Article Text

Abstract
Objective: To devise a physiology-based scoring system for assessment of children presenting to the emergency department (ED) and to validate the system retrospectively.
Study design: Age-dependent physiological parameters designed to reflect the cardiovascular, respiratory and neurological status of patients presenting to the ED were included in a scoring system called the Paediatric Advanced Warning Score (PAWS). A retrospective pilot evaluation was performed to validate PAWS.
Setting and patients: PAWS scores were calculated retrospectively for 46 consecutive children who required admission from the ED to the paediatric intensive care unit (PICU) and for 49 control children who were admitted from the ED to the general paediatric ward.
Main outcome measures: To validate the PAWS score, we determined if this score was able to identify patients who require admission to the PICU and were therefore significantly unwell.
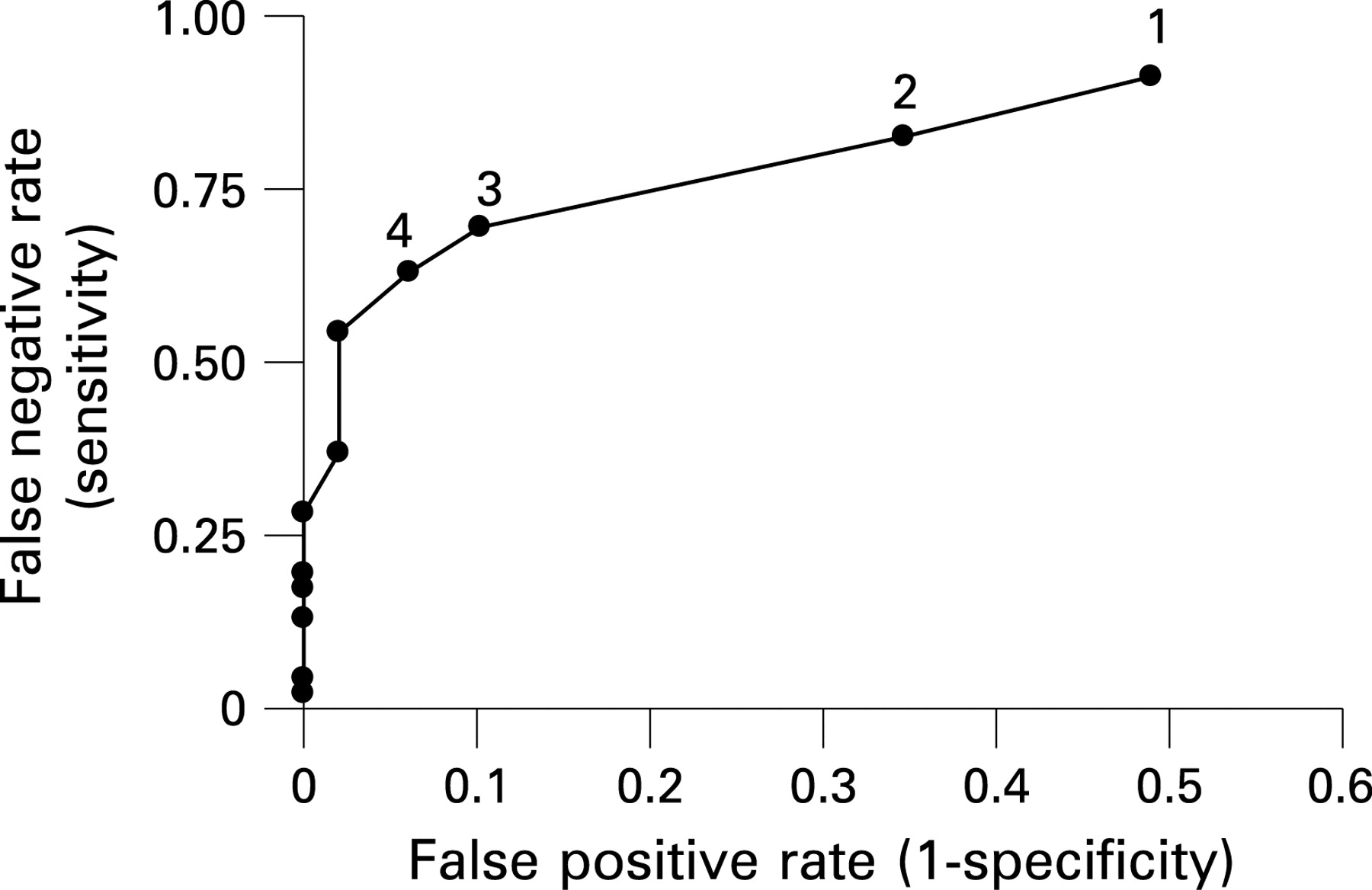
Results: The PAWS score area under the receiver operating characteristic curve was 0.86. Using a trigger score of 3 or above, PAWS was able to identify patients requiring PICU admission with a sensitivity of 70% and a specificity of 90%.
