Article Text

Abstract
Currently, one of the most important unresolved questions concerning Helicobacter pylori is whether eradication of the organism leads to a sustained improvement in symptoms in patients diagnosed with functional (non-ulcer) dyspepsia. Recently, two very similar studies, the ORCHID and OCAY studies, have been completed and the combined results of these two multicentre, multinational, randomised, double blind, controlled clinical trials are reviewed.
- clinical trial
- dyspepsia
- Helicobacter pylori
- OCAY study
- ORCHID study
- quality of life
- symptom relief
- GDSS, Glasgow dyspepsia severity score
- GORD, gastro-oesophageal reflux disease
- GSRS, gastrointestinal symptom rating scale
- ITT, intention to treat
- MRC, Medical Research Council
- OAC, omeprazole 20 mg twice daily, amoxycillin 1000 mg twice daily, and clarithromycin 500 mg twice daily for seven days
- PGWB, psychological general well being
Statistics from Altmetric.com
- GDSS, Glasgow dyspepsia severity score
- GORD, gastro-oesophageal reflux disease
- GSRS, gastrointestinal symptom rating scale
- ITT, intention to treat
- MRC, Medical Research Council
- OAC, omeprazole 20 mg twice daily, amoxycillin 1000 mg twice daily, and clarithromycin 500 mg twice daily for seven days
- PGWB, psychological general well being
SUMMARY
One of the most important unresolved questions about Helicobacter pylori is whether eradication of the organism leads to a sustained improvement in the symptoms of functional dyspepsia. Recently, two multicentre, multinational, randomised, double blind, controlled clinical trials were completed which looked at the effect of eradication on functional dyspepsia symptoms over a 12 month follow up period. In the ORCHID study, 370 patients were randomised to seven days of treatment with omeprazole, amoxycillin, and clarithromycin (OAC) or placebo. In the OCAY study, 348 patients were randomised to seven days of treatment with OAC or omeprazole/placebo antibiotics. In both studies, patients were followed for 12 months and the main outcome measure was relief from dyspeptic symptoms, which was measured on a seven point Likert scale. “Responders” had no or minimal symptoms during the seven days preceding the final visit at 12 months. The proportion of responders in the combined intention to treat analysis was 26% (77 of 297) in the group of patients treated with OAC and 21% (65 of 306) in those treated with placebo/omeprazole only (NS). Quality of life scores were similar in both treatment groups over the 12 month period. In a secondary analysis, the rate of treatment success was significantly higher in patients in whom gastritis had healed compared with those in whom gastritis had not healed (31% v 21%, respectively; p=0.01, Fisher's exact test, two sided). In the dyspepsia subgroup analysis, patients with ulcer-like and reflux-like dyspepsia were more likely to be a responder if H pylori was eradicated; no difference was seen in the dysmotility-like dyspepsia group.
INTRODUCTION
Currently, one of the most important unresolved questions about H pylori is whether eradication of the organism leads to a sustained improvement in symptoms in patients diagnosed with functional (non-ulcer) dyspepsia.1 Recently, two very similar studies, the ORCHID and OCAY studies, have been completed.2,3 The combined results of these two multicentre, multinational, randomised, double blind, controlled clinical trials are reviewed here.
