood culture, handling of vials after inoculation and the clinical interpretation of a negative or positive result. Contamination resulting in a ‘pseudobacteraemia’, where an isolate is actually from outside of the patient's blood stream, is a frequent problem and often results in unnecessary antimicrobial therapy, potentially resulting in toxicity, selection of resistance and complications related to line changes or repeated sampling.
This paper aims to provide a guide to the procedure itself, the transport of the specimen and the interpretation of a negative and positive result when aligned with the history and presentation of the patient.
Technological background
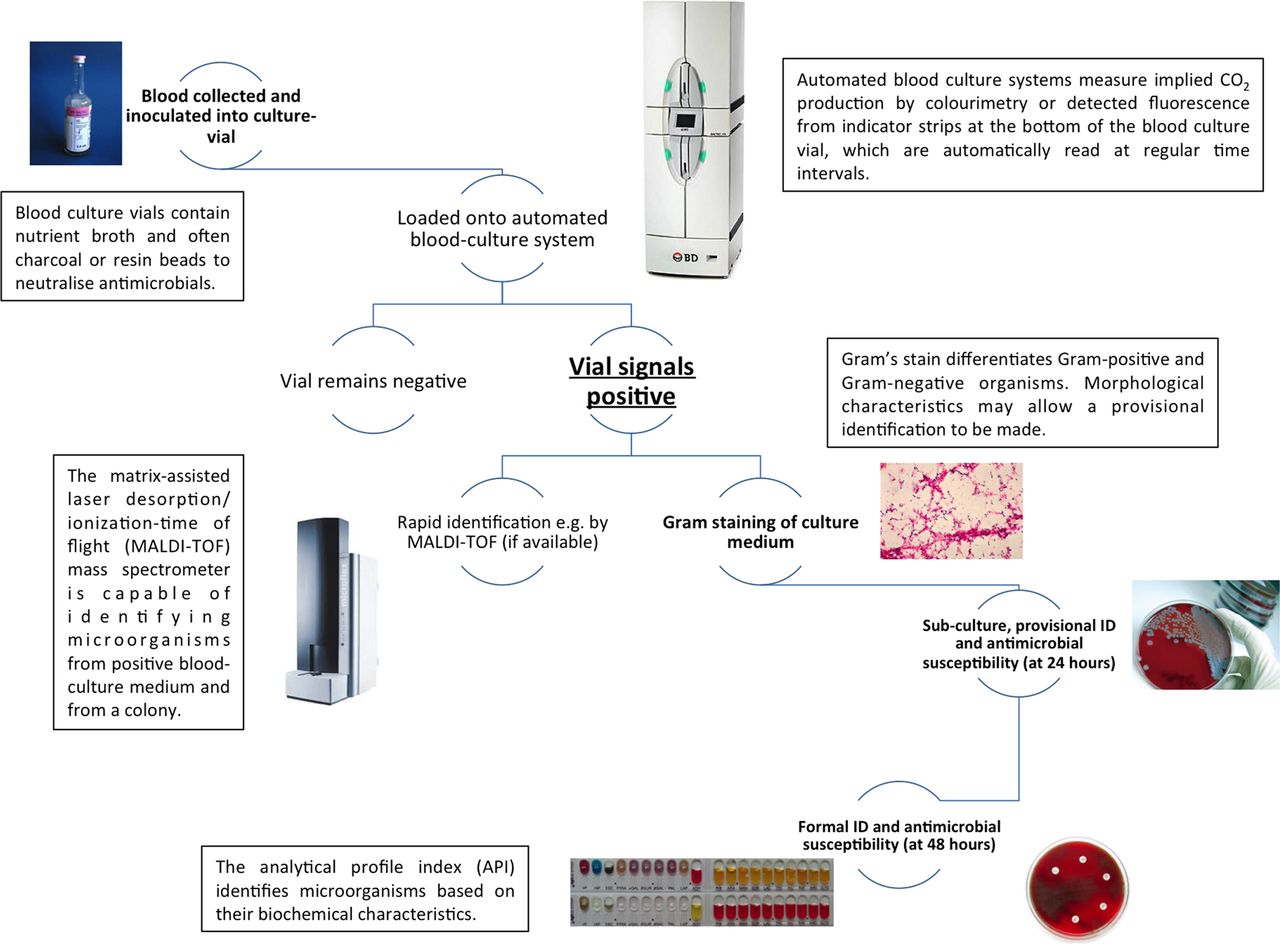
