Article Text

Abstract
Eosinophils are important effector cells of the innate immune system. Eosinophilic infiltrative disorders of the gastrointestinal tract, though recognised for decades, have recently witnessed a resurgence of interest, particularly for oesophageal disease. A more comprehensive basis for eosinophilic infiltration and activation has identified interleukin 5 (IL5) as a key cytokine for the differentiation and proliferation of eosinophils, while eotaxins promote the recruitment of mature eosinophils to the gut. When activated, eosinophils release multiple cytotoxic agents and immunomodulatory cytokines, resulting in local inflammation and tissue damage. Although eosinophils normally convey a defence against unwanted interlopers such as parasites, in the absence of such inciting agents, their accumulation and activation can elicit the primary infiltrative disorders of the gut: eosinophilic oesophagitis, gastroenteritis and colitis. Diagnosis of these disorders is dependent on the clinical presentation, endoscopic findings (particularly for eosinophilic oesophagitis), and most importantly, histological confirmation. Dietary modifications and topical corticosteroids are first-line treatments for eosinophilic oesophagitis. Systemic corticosteroids are the mainstay of treatment for eosinophilic gastroenteritis; surgery may be required depending on the layer of mucosa involved. Eosinophilic colitis most often occurs in infants; removal of the causative allergen usually results in a complete response. Steroids may be required for older children/adolescents or adults. This review summarises current knowledge on the trafficking of eosinophils to the gastrointestinal tract and the clinical management of the primary disorders of eosinophilic oesophagitis, eosinophilic gastroenteritis and eosinophilic colitis.
Statistics from Altmetric.com
The gastrointestinal tract is a constant battlefield between challenges from the external environment and the internal milieu of the body which seeks to maintain homeostasis. With a vast epithelial surface exposed to foreign (potentially toxic) substances, the alimentary tract employs defences, particularly its immune system. This must be exquisitely balanced to exclude toxic agents and organisms while simultaneously allowing the efficient absorption of nutrients essential to life. Eosinophils are key effector cells of the innate immune system within the gastrointestinal tract. These cells are customary inhabitants of the gastrointestinal tract, except for the oesophagus. In an evolutionary sense, intestinal eosinophils protect vertebrates against parasitic infestations, particularly helminths. Although the rate of parasitic infections in humans has decreased markedly in the developed world, there has been a substantial rise in atopic/allergic disorders. As a result, hypersensitivity responses to allergens may be a driving factor towards recruitment and activation of gut eosinophils. There has been a resurgence of interest in eosinophilic gastrointestinal disorders over the last 20 years, particularly eosinophilic oesophagitis. Eosinophilic gastrointestinal disorders are a heterogeneous group of diseases, which are often grouped into primary (idiopathic) disorders and secondary eosinophilic disorders (inflammatory, infectious or hypersensitivity illnesses resulting in gut eosinophilia). This article reviews the physiology of gut eosinophils and the primary eosinophilic disorders: eosinophilic oesophagitis, eosinophilic gastroenteritis and eosinophilic colitis.
PHYSIOLOGY AND PATHOPHYSIOLOGY OF EOSINOPHILS
Origin of the eosinophil
Eosinophils were first described over century ago as granular white blood cells that stained readily with eosin. These “acid-loving” granulocytes (“acidophils”) are the predominant inflammatory cell involved in allergic and parasitic disorders in vertebrates.
Eosinophils begin life and reside in the bone marrow for 8 days while undergoing maturation. Eosinophils subsequently relocate into the peripheral circulation for 8–12 h and finally traffic to specific tissues, predominantly the gastrointestinal tract, where they reside for at least 1 week.
Several inflammatory mediators and chemoattractants enhance eosinophil development, migration and effector function. Differentiation of haematopoietic stem cells to eosinophils in the bone marrow is dependent on a number of cytokines and growth factors. In the presence of interleukin 1 (IL1), IL3 and granulocyte macrophage colony stimulating factor (GM-CSF), primitive stem cells become eosinophilic precursor myeloblasts.1 The terminal differentiation into eosinophils and any proliferation thereafter is critically dependent on the presence of IL5.2 3 Transgenic (Tg) mice that over-express IL5 under control of the T cell promoter CD2 (CD2 IL5 Tg mice) exhibit a 20-fold increase in eosinophils in haematopoietic organs.4 In contrast, mice that are deficient in IL5 (IL5−/− BALB/c Tg mice) have decreased circulating eosinophils (by 80%) and decreased gastrointestinal eosinophils (50%) compared with control (wild-type) mice. Similarly, mice deficient in the functional receptor of IL5 (βc-deficient mice, C57BL/6) have decreased peripheral circulating and gastrointestinal eosinophils. Interestingly, as bone marrow eosinophils are only slightly reduced in either IL5 deficient or IL5 receptor deficient mice, other factors must be responsible for maintaining basal levels of eosinophils.5
Only a small number of mature eosinophils normally circulate in the peripheral blood. Rather, eosinophils are predominantly tissue-dwelling cells with greatest affinity for epithelial surfaces that interact with the external environment (eg, skin, lung and gastrointestinal tract). Eosinophils customarily reside in haematopoietic tissue and in the lamina propria of the gastrointestinal tract, the exception being the oesophagus.6 7 Within the lamina propria, eosinophils are ideally situated to protect against parasitic infestation. Resident eosinophils in the gastrointestinal tract do not evoke either an inflammatory reaction or cause tissue damage under normal circumstances.4 5 When provoked, eosinophils become activated to degranulate, releasing multiple cytotoxic agents to rid the body of the noxious agent or organism, but they also can result in local tissue damage and dysfunction. Eosinophils are mediators of allergic responses such as atopic dermatitis, allergic rhinitis, asthma and eosinophilic disorders of the gastrointestinal tract.