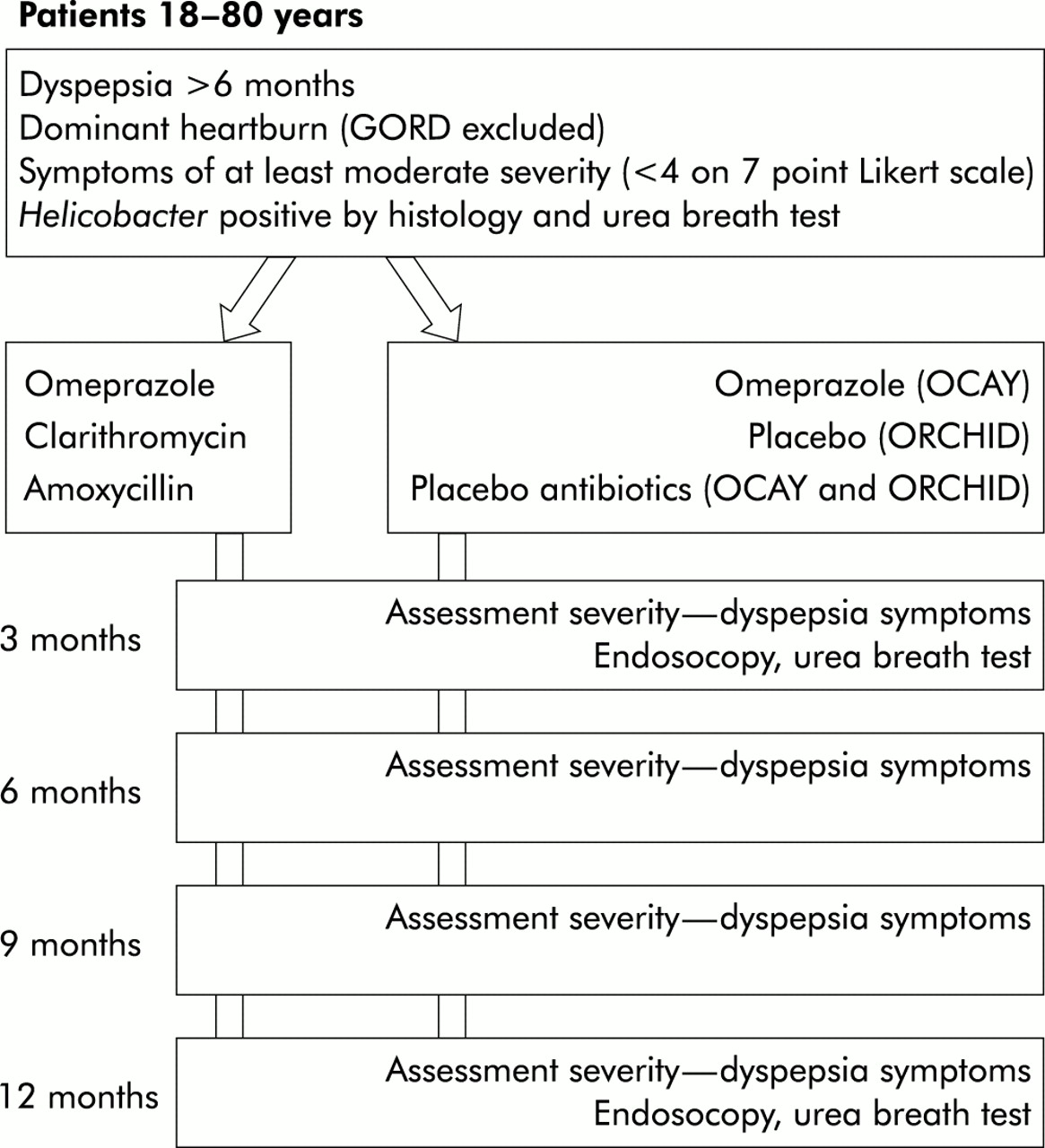
The primary objective in both studies was to compare the efficacy of H pylori eradication therapy using the combination of omeprazole, amoxycillin, and clarithromycin with that of either placebo (ORCHID study) or omeprazole (OCAY study) in relieving dyspeptic symptoms 12 months after the eradication therapy. The secondary objectives were: (a) to determine whether there is a relationship between healing of gastritis and symptom relief; (b) to determine whether dyspepsia subgroups help to predict treatment response; and (c) to examine the effect of treatment on gastrointestinal related quality of life. The basic study design is shown in fig 1.