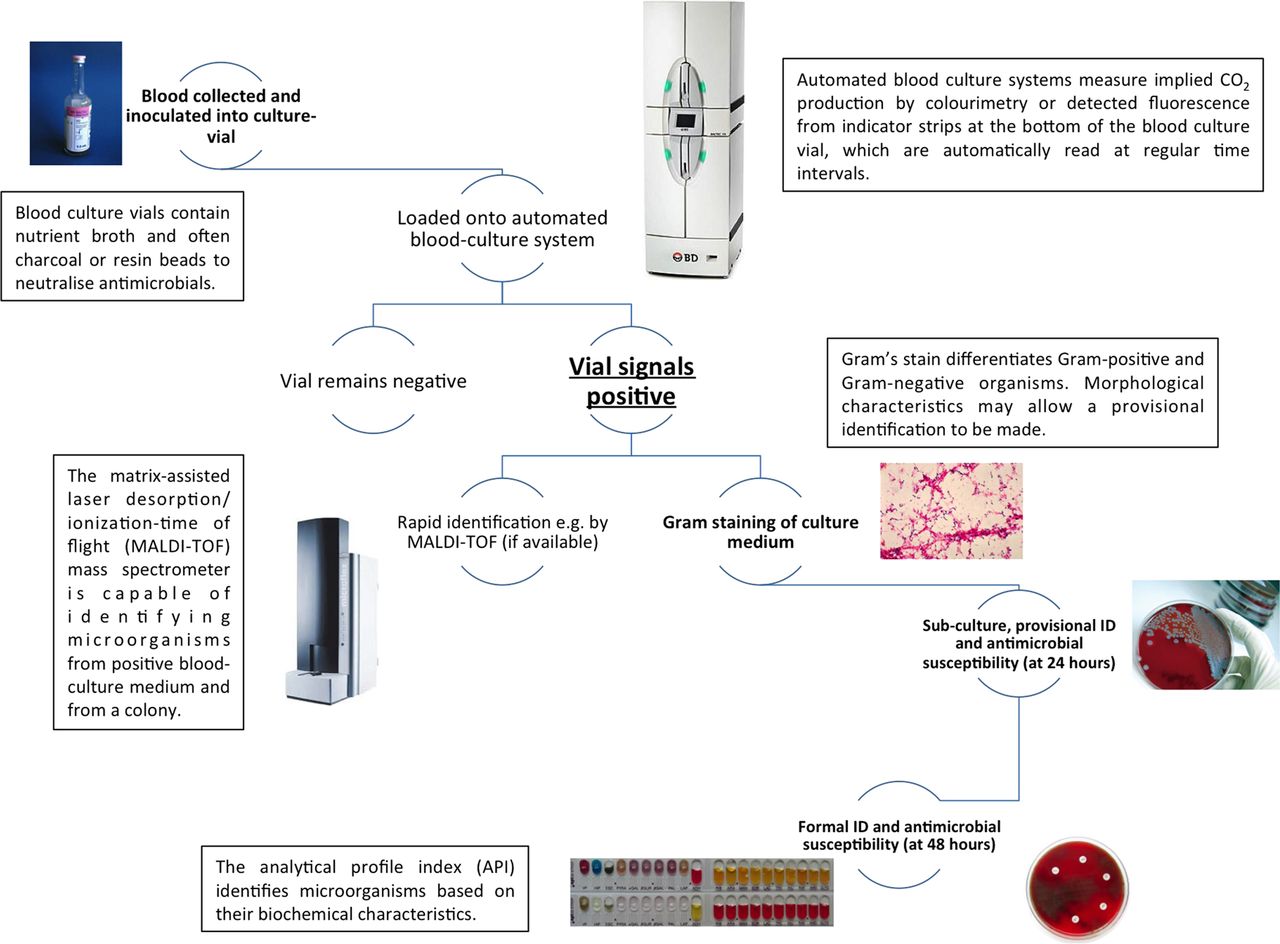
Most hospital laboratories in the developed world use automated, continuous blood culture systems, commonly the BACTEC (Becton-Dickinson, USA) and BacT-ALERT (bioMérieux, France) systems or variants. Blood culture vials, once inoculated, are loaded on to the system, where they are incubated and monitored for production of CO2 by the multiplying bacterial population. The system is designed to ‘signal positive’ when a predefined threshold of implied CO2 production, related to biological activity of the cellular components of the inoculum, is crossed. It is the change in CO2 concentration rather than the absolute value that is the trigger of positivity.