Trafficking of eosinophils to the gastrointestinal tract
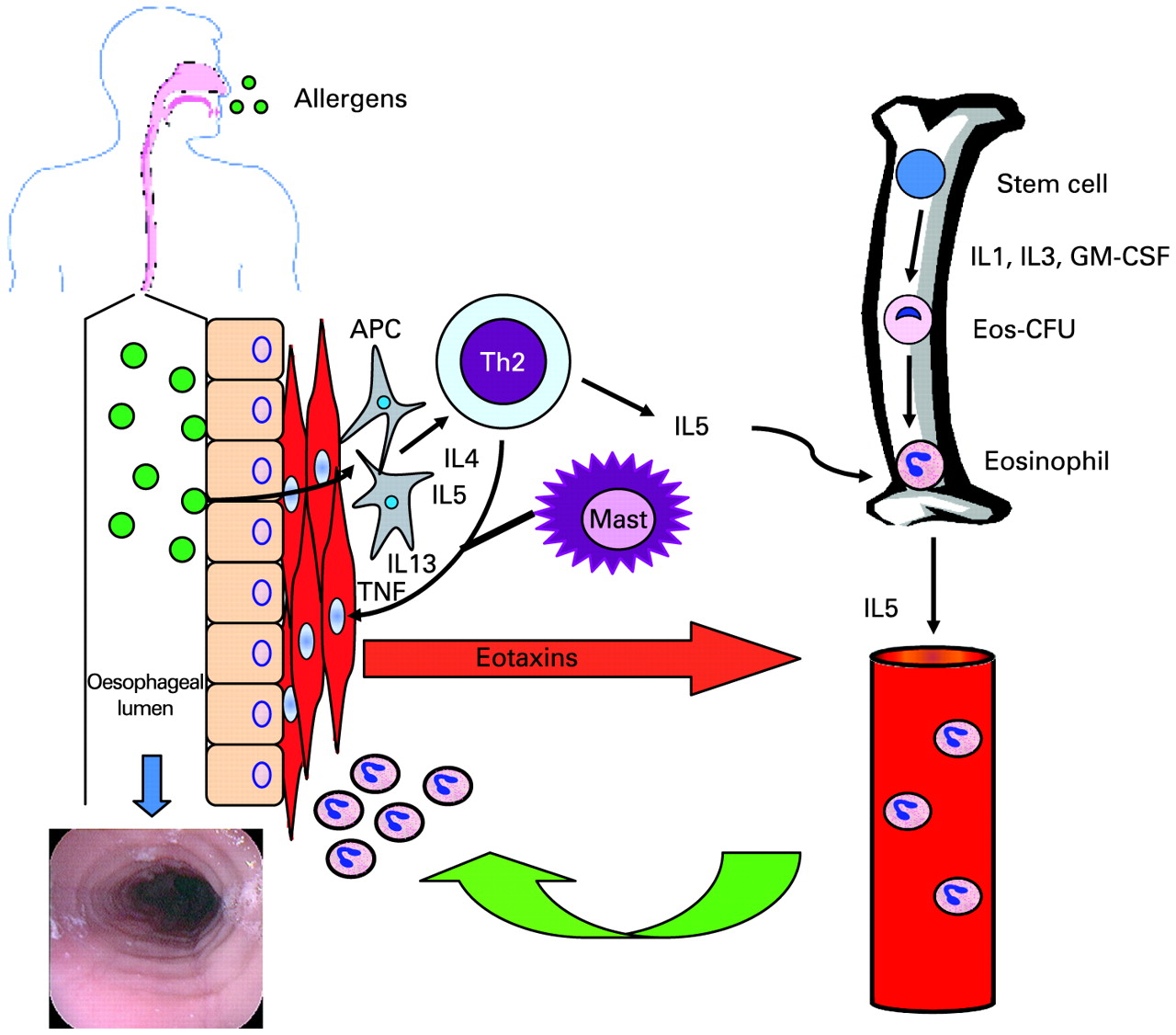
Homing of eosinophils to the oesophagus is shown in fig 1. Eosinophils initially home to the gut in the prenatal period, independent of bacterial flora.5 Although IL5 is important in regulating circulating levels of eosinophils, their accumulation in the gastrointestinal tract depends on a synergistic effect with eotaxin. Over-expression of IL5 in CD2 IL5 Tg mice results in a 4-fold increase in eosinophils in jejunal lamina propria and an almost 50-fold increase in oesophageal eosinophils, compared to wild-type mice.5 Conversely, mice deficient in eotaxin (CD2 IL5 Tg eotaxin −/−) have a significantly reduced number of jejunal eosinophils (by ∼90%), whereas peripheral eosinophils increase 2-fold.5 Therefore, the absence of eotaxin dramatically reduces eosinophils accumulating in the gut despite an elevated IL5 and the presence of increased circulating eosinophils. Thus, IL5 is important for upregulating eosinophilic differentiation by haematopoietic organs and controlling peripheral circulating eosinophil levels, whereas eotaxin is required for trafficking and accumulation in the gastrointestinal tract.