Conclusions: This pilot study has shown that a physiology-based scoring system can help to identify children in the ED requiring PICU admission. Future prospective validation of PAWS is necessary to assess its ability to identify all children in need of urgent assessment in the ED.
Statistics from Altmetric.com
The use of early warning scoring systems has become commonplace over recent years. This is reflected in the recent NICE guidance on acutely ill patients in hospital.1 Evaluation of such systems has taken place in clinical settings such as adult acute medical admissions units,2 postoperative surgical wards3 and, more recently, the emergency department (ED).4 5 Existing paediatric early warning scoring systems have concentrated on hospitalised patients6–9 and may be less useful for initial assessment in the ED. The aim of this study was to design and validate a scoring system to identify children attending the ED in need of urgent medical assessment and appropriate intervention.
METHODS
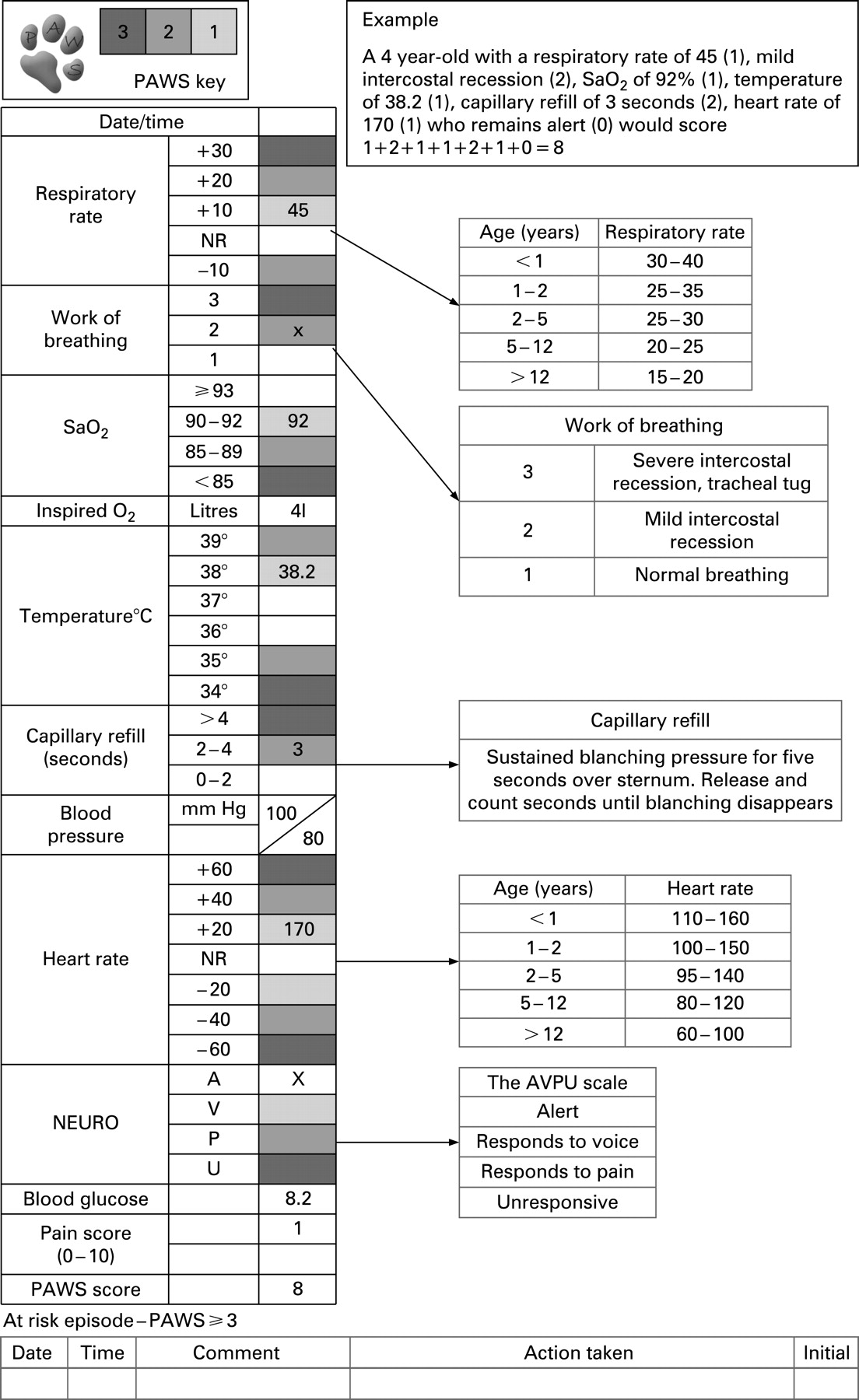
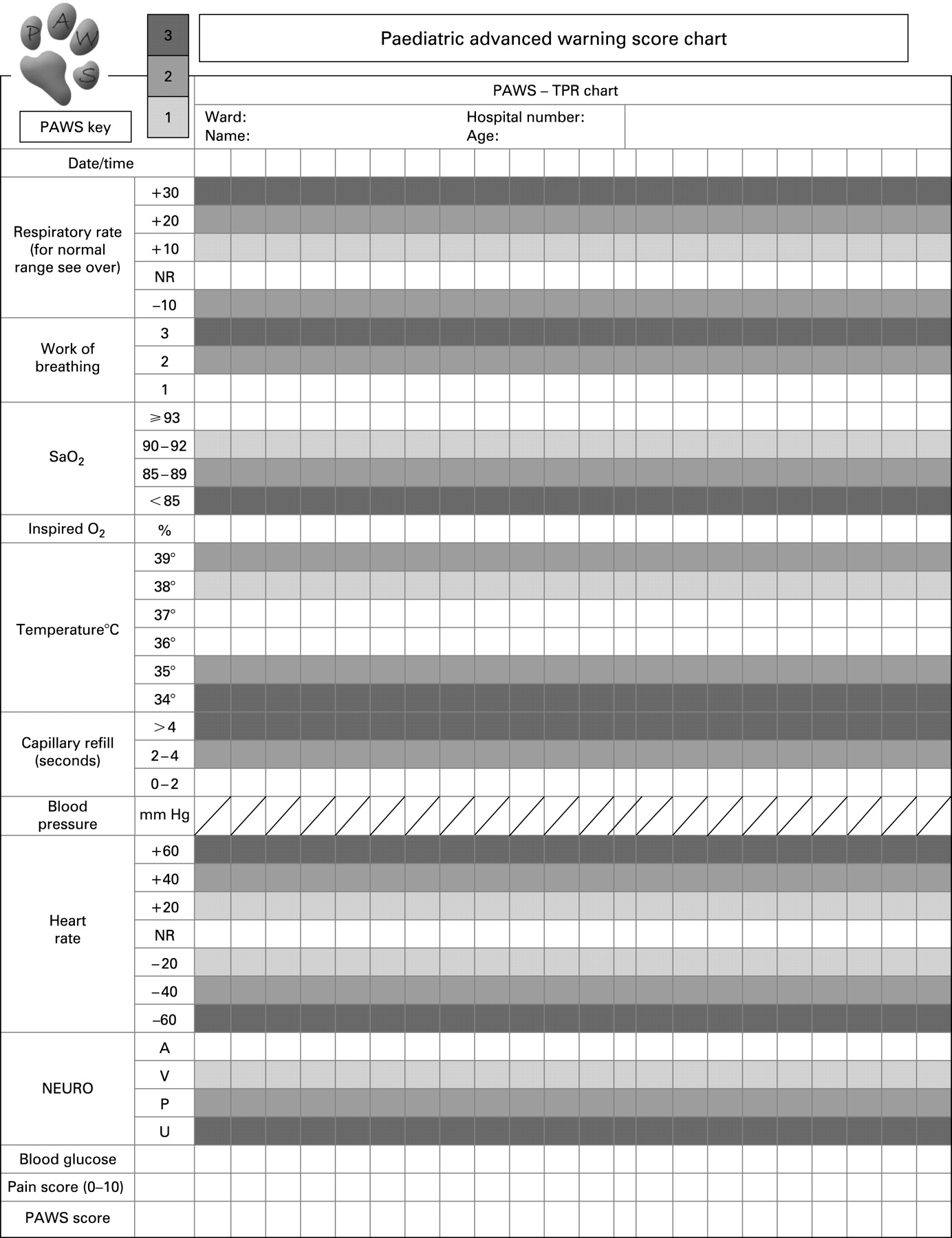
A Paediatric Advanced Warning Score (PAWS) chart was designed. The chart uses physiological parameters (respiratory rate, work of breathing, oxygen saturation, temperature, capillary refill, heart rate and conscious level), taking into account age-related differences between normal values. In each parameter, increasing deviation from the normal is given a greater score. The scores for all of the different parameters are cumulated to produce a single numerical value (figs 1 and 2). The more abnormal the physiological parameters recorded, the higher the PAWS score obtained. The normal values used in the chart were taken from the Advanced Paediatric Life Support (APLS) guidelines.10

We completed a pilot study to validate the scoring system by performing a retrospective analysis of children attending the ED of James Cook University Hospital, Middlesbrough. Fifty consecutive patients who required admission directly from the ED to the paediatric intensive care unit (PICU) between 1 September 2003 and 1 September 2005 were identified. This list was obtained from a database of all admissions kept on the PICU. A control group of 50 consecutive children who were admitted from the ED to the general paediatric ward within the same time period was also identified from the ward admission book. The ED cards for both groups were obtained and the PAWS scores were calculated, based on data recorded at presentation to the ED. Children whose cards could not be located were excluded from the study. As some data were likely to be missing from the cards, a decision was made that missing values would be assumed to be normal. We then compared the PAWS scores between the two groups in order to see whether the PAWS chart would be able to identify those children in need of admission to a critical care area.