Once it has signalled positive, the vial is removed from the system and Gram's stain performed on a sample of the culture medium in order to differentiate Gram-positive and Gram-negative microorganisms. Additional characteristics such as morphology (cocci, bacilli or coccobacilli) and their arrangement (eg, pairs, clusters or chains) are used to further categorise the organism and may allow the microbiologist to suggest a possible identification (table 1). This initial investigation has clinical value in that it will guide empirical antibiotic therapy as early as 12 h after the blood culture was taken.1
Characteristics of microorganisms commonly isolated from blood culture
The blood culture medium is then subcultured on to agar plates, incubated further to provide sufficient bacterial cells to allow identification and antimicrobial susceptibility testing to be performed. The choice of which culture plates are used and which antibiotic assays are performed is determined by the result of the Gram stain. Direct identification and susceptibility of the organism from the broth culture using biochemical characteristics and antibiotic susceptibility plates can be attempted at this point. However, this is less sensitive than identification and susceptibility testing from a pure cultured colony of microorganisms.2 Using conventional methods, provisional susceptibility and identification may be available after 18–24 h, with definitive results usually available after 48 h. Rapid methods of identifying microorganisms using mass spectrometry and genome sequencing are becoming more widespread. For example, the matrix-assisted laser desorption/ionisation time-of-flight (MALDI-TOF) mass spectrometer is already being used in some laboratories to identify microorganisms directly from positive blood culture medium or from a cultured colony,3 although the clinical impact of this is unclear especially with regards to practice in paediatrics (figure 1).
{kind=link}
Algorithm for blood culture processing.
Physiological background
Most common pathogenic microorganisms, that is, bacteria, yeasts and atypical mycobacteria, can be cultured from standard blood culture vials. However, the widely used BACTEC Peds Plus/F (Becton-Dickinson, USA) vials cannot support the growth of strict anaerobes, such as some Clostridium and Bacteroides spp. A dedicated anaerobic vial is required to culture these organisms. Indications for additional anaerobic blood cultures in children include suspected septicaemia due to abdominal pathology, human bite wounds, oral mucositis, chronic sinusitis, sacral or perianal cellulitis.4 Another important indication is suspected neutropenic sepsis (especially when the child has received high-dose steroids that could mask abdominal signs and symptoms).5
Some important organisms such as mycobacteria may be difficult to detect by Gram staining and require special stains. If no organisms are seen in the initial Gram film, discussion of the clinical case with the microbiology team is warranted so that the appropriate techniques can be performed.
Clinical questions
In children with suspected sepsis, does taking of multiple blood cultures improve sensitivity?
Despite being considered the gold standard for the detection of bacteraemia/fungaemia, blood cultures vary in their sensitivity. This is determined by a variety of factors, including the volume of blood inoculated, preincubation of the inoculated culture vials before loading on to the automated monitoring system, the periodicity of the bacteraemia (ie, whether it is transient, intermittent or continuous), the organism causing the bacteraemia/septicaemia and its density in the bloodstream.4 ,6
This leads to the question of how many blood cultures need to be taken per episode to maximise the sensitivity of the test. In adults, multiple blood cultures per infectious episode have been found to yield maximum sensitivity, especially in the context of infective endocarditis.7 This finding is also supported in paediatrics and takes into account the reduction of sensitivity caused by small inoculation volumes.6 However, a study in neonates prospectively evaluating both early-onset sepsis (EOS) and late-onset sepsis (LOS) by taking two blood cultures from different sites found no benefit with this approach compared with a single blood culture.8 In the context of febrile neutropenia in paediatric oncology, repeating the blood culture even when an initial culture is negative may detect an additional 10% of cases of true bacteraemia.9
Although the taking of multiple blood cultures in general paediatrics and paediatric oncology may improve sensitivity, this has not been shown to be the case for neonates.