Homing of eosinophils to the oesophagus. Eosinophilic precursors (colony forming units) (Eos-CFU) are generated in the bone marrow under the influence of interleukin 1 (IL1), IL3, and granulocyte macrophage colony stimulating factor (GM-CSF). Patients are exposed to allergens (food or air). Antigen presenting cells (APCs) process these antigens and present them to helper T lymphocytes (Th2). Activated Th2 cells produce IL5, which is critical for the terminal differentiation and proliferation of eosinophils. IL4 is also produced by Th2 cells, which promotes eosinophilic accumulation and immunoglobulin E (IgE) production from B cells. In addition, Th2 cells and (activated) mast cells release IL13 and tumour necrosis factor (TNF) which promote local inflammation. Gastrointestinal epithelial cells produce eotaxins, which has essential chemokine activity for the recruitment of circulating eosinophils to the site of inflammation. As a result, mature eosinophils accumulate in the oesophagus, are activated, and degranulate releasing multiple cytotoxic agents. Chronic inflammation leads to architectural changes to the oesophagus as manifested in this diagram by mucosal rings, linear furrows, and adherent white exudates.
Eotaxin is a member of the chemokines (termed CC) family and was initially discovered in a rodent model for asthma and allergen-induced lung eosinophilia.8 9 Subsequently, human eotaxin was cloned and shown to be a specific chemoattractant for eosinophils.10 11 Human genomic analyses have led to two further eosinophilic specific chemokines, named eotaxin 2 and 3.12 13 Eotaxin 2 and 3, however, are located on a different chromosome and only share 30% sequence homology to eotaxin 1.9 The receptor for all eotaxins is CCR3 which is highly expressed on eosinophils. Eotaxins play a major role in regulating eosinophil levels in the gut, as demonstrated by a constitutive high expression of eotaxin mRNA by intestinal cells.10 14 Eotaxin-1 deficient mice (eotaxin−/− 129/SvEv mice) exhibit markedly reduced intestinal eosinophils in the absence of change in peripheral, splenic or marrow eosinophils.5 15 Similarly, CCR3 deficient mice have decreased baseline eosinophils (but increased splenic eosinophils) and do not recruit eosinophils when infected with Trichinella spiralis.16 Eotaxins therefore have a critical role for recruiting eosinophilic to the gastrointestinal tract.
Activation of eosinophils
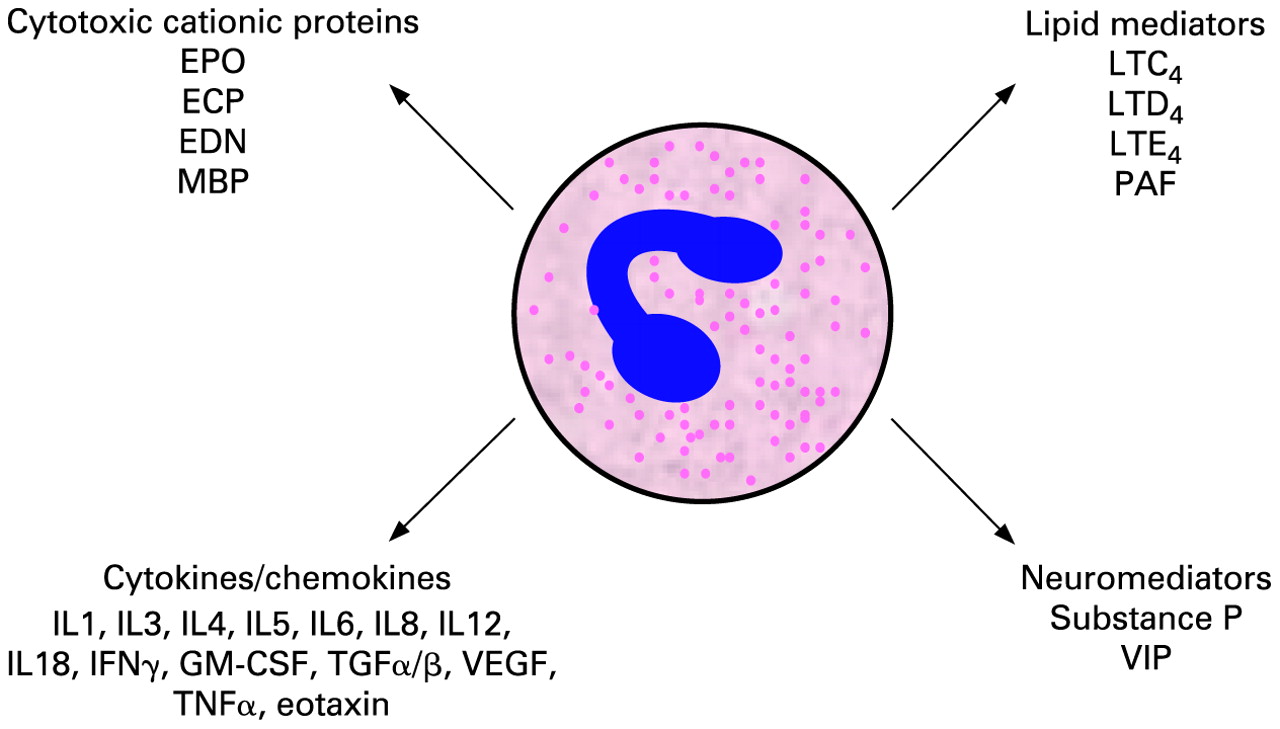
Eosinophils respond to a number of stimuli including non-specific tissue injury, allergens and infections (fig 2). Recruitment and activation of eosinophils to sites of inflammation is regulated by cytokines, including IL5, IL13, IL4 and tumour necrosis factor (TNF) produced by activated Th2 and mast cells.17 18 Activation results in degranulation, upregulated cytokine production, and IgE production. Pre-formed granules contain four major cationic proteins, all of which are cytotoxic: eosinophil peroxidase (EPO), eosinophilic cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and major basic protein (MBP). In addition, ECP and EDN have ribonuclease activity. MBP increases smooth muscle reactivity and can directly induce degranulation of mast cells and basophils. Eosinophils also generate large quantities of leukotriene (LT) C4, which is then metabolised to LTD4 and LTE4. All three are potent smooth muscle constrictors. Eosinophils produce a wide range of cytokines that potentiate the inflammatory response including IL1, IL3, IL4, IL5, IL6, IL8, GM-CSF, transforming growth factor (TGF)α/β, TNF, and eotaxin. Eosinophils therefore act not only as effector cells, but also as immunoregulatory cells.