RESULTS
Of the 50 patients in each group, cards were missing for one of the ward patients and four of the PICU patients, leaving 49 and 46 in the two groups. The age range of the patients in both groups was 0–16 years. There was no significant difference between the two groups with regard to sex or mean age (table 1). The range of PAWS scores for patients admitted to the PICU was 0–16 compared with 0–6 in the patients admitted to the general paediatric ward. The mean and median PAWS scores in the patients admitted to the PICU were higher than in the group admitted to the general paediatric ward (table 1).
The area under the receiver operating characteristic (ROC) curve was calculated (fig 3). The PAWS score was found to be able to discriminate between cases and controls, with an area under the ROC curve of 0.86 (p<0.0001). The curve suggests using 3 or 4 as the trigger score. At a trigger score of 3, the PAWS score was able to identify those children requiring admission to the PICU with a sensitivity of 70% and a specificity of 90% (table 2).

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Four paediatric early warning scores have been published,6–9 but none of them has yet been fully validated. None of the published tools has been specifically designed for use in the ED and, consequently, to complete the chart fully they require data that may not be immediately available in the ED setting. The PAWS chart can be fully completed by simply taking a thorough set of observations. Indeed, we feel that one of the benefits of using the chart is that it ensures that complete sets of observations are, in fact, being done, including those values that are often less well recorded such as respiratory rate.11
Assessment of paediatric patients is complicated by the range of normal parameters in different age groups. Inexperienced staff may find it difficult to interpret the significance of physiological readings over a wide range of ages. By drawing together clinical data as a single numerical score plotted on a colour coded chart, abnormal physiology is more readily identified. It serves to act as a “red flag” for those children who are in need of urgent assessment and intervention. The chart is visually striking and similar in design to those commonly used for adult patients. The reverse side of the chart also provides a useful “aide-memoire” for the normal physiological values in different age groups.
Having evaluated the ROC data, the curve suggests using 3 or 4 as the trigger score. Our chart is designed to be a “rule-in” tool, and we therefore feel that a PAWS score of 3 is the most suitable trigger value as it has the higher sensitivity. Using a trigger score of 3 or more, the PAWS chart is able to identify patients who require admission to an intensive care facility with a sensitivity of 70% and a specificity of 90%. We could raise the sensitivity of the chart further by lowering the trigger score, but this would be at the cost of having a much lower specificity. It is unlikely that any physiology-based scoring system will achieve 100% sensitivity in identifying children needing intensive care. Severely ill children with single organ pathology, or children early in the course of a rapidly progressive illness, may have relatively normal physiological values and may not be picked up by this type of system.
We used admission to the PICU as a surrogate marker for severe illness. Our unit does not have a paediatric high dependency unit (HDU). There may therefore have been some children admitted to the general paediatric ward who did in fact receive a level of care equivalent to high dependency and who were significantly unwell. This could have the effect of decreasing the specificity of the PAWS score in our study. In the future, it would be useful to validate the PAWS score further by using an illness severity scoring system to refine the description of the children’s clinical status.
We did not record exactly what data were missing from the ED cards. On reflection, we feel that this information should have been collected. However, we still feel that, for the purpose of this pilot study, it is reasonable to assume that if data were not documented on the card, they were within normal values. With all children having been assessed by at least one nurse and one doctor, it is highly likely that, if a physiological value was abnormal, it would have been identified and subsequently documented.
The PAWS chart provides a simple way of identifying children with significantly deranged physiology for their age. The data that we present here are limited to a pilot evaluation of PAWS and we plan subsequent refinement of the tool and prospective validation of its use. It is not intended to be used in isolation as the sole determinant of the need for admission to an intensive care facility. However, if used as an adjunct to standard clinical assessment, it could provide an additional tool with which to “red flag” children who need a high level of treatment or monitoring.
CONCLUSIONS
We have designed a physiology based-scoring system for use in children in the ED setting. This pilot evaluation demonstrates that the PAWS chart shows promise as a “rule-in” tool for PICU admission. Future prospective validation of PAWS is necessary to assess its ability to identify all children in need of urgent medical assessment and intervention in the ED.
Acknowledgments
The authors thank Caroline White, Sister in the Paediatric Intensive Care Unit, James Cook University Hospital, Middlesbrough, for her help in the preparation of this document and Mr A P Navarro for his help with statistical analysis of the data.
Footnotes
Funding: None.
Competing interests: None.
Linked Articles
- Primary survey