What is the optimal skin preparation before collecting blood cultures?
A systematic review, which included studies in paediatric and adult practice, concluded that the use of 0.5–2% chlorhexidine–alcohol-based skin preparation is superior to povidone-iodine aqueous preparations in reducing the rate of contamination of blood cultures with skin organisms. The authors also suggest that the role of alcohol is important with no superiority of chlorhexidine–alcohol demonstrated over other alcoholic preparations.10
There is concern regarding the potential irritant effect of chlorhexidine on the skin of neonates, with limited safety data available. A randomised trial in 344 neonates weighing over 1500 g found that skin preparation with 1% aqueous chlorhexidine was associated with a reduced rate of blood culture contamination compared with 10% povidone-iodine with no reported contact dermatitis when it was washed off immediately after the procedure.11 However, a small study of 20 preterm neonates (<32 weeks’ gestation) found that chlorhexidine was detectable in the serum in half of those who had a single skin preparation with 2% chlorhexidine gluconate before central venous catheter insertion, with no reported concurrent dermatitis.12 The clinical significance of this is not known.
In conclusion, using skin preparation containing chlorhexidine and alcohol before obtaining a blood culture reduces the risk of contamination with skin microorganisms, but more research into safety in the neonatal patient group is required.
Does a blood culture taken from a newly inserted peripheral catheter increase the risk of contamination compared with dedicated phlebotomy?
In adults, blood cultures drawn from a peripheral venous catheter are associated with a higher rate of contamination, leading to decreased specificity and positive predictive value.13 However, in paediatrics, taking a dedicated blood culture presents problems. First, it is not possible to use the vacuum mechanism within the blood culture vial to aspirate blood in neonates, infants and toddlers as the pressure rapidly causes collapse of the peripheral veins. Furthermore, it is good practice to minimise the number of invasive procedures performed particularly in the neonatal intensive care cohort in order to preserve the peripheral vasculature.
The practice of taking ‘open’ blood cultures from a newly inserted venous catheter is common in paediatric practice, but there is concern regarding a potentially higher rate of contamination of the culture with skin flora compared with blood cultures taken by dedicated phlebotomy. There is no specific evidence relating to neonatal practice, but the evidence in children is conflicting. A small study of 99 patients showed no difference between the rate of contamination of cultures taken in parallel through a newly inserted venous catheter compared with dedicated phlebotomy using a butterfly needle.14 This result was reproduced in a larger trial involving 940 patients based in an Australian paediatric emergency department (ED).15 However, a non-randomised study that analysed results from 2431 paediatric blood cultures taken in a Houston children's ED found a significantly higher rate of contamination from samples taken from a newly inserted cannula compared with dedicated phlebotomy over a 6-month period.16 A 2003 US trial conducted in a children's ED that involved over 4000 blood cultures demonstrated a significant decrease in the rate of contamination when they changed from a policy of venous catheter blood culture to dedicated blood culture phlebotomy.17
When possible, blood cultures should be taken by dedicated phlebotomy to reduce the risk of contamination. However, the utility of this practice in the neonatal setting has not been proven.
Does changing needles prior to inoculation of the blood culture vial reduce false-positive findings?
The so-called ‘double-needle’ technique of collecting a blood culture, where the phlebotomist changes the needle after venipuncture before inoculation of the blood culture bottle, is associated with an increased risk of needlestick injury,18 but perceived to reduce contamination rates. A meta-analysis study showed a small but statistically significant decrease (1.25%) in the rate of contamination of blood cultures using a double-needle technique compared with a single-needle technique.19
However, most healthcare organisations’ occupational health policies mandate that healthcare professionals do not re-sheath and change needles because of the risk of needlestick injury, and the authors of this review share this view.