Mediators released by activated eosinophils. This figure is modified from Rothenberg.9 ECP, eosinophilic cationic protein; EDN, eosinophil-derived neurotoxin; EPO, eosinophil peroxidase; GM-CSF, granulocyte macrophage colony stimulating factor; IFN, interferon; IL, interleukin; LT, leukotriene; MBP, major basic protein; TGF, transforming growth factor; TNF, tumour necrosis factor; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide.
EOSINOPHILS IN GASTROINTESTINAL DISEASE
Although first described in 1930s, eosinophilic gastrointestinal disorders did not receive great attention until the last decade. Publications have exponentially risen in the last decade, in particular for eosinophilic oesophagitis (fig 3). Eosinophilic disorders of the gastrointestinal tract can be separated into primary or secondary eosinophilic diseases: primary having no inciting cause, and secondary due to other illnesses resulting in eosinophilia.9 These gastrointestinal inflammatory disorders involve eosinophils but most patients also have a common feature of food-specific IgE and atopy, without food-induced anaphylaxis. Their features seem more related to cellular-mediated hypersensitivity from eosinophils rather than humoral (IgE) hypersensitivity.

PubMed search for “eosinophilic oesophagitis” (EO), “eosinophilic gastroenteritis” (EGE) and “eosinophilic colitis” (EC). Relatively few publications were available prior to 1995. From 2000 to 2008 there has been a surge of publications related to eosinophilic disorders of the gastrointestinal tract. In particular for eosinophilic oesophagitis, publications have risen exponentially since 1991.
Eosinophilic oesophagitis
Eosinophilic oesophagitis (EO), first reported in 1977, has gained widespread recognition over the past decade.19–21 Eosinophilic infiltration of the oesophagus can arise from acid-pepsin reflux into the reflux oesophagitis (GORD)22 but EO is a distinct entity, likely the product of a genetic basis, requiring allergens for expression.23 24 The differential diagnosis for eosinophilic oesophagitis and eosinophilic gastrointestinal disorders is shown in table 1.
Epidemiology and natural history
EO affects all ages and all ethnic groups, although reports have been selective, emanating predominantly from developed, industrialised countries. Population-based findings in children suggest an incidence of 1 in 10 000 and a prevalence of 4 in 10 000.25 An Italian study estimated a rather high prevalence of 3.5% in children.26 There appears to be a familial aspect to EO, implicating genetic factors.27 In adults, large studies are lacking, but estimates suggest an incidence of 2–6 per 105/year and a rising prevalence over a 16 year period from 2 per 105 to 27 per 105.28 Population-based data from an urban Canadian centre yield a combined children and adult incidence of 7.2 per 105/year.29 Prevalence from a large database in the United States indicates that EO occurs at any age (not just children); in adults it occurs most commonly in the 30s and 40s.30 There is a male predominance at 3:1 male to female ratio. Food impaction has a high pre-test probability for the disease; some 50% of cases with food bolus impaction are related to it.31 32 In a population study of upper endoscopies performed in 1000 (randomly selected) Swedish adults, 5% had increased eosinophils (many also had GORD), while 0.4% had definite eosinophilic oesophagitis.33 Thus EO is more frequent in children and young male adults; its primary associations are with a personal and family history of other allergic conditions. Indeed, the incidence of the disease appears to be rising, in part due to increased recognition.28 34
Clinical practice points for eosinophilic oesophagitis
Eosinophilic oesophagitis is an important and established cause of dysphagia
Adult patients often present with dysphagia, food impaction, or reflux symptoms non-responsive to proton pump inhibitor therapy
Endoscopic features are typical and need to be recognised; normal endoscopy does not exclude eosinophilic oesophagitis
Biopsy for histology is critical for the diagnosis of eosinophilic oesophagitis: four to five biopsies in the mid- to upper oesophagus maximises sensitivity
Topical corticosteroid is first-line treatment in adults; relapse is common
Dilatation may be useful to treat fixed strictures after medical therapy, but is associated with an increased risk of mucosal lacerations and perforation
Endoscopic complications may be as high as 31%
Its natural history reveals fluctuating symptoms that appear to correlate with seasonal variability and exposure to exogenous allergens. A disproportionally increased frequency of EO is diagnosed in late summer/fall, supporting the putative role of inhaled allergens.35 In long-term follow-up of adults36–38 and children,39 EO does not appear to limit life expectancy nor is it associated with any increased risk of premalignant/malignant conditions. Nevertheless, the disease has a significant impact on quality of life.40 In children, most will have recurring symptoms after withdrawal of medical treatment; however, dietary treatment can be highly successful in inducing and maintaining remission.39 In adults, one-third of patients experience stable symptoms whereas one-quarter have increasing dysphagia, when followed for some 7 years (range 1.4–11.5 years).36 Any natural progression of disease from childhood to adult life has not been studied. Given the chronic nature of EO, affected children likely will continue to experience it into adulthood. This would support the epidemiological evidence showing a rise in prevalence over time.28
Clinical characteristics and diagnostic criteria
The diagnosis depends on the clinical presentation, endoscopic features and histological criteria.41 The most common clinical presentation in adults is chronic, non-progressive dysphagia for solids (approximately 70%) and/or food impaction, followed by gastro-oesophageal reflux disease/heartburn (GORD, 38%) (table 2).30 Vomiting and regurgitation may also be present. Uncommon are haematemesis, weight loss and failure to thrive. Children more often present with heartburn (38%), abdominal pain (31%), and failure to thrive compared to adults. Atopy (asthma, atopic dermatitis, eczema and food and seasonal allergies) is common in both children and adults.
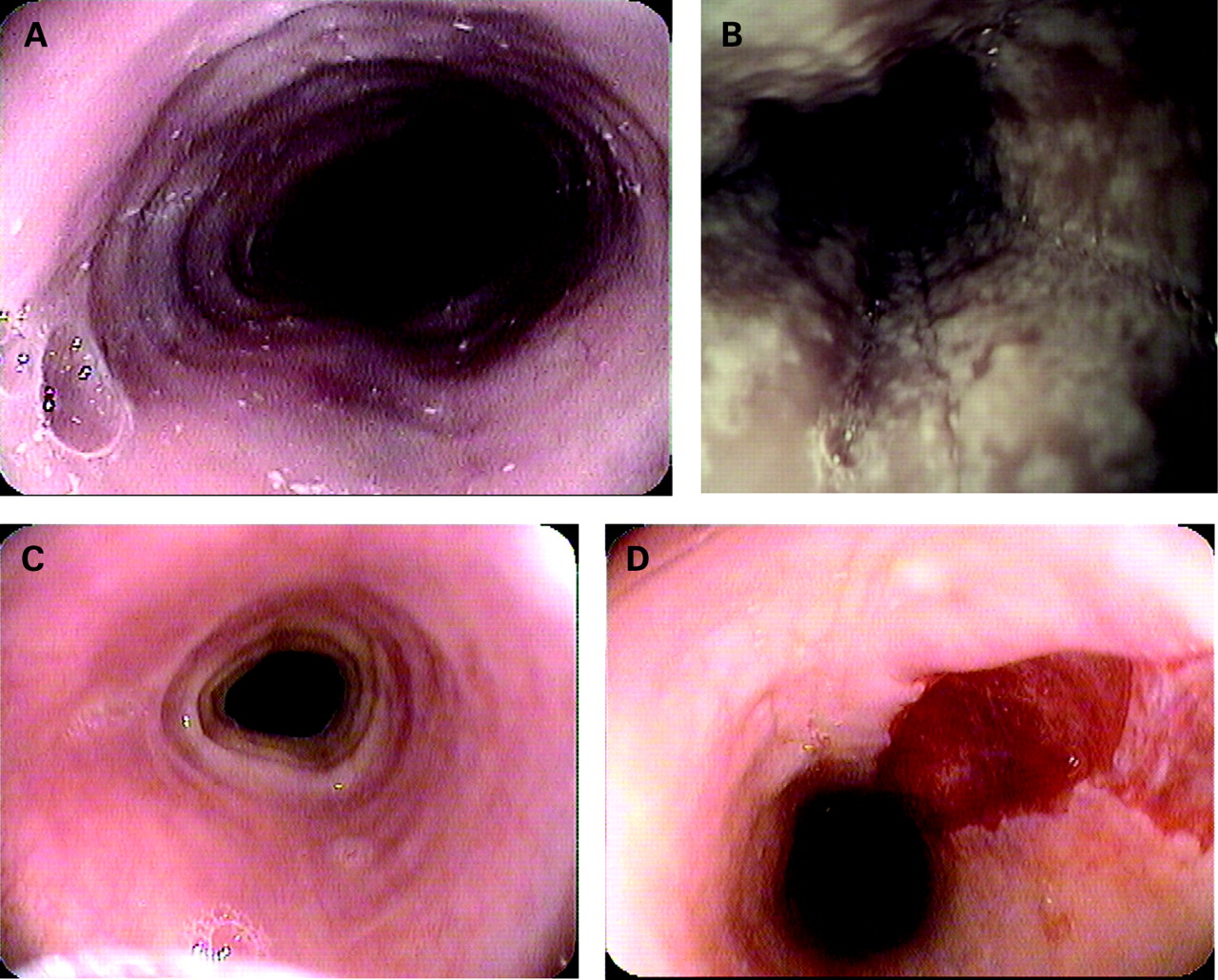
Endoscopic features can be characteristic (table 3, fig 4A–D). Oesophageal furrows may indicate active disease; adherent white papules represent eosinophilic aggregates.42 Yet, no single endoscopic feature is pathognomonic for EO. In patients with endoscopic features of the disease, about one-third (8/21 in a recent report) will fulfil the diagnostic histological criteria.43 Conversely, a normal endoscopy does not necessarily exclude it. Approximately 10% of adult patients with dysphagia and a normal endoscopic appearance will have it histologically.43 One-third of children with severe histological eosinophilia have a normal oesophagus on endoscopy.39
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Endoscopic images of eosinophilic oesophagitis. (A) Concentric rings, (B) linear furrows and adherent white exudates, (C) small calibre oesophagus with stricture, (D) mucosal laceration from diagnostic oesophagogastroduodenoscopy.