What is the optimal amount of blood that one should inoculate into the blood culture vial?
The yield from small blood volumes obtained in paediatric practice is affected by multiple factors, including the blood culture system used, the type of nutrient media in the vial, the organism causing the bacteraemia and the dilution factor.
Dedicated paediatric blood culture vials are often enriched in order to accommodate small volumes of blood. The manufacturer of BACTEC Peds Plus/F culture vials recommends that 0.5–5 mL of blood may be inoculated into the bottle, with an optimal volume being 3 mL.20 Any less than 0.5 mL may reduce sensitivity, especially of fastidious organisms, such as Haemophilus spp. Moreover, there is an increased risk of contamination with smaller blood inoculums.21
Evidence on how much volume of blood is required is conflicting. A Mexican study that divided a 2.2 mL draw into 2 and 0.2 mL aliquots found the smaller volume had a 95% sensitivity and 99% specificity for detection of bacteraemia.22 However, the dilution factors of the two volumes were maintained and the blood culture system used differs considerably from those used elsewhere. A group working in a children's ED found significantly reduced sensitivity with a 2 mL compared with a 6 mL draw of blood for culture.6 However, the vials that were used are not directly comparable to the enriched paediatric vials used in today's practice.
An in vitro study that evaluated blood spiked with known concentrations of pathogens showed that blood with a load of <4 colony-forming units per millilitre (cfu/mL) had a significantly decreased chance of being detected if the volume of blood was less than 0.5 mL. In the case of an Escherichia coli ‘bacteraemia’ with a load of 4 cfu/mL, a 0.5 mL draw would only have an 81% chance of being detected by a BacT/Alert system. The authors of the study suggested a draw of 1–2 mL would probably lead to greater sensitivity for detection of bacteraemia.23 One study reported that bacteraemia-associated group B streptococcal sepsis may have a higher bacterial load compared with sepsis caused by Gram-negative organisms and enterococci.24
Excessive volumes of blood inoculated into the vial may also reduce sensitivity due to the inhibitory action of a large volume of blood relative to broth.25
Based on current evidence, inoculation volumes of 1–3 mL of blood into a paediatric blood culture vial are optimal for detecting significant pathogens. Lower or higher volumes may compromise sensitivity and specificity of the test.
In a child with suspected sepsis who is clinically improving on intravenous antibiotic therapy, after how long an incubation period can a culture be considered negative?
The administration of empirical antimicrobial therapy for suspected or presumed sepsis, once a blood culture has been taken, is accepted good practice. Given the majority of blood cultures will show no evidence of bacterial growth,26 after how long a negative incubation period can antimicrobial therapy be stopped, assuming that the child has made a clinical improvement and there is a preferred alternative diagnosis other than bacterial or fungal sepsis?
Conventional wisdom states that the majority of blood cultures will signal positive before 48 h’ incubation. A study carried out in 1979 found that 96 and 98% of significant neonatal bacteraemias will be detected at 48 and 72 h, respectively.27 A subsequent study that analysed results from over 3500 blood cultures using the PedsBacT/Alert system found that the time to positivity (TTP) varied by organism and whether EOS (<48 h of age) or LOS (>48 h of age) was being evaluated. Blood cultures that yielded group B Streptococcus (GBS) and E coli had the shortest TTP (median 9.3–11.3 h). Those that grew Staphylococcus aureus had a slightly longer median TTP of 17.6 h with coagulase-negative Staphylococcus (CoNS) and Micrococcus spp. having the longest TTP (median 28.9–34.8 h). EOS tended to have a shorter TTP compared with LOS, median 13.7 and 17.2 h, respectively; the reason for this was not clear. The authors concluded that 36-h incubation was sufficient for blood cultures evaluating early-onset neonatal sepsis, but in LOS, a 48-h incubation period should be maintained before cessation of antimicrobials could be considered.28 However, the evidence is conflicting; another study using the BacT/Alert system showed a less pronounced difference between TTP in EOS and LOS. The authors suggest that it would be safe to discontinue empiric treatment of Gram-negative organisms, rationalising treatment so that cover is provided for Gram-positive organisms only if blood cultures remain negative at 48 h. They recommend incubating blood culture vials for 72 h before antibiotic therapy is stopped. This is based on the evidence that Gram-negative organisms had a significantly lower median TTP compared with Gram-positive bacteria. However, in a patient with early onset disease, the time taken to yield a positive GBS result did not exceed 24 h in any of the cases in the study.29
The TTP is also affected by the volume of blood inoculated into the culture vial with longer incubation periods required for smaller samples.6 ,23
It is important to emphasise that TTP refers to the period after which the culture vial is loaded on to the automated system and not from the time of collection; samples collected ‘out of hours’ are often not processed until the next morning. Furthermore, blood cultures taken at one site and then transported to a centralised laboratory could significantly increase the time in transit, further delaying the onset of incubation.