As histology is critical for the diagnosis of EO, biopsies should be attained regardless of the endoscopic appearance of the oesophagus.41 Biopsies might also be attained from the stomach and duodenum to rule out eosinophilic gastroenteritis and Crohn’s disease.41 Although the literature varies widely on the threshold number of eosinophils per high-power field (ranging from 15 to 30 per high-power field (hpf)), consensus opinion suggests a diagnostic threshold number of ⩾15 eosinophils/hpf in the mid oesophagus (table 4).41 On average, most patients will have >40 eosinophils/hpf.24 There is no definite cut-off criterion to distinguish EO from acid-peptic gastro-oesophageal reflux solely based on number of eosinophils, although reflux typically induces infiltrates with counts less than 10 per hpf.24 Other supporting features of the disease include basal zone hyperplasia, increased papillary size, superficial eosinophilic layering/aggregates, and microabscesses. The sensitivity of biopsies for the diagnosis of EO depends on the number of biopsies taken, increasing from 55% for one biopsy specimen to 100% for five specimens.44 Because acid-pepsin injury to the oesophagus causes a modest infiltration of eosinophils, some overlap can exist between EO and GORD, supporting the notion of doing proximal oesophageal biopsies to better distinguish EO. Thus all diagnostic features should be correlated with the clinical context.
Pathophysiology
The basis for developing EO is only partially understood.20 Compared to other regions of the gastrointestinal tract, the oesophagus normally lacks eosinophils. Allergic responses, tissue injury or infection cause the trafficking of eosinophils to the oesophagus where they become activated to secrete chemokines, cytokines, lipid mediators and cytotoxic secretory products (see preceding sections). How this results in dysphagia and food impaction is unknown. The chronic inflammation likely causes thickening of the mucosa/submucosa and muscularis propria layers, leading to fibrosis and remodelling, according to endoscopic ultrasound case reports in children and adults.45–47 Collagen accumulates in the mucosa and lamina propria of the oesophagus while the basal layer thickens.48 Oesophageal manometry varies in adults and children, but may be abnormal in one-half41 49 50 Most of the positive findings are non-specific peristaltic abnormalities; however, high-amplitude contractions, spasms, tertiary contractions and aperistalsis have been reported.49 Primary motility disorders are rare, having been identified in only 12 patients: two with achalasia, seven with diffuse oesophageal spasm, and three with the nutcracker oesophagus.49 The authors also have another with scleroderma (personal communications). The mechanisms by which dysmotility arises is not completely understood. Theories abound: increased contraction of fibroblasts in the presence of eosinophils, axonal necrosis from eosinophil degranulation, major basic protein effects on smooth muscle contraction, and inflammatory cytokine inhibition of acetylcholine release leading to dysmotility. The lower oesophageal sphincter pressure is normal in most patients; hypotensive and hypertensive lower oesophageal sphincter pressures are rarely seen. Some confusion arises because patients with EO may have concomitant GORD, based on pH testing.50
Treatment
Multiple therapeutic regimens have been used with varying success in both the paediatric and adult populations (table 5).41 Dietary restriction with either an elemental or elimination diet has been very successful in children with reported response rates up to 98%.39 51 52 Dietary studies in adults are limited, appearing only as abstracts.53 54 Corticosteroids have been used successfully to treat EO in both children and adults. Swallowed fluticasone is effective for clinical, endoscopic, histological and immunological improvement,50 55–59 although only one randomised, double-blind, placebo-controlled trial has been published. In this study, 50% of children achieved histologial remission, compared to 9% for placebo.57 Approximately 75% of adults attained complete remission in non-randomised clinical studies.41 Recommended dosage is fluticasone 880–1760 μg per day split into twice or four times daily dosing for 6–8 weeks. Recurrence of symptoms is common and can occur in 50–60% at 1 year.41 55 Furthermore, up to 20% may develop oral and/or oesophageal candidiasis. Use of systemic steroids has only been published in the paediatric population; a 4 week regimen of 1.5 mg/kg methylprednisolone may be effective.60 In a trial comparing topical fluticasone to oral prednisone, no significant difference was found in efficacy or relapse, although fewer adverse events were noted for fluticasone.61 Oral budesonide theoretically is a less cumbersome method of topical therapy than swallowing aerosolised particles. In a retrospective review of 20 children with EO, oral viscous budesonide 1–2 mg daily for 3–4 months resulted in an 80% response rate (defined as eosinophils <7/hpf) with a significant correlation between symptomatic, histological and endoscopic scores.49 In a preliminary report in adults with the disease, 2 mg/day budesonide for 15 days produced remission (defined as <5 eosinophils/hpf) in 11/18 (61%), compared to 1/18 (5.7%) receiving placebo.62
Other therapies for EO have employed small trials. Montelukast, a selective inhibitor of the LTD4 receptor, provided symptomatic improvement in eight adult patients with dysphagia secondary to EO.63 Six patients, however, experienced recurrence of symptoms within 3 weeks of dose reduction or cessation. Further, treatment did not change the density of eosinophils on repeat biopsy. Mepolizumab, a humanised anti-IL5 monoclonal antibody, shown benefit in five patients without serious side effects.64 65 Specific eotaxin inhibitors are also under development.66 Medications successfully used in eosinophilic gastroenteritis such as cromolyn and ketotifen (mast cell stabilising medications), and suplatast tosilate (a selective Th2 IL4 and IL5 inhibitor) have not been studied in adults with eosinophilic oesophagitis. Cromolyn was not efficacious in children with EO.39 Dilatation is useful in symptomatic patients with fixed strictures, but because of the increased risk of causing a mucosal laceration or perforation, such manipulation should only be undertaken after a trial of medical treatment.