In conclusion, the TTP is affected by many factors, but an incubation time of 36 h for early-onset neonatal sepsis and 48 h in most other settings without detectable growth appears to be safe based on current evidence. If the child has additional risk factors for sepsis with Gram-positive organisms other than GBS (box 1), a longer incubation period (72 h) may be advisable before bacteraemia can be excluded.
Clinical questions when assessing significance of coagulase-negative Staphylococcus (CoNS) or α-haemolytic streptococcus (AHS) in a blood culture
-
Does the child have ongoing clinical symptoms/signs/laboratory markers of sepsis?
-
Is the organism a likely pathogen in the clinical context? For example, CoNS and AHS would be unlikely pathogens in the context of a urinary tract infection.
-
Does the child have an implanted indwelling vascular catheter or other medical device?
-
Has the organism been isolated from more than one set of blood cultures or from multiple sites?
-
If so, is it the same species on all occasions?
-
-
Is the child in a particular at-risk group, that is,
-
Oncology patient
-
Haematopoietic stem cell transplant recipient
-
Burns patient
-
Very low birth weight (<1500 g) infant
-
Does preincubating blood culture vials make any difference to the TTP?
Although it is advisable to load the blood culture vial on to an automated system as soon as possible after collection, many laboratories do not operate a service where this is possible 24 h a day. Therefore, it has become practice in some centres to preincubate blood culture vials soon after inoculation in an unmonitored incubator at 35–37°C during the interval time. This has been shown to reduce the TTP of the blood culture and the time to reporting a positive Gram stain result.30 ,31 However, automated blood culture systems detect change in CO2 to indicate growth as opposed to the absolute concentration. The concern is that the CO2 level may have plateaued by the time the blood culture vial is loaded on to the machine and a positive result may be missed; the rate of false-negatives is as high as 4% with preincubation.31 Visual inspection of the preincubated bottles for signs of growth on receipt in the laboratory was not useful, with only a 50% sensitivity in detecting a positive culture result.30
On a practical level, if an out-of-hours biomedical scientist were processing an urgent cerebrospinal fluid or other specimen on a patient, it would not be unreasonable to request that the blood culture vial taken concurrently be loaded on to the system at the same time.
Another approach is to train non-microbiology healthcare staff to load the blood culture vials out of hours. This has been found to reduce turnaround times and directly influence clinical decisions in an adult study population.32
Preincubating blood culture vials in unmonitored incubators may decrease the TTP but comes at the price of reduced sensitivity. The utility of placing monitored incubators at the point of care is yet to be evaluated in paediatrics.
When can one disregard a CoNS or α-haemolytic Streptococcus grown from a blood culture?
When evaluating a blood culture that has grown CoNS or α-haemolytic Streptococcus (AHS), factors that increase the likelihood of a true bacteraemia need to be considered (box 1). If the answers to those questions are all negative, then the organism is more likely to be a contaminant and may be disregarded.