Complications
EO carries a relatively high endoscopic risk as either perforations or mucosal lacerations (fig 4D) from oesophageal dilatation, biopsy or even from simply passing an endoscope.36 38 68–70 Eight perforations have been reported in the literature – five were procedure-related,69 71 72 and three were spontaneous oesophageal ruptures (Boerhaave’s syndrome).71–73 In a single-centre audit over a 5 year period, 11 of 36 patients (31%) with EO experienced complications: seven mucosal lacerations, three perforations, and one spontaneous emesis-induced rupture.71 The presence of strictures, a longer duration of symptoms, and higher density of eosinophilic infiltration were associated with an increased risk for complications. Dilation was involved in six of the complications, occurring with through-the-scope balloons in four, a bougie in one, and an endoscope as dilator in another. The perforation rate for food bolus removal requiring rigid endoscopy has been reported at 2/134.72 At our centre, we have not observed such a high complication rate, with only 5.5% rate of minor complications over a 4 year period (personal communication).
EOSINOPHILIC GASTROENTERITIS
Eosinophilic gastritis and eosinophilic enteritis appear to be disorders separate from eosinophilic oesophagitis. Eosinophils are constitutive inhabitants of the gastrointestinal outside of the oesophagus in the normal, healthy state. Therefore, diagnosis of idiopathic eosinophilic gastroenteritis is more difficult than when the oesophagus is involved. Disorders are best categorised into primary (idiopathic) or secondary eosinophilic gastroenteritis (table 6). Primary eosinophilic gastroenteritis (EGE) has also been termed allergic gastroenteropathy, as a subset of patients have an associated allergic component.74–76 Although considered idiopathic, an allergic mechanism may be involved as most patients exhibit increased total IgE and food-specific IgE levels. Secondary disorders linked to EGE include the hypereosinophilic syndrome (HES), coeliac disease, Crohn’s disease, vasculitis (Churg–Strauss syndrome, polyarteritis nodosa), connective tissue disease (scleroderma), infection (Helicobacter pylori, parasites) and drug injury/hypersensitivity.
Epidemiology
EGE is exceedingly rare, lacking epidemiological data to estimate its true frequency. Since its original description in 1937,77 fewer than 300 cases have been reported in the literature.42 75 78 Major referral centres may identify 1 case per 100 000 patients. Even the Mayo Clinic (from medical records documenting more than 4 million individuals) was only able to identify 40 patients with EGE from 1950 to 1987.79 It can affect any age group, but the peak incidence is in third to fifth decade of life. There is a slight male predominance of about 1.4:1. EGE is a benign disorder, albeit the natural course of the disease is unknown.
Clinical presentation
Clinical feature of EGE are listed in table 7. The Klein classification80 separates EGE into mucosal, muscular or (sub)serosal disease as the clinical presentation is dependent on the involved layer of the gastrointestinal tract.9 42 75 79 81 Approximately 57.5% have mucosal, 30% muscular and 12.5% (sub)serosal disease, respectively.79 Patients with predominant mucosal disease present with symptoms similar to inflammatory bowel disease. This may include vomiting, abdominal pain, diarrhoea, gastrointestinal bleeding, iron deficiency anaemia, malabsorption, protein-losing enteropathy, or failure to thrive. Disease involving the muscularis propria typically presents with obstructive symptoms.82 Distinguishing features of serosal involvement are the presence of ascites (with a low serum:ascites albumin gradient), bloating, a high peripheral eosinophil count, and possibly features of peritonitis.79 83 84
Diagnosis
The diagnosis of EGE may be elusive. Symptoms are non-specific. Peripheral eosinophilia is variable; the eosinophil count is normal in 25% of patients.79 Atopy and allergies are associated in 25–75% of cases.75 Radiographic studies help detect the muscular disease by finding stenosis or thickening of the stomach and small bowel folds.85
Mucosal disease is the most readily diagnosed form of EGE, given that endoscopy can directly visualise any mucosal changes and acquire biopsies. Endoscopic features are nevertheless rather non-specific: thickened folds, erythema, friability, nodularity, and abnormal peristalsis.86 Biopsies show increased eosinophils; however, no standards of diagnosis have been established. Indeed, the “normal” number of eosinophils has not been defined and criteria may differ between pathology departments. For example, the “normal” ileum may show as many as 30 eosinophils per high-power field.87 Other suggestive histological features include eosinophilic infiltration of intestinal crypts and gastric glands. Other organs are not involved. Secondary causes of tissue eosinophilia, like helminthic infestations, should be excluded. In the muscular form, endoscopy may appear normal, although a case report has been published on a non-healing gastric ulcer ultimately being diagnosed as the mural form of eosinophilic gastritis on surgical pathology.88
Most EGE cases have been diagnosed on surgical, full-thickness biopsy or resection performed for obstruction or suspicion of malignancy. Serosal disease may be identified as part of an evaluation for ascites. Laparoscopy may reveal thickening of the peritoneum (both parietal and visceral) and white nodules; serosal biopsies are essential for the diagnosis.83 Other causes, such as malignancy or tuberculosis, must be excluded.
Treatment
The rarity of EGE has limited any large prospective randomised therapeutic trials. The mainstay of treatment in non-obstructive disease is corticosteroid therapy.78 79 89 Prednisone at a dose of 20–40 mg daily for 8 weeks can yield a good response. Budesonide is an alternative steroid with fewer systemic side effects.90 Those with serosal disease appear to experience the greatest response to corticosteroids.79 Elimination or elemental diets may be helpful in patients with mucosal disease or identified allergic response to foods.91 92 Other therapies used with some success include cromolyn,93 94 montelukast,95 96 ketotifen,97 98 suplatast tosilate,99 and octreotide.100 When therapy ends, the disease tends to relapse. Therefore, steroid-sparing treatments, such as dietary modification or montelukast, are preferred maintenance strategies. Immunosuppressive agents, like azathioprine or mycophenalate mofitil, might prove to be alternatives to corticosteroids though clinical trials are lacking.