Multiple species of CoNS are known to colonise humans as part of the normal regional flora. They are the most common contaminants of blood cultures and yet are the most frequent cause of bacteraemia in neonates in England.33 These organisms secrete an extracellular polysaccharide, which enables formation of a biofilm on indwelling medical devices such as intravascular catheters and other prosthetic material.34
Non-pneumococcal AHS are the second commonest contaminants of paediatric blood cultures.35 In the absence of the risk factors above, these organisms are most likely to have their origins from the skin. An exception is Streptococcus mitis, which is not part of the regional skin flora and has been associated with serious neonatal infection.36
When the diagnosis of true bacteraemia is in doubt, an acceptable strategy is to repeat the blood culture; some definitions of CoNS sepsis require two separate blood cultures of the same organism for diagnosis.37 However, evidence suggests that the number of positive CoNS blood cultures does not generally affect management and diagnosis is still predominantly based on the clinical assessment.38
Topics for further research
-
The utility of taking blood cultures from newly inserted venous catheters compared with a dedicated venipuncture and investigation of the efficacy and safety of skin preparation formulations, specifically in the neonatal patient group.
-
The utility of techniques to rapidly identify microorganisms from a positive blood culture medium specifically relating to children and neonates; does it make a difference clinically?
-
Inserting blood culture vials directly into a monitored incubator at the point of care; does it make a difference to outcomes in the paediatric population?
-
The utility of other methods such as genome detection directly on clinical samples to replace blood culture as the gold standard for detecting sepsis.
Clinical bottom line
-
Sensitivity and specificity of blood cultures depend on many factors. Taking repeated cultures in infants and children may increase sensitivity, but this has not been shown to be the case in the neonatal age group.
-
In the context of suspected septicaemia in paediatrics, blood culture by dedicated phlebotomy with chlorhexidine–alcohol skin preparation is the optimal method for maximising sensitivity and reducing rates of contamination, respectively. However, the utility of dedicated phlebotomy relating specifically to neonates is yet to be clarified.
-
Double-needle technique of inoculating blood culture vials should be discouraged despite a possible small increase in the risk of contamination associated with direct inoculation.
-
An inoculation volume of 1–3 mL of blood into a paediatric blood culture vial is optimal for detecting significant pathogens. Lower or higher volumes may compromise sensitivity and specificity of the test.
-
Time to positivity for most significant pathogenic organisms is usually less than 24 h, but this should not be relied upon given variability due to technical aspects of sample collection and handling. A negative blood culture at 36-h incubation to guide cessation of antibiotic therapy for early-onset neonatal sepsis and 48 h in most other settings appears to be safe.
-
Preincubating blood culture vials in an unmonitored incubator reduces time to positivity and reporting but also reduces sensitivity of the test.
-
Interpretation of the significance of coagulase-negative Staphylococcus and α-haemolytic Streptococcus in a blood culture remains a challenge and should be based on the clinical condition and risk factors for significant infection. When considered significant, the organism should be identified.
Test your knowledge of blood cultures in paediatrics
-
Which of the following statements are true regarding blood cultures?
-
A blood culture with no detectable growth after an incubation period of 36 h is sufficient to exclude late-onset neonatal sepsis.
-
Group B Streptococcus is the commonest organism isolated from neonates with early-onset sepsis.
-
Streptococcus mitis is a common contaminant of blood cultures from neonates.
-
‘Gram-positive cocci in clusters’ cultured from blood are always contaminants.
-
In children with indwelling central venous catheters, taking paired line and peripheral cultures increases sensitivity of detecting true bacteraemia.
-
-
Of the following options which is the optimal volume of blood to be inoculated into a paediatric blood culture vial to maximise sensitivity of the test?
-
0.2 mL
-
0.5 mL
-
3 mL
-
10 mL
-
-
Which of the following statements are true of the technical aspects of blood cultures?
-
The time to positivity is the time from specimen collection to the blood culture signalling positive.
-
Strict anaerobic organisms can be cultured in BACTEC Peds Plus/F bottles.
-
Preincubating blood culture vials in an unmonitored incubator reduces sensitivity of the test.
-
It is possible to definitively identify an organism directly from blood culture medium that has signalled positive using current techniques.
-
Mycobacteria may not be detected using Gram's stain.
Answers are on page 151.
-
Answers to the quiz on page 150
-
Question 1: A (F), B (T), C (F), D (F), E (T).
-
Question 2: C (T)
-
Question 3: A (F), B (F), C (T), D (T), E (T).
References
Footnotes
-
Contributors SD drafted and revised the paper. NS and MK revised the draft paper.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.