EOSINOPHILIC COLITIS
Eosinophilic colitis (EC) can also be categorised as either being primary (idiopathic) or secondary to other disorders (with a similar differential diagnosis as EGE, table 6). Primary EC (also known as allergic colitis of infancy or dietary protein-induced proctocolitis of infancy syndrome) is sub-classified into atopic and non-atopic variants. EC has a bimodal age distribution, usually affecting infants (mean age of 60 days) and adolescents.101 102 In contrast to EGE, most EC is thought to be non-IgE based, although the exact immunological mechanism is not fully understood. It may be an early expression of protein-induced enterocolitis of which cow’s milk and soy proteins are considered the main culprits.103 104 EC may occur more often in infants who are exclusively breast-fed.101 103 It also may develop in children following solid organ transplantation. In one report, 37% of children with liver transplants on immunosuppression with tacrolimus had EC on rectal biopsy, performed to detect if lymphoproliferative disease had developed. Half of those with EC also had an atopic variant with elevated food specific IgE levels.105 A single case report has been published of an adult patient developing EC following bone marrow transplantation for acute myeloid leukaemia.106
The clinical features of EC are similar to EGE depending on degree and location of colon involvement.9 101 107 Diarrhoea, which can be bloody,108 is the classic presentation. Abdominal pain, anorexia and weight loss are other features, although the majority of infants are otherwise healthy with no constitutional features. Obstructive presentations (like caecal volvulus or intussusception) seem to be more common in adults compared to children.109 110 EC can even masquerade as a tumour.111–113 Laboratory features include increased peripheral blood eosinophilia or eosinophils on stool examination. Endoscopic findings are non-specific, being similar to EGE if the mucosa is involved: erythema, loss of vascularity, friability, nodularity and lymphonodular hyperplasia. Histology reveals increased eosinophils and aggregates of eosinophils in the lamina propria, muscularis propria, or subserosa. Other inflammatory cells are not present. The architecture of the mucosa is generally preserved, helping to distinguish EC from other colitides.
Clinical practice points for eosinophilic gastroenteritis
Eosinophilic gastroenteritis is a rare disease; secondary disorders must be excluded
Clinical presentation is influenced by the layer of gut involved:
mucosal: pain, diarrhea, malabsorption
muscularis: obstruction
serosal: ascites, bloating, tends to have higher peripheral eosinophilia
Endoscopic features (non-specific) accompany mucosal disease; muscularis and serosal disease are diagnosed on surgical full thickness biopsy or resection
The mainstay of therapy is corticosteroids
Relapse is common; steroid sparing alternatives should be considered in those with severe cases, which are steroid dependent or refractory
The natural history is unknown
In infants, the clinical course is usually benign. Withdrawal of the culprit protein trigger(s) usually resolves any symptoms. Bloody diarrhoea typically disappears within 72 h. Most infants will be able to tolerate a subsequent re-introduction of the culprit protein by age 1–3 years.101 103 Controversy exists as to whether or not infantile EC predisposes to the future development of inflammatory bowel disease.101
Older patients (adolescents and adults) may require medications because IgE-associated triggers are rarely identified even in the atopic variant.9 Although well-designed clinical trials are lacking, short courses of topical or systemic corticosteroids (prednisone 20–40 mg or budesonide 9 mg daily) for 1–2 weeks or a 5-aminosalicylic acid appear to be efficacious. The effectiveness of other agents used in EGE is unknown. In refractory cases, immunomodulator therapy with azathioprine may be required. The natural history of eosinophilic colitis in older patients is unknown; it tends to follow a waxing and waning course similar to eosinophilic oesophagitis and eosinophilic gastroenteritis.
Clinical practice points for eosinophilic colitis
Eosinophilic colitis is a rare disease; secondary disorders must be excluded
The disease is the most common cause of bloody stools in the first year of life:
withdrawal of the offending protein trigger usually results in clinical improvement
prognosis is very good; triggering foods can be re-introduced later by age 1–3 years
Older children and adults with eosinophilic colitis typically present with diarrhoea and abdominal pain
symptoms are dependent on location and degree of colon involved
treatment is withdrawal of offending food if atopic variant
a short course of corticosteroid (prednisone 20–40 mg daily for 1–2 weeks) or a 5-aminosalicylic acid is usually required
Endoscopy may be normal or have non-specific features of inflammation; histology shows an increased infiltration of eosinophils or focal aggregates
Older patients with the disease have a relapsing course; steroid-sparing alternatives should be considered in severe cases that are steroid-dependent or refractory
The natural history is unknown
CONCLUSION
Primary eosinophilic gastrointestinal disorders have undergone a renewed interest in the past decade. Eosinophilic oesophagitis has become a well-recognised cause of dysphagia and likely is the main cause of food bolus obstruction in young otherwise healthy adult men. This entity is separate from eosinophilic gastroentercolitis and is increasing in incidence. Recognition of its clinical presentation along with endoscopic and histological features provides the correct diagnosis and subsequent treatment. Eosinophilic gastroenteritis and colitis are quite rare but must be included in the differential diagnosis of non-specific gastrointestinal symptoms. Increased knowledge of the pathophysiology and underlying immune mechanisms should lead to more effective management of disorders of eosinophils. Under active investigation are agents to specifically block IL5, eotaxins or their receptors. Many questions remain unanswered: given the waxing and waning course of disease, what are the treatment goals and endpoints? Is there a role for maintenance therapy? What is the natural history of the disorders and does treatment alter the natural history? Vigorous randomised, controlled trials assessing current (and any novel) therapies are necessary to determine which agents are most effective. Eosinophils have always been a component of gastrointestinal tract physiology; our understanding of their role(s) has only just begun.
REFERENCES
Footnotes
Competing interests: None.