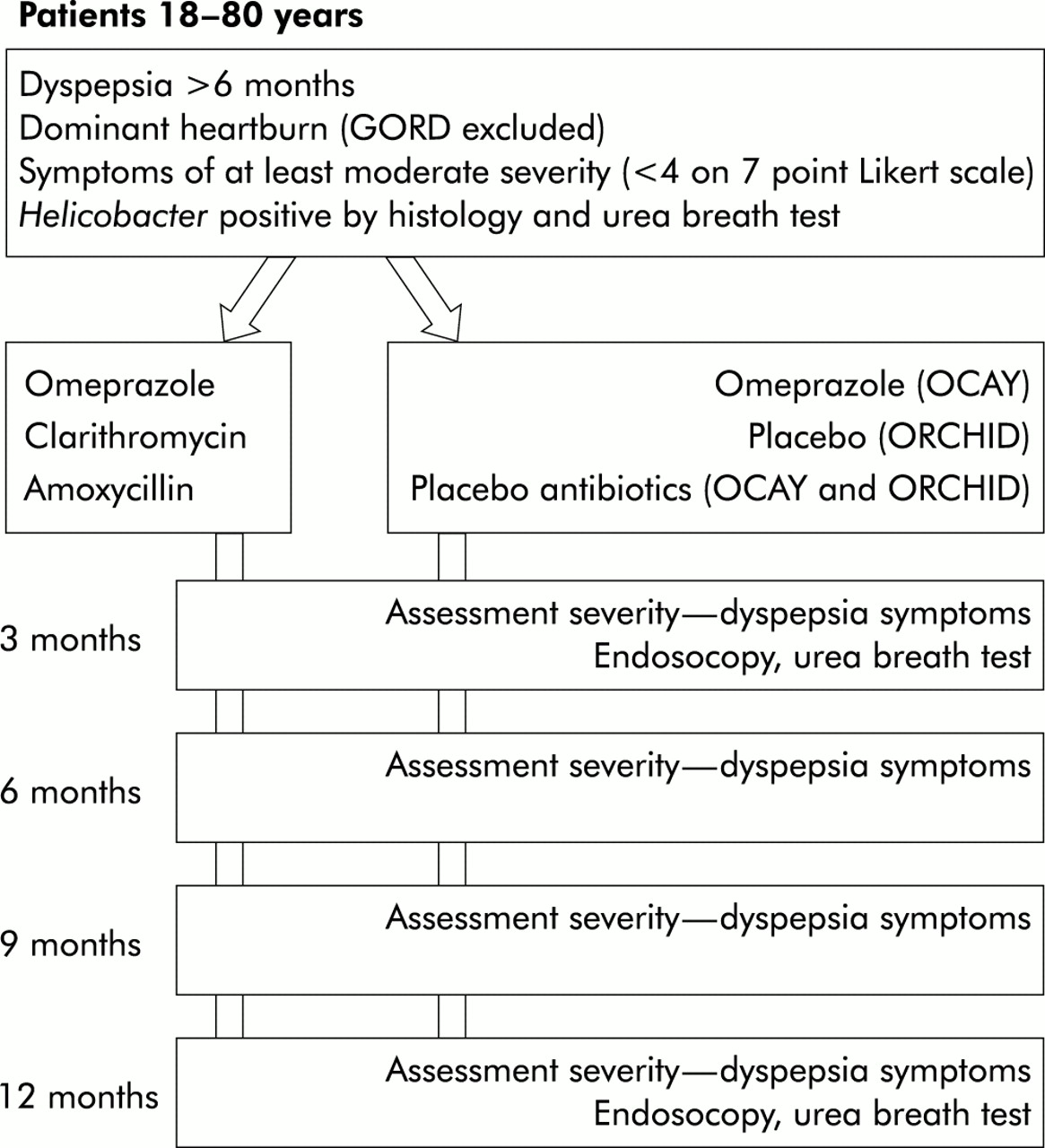
Design of the OCAY and ORCHID studies. GORD, gastro-oesophageal reflux disease.
STUDY PROTOCOL
In these multicentre, multinational, randomised, double blind, controlled clinical studies in investigated functional dyspepsia, a normal endoscopy was required for entry into the studies. Patients had to be between 18 and 80 years of age, and to be H pylori positive, which was assessed using a rapid urease test, histology, and a validated 13C urea breath test. Other inclusion criteria were as follows: patients needed to have pain or discomfort centred in the upper abdomen, which was of at least moderate severity, for a minimum of three days during the one week period of baseline observation. Severity was assessed on a seven point Likert scale, as shown in table 1; dyspeptic symptoms had to be present for at least six months and could be either continuous or frequently recurring.
Seven point Likert scale based on the response to the question: “overall, how would you rate the severity of your central upper abdominal pain/discomfort? ”
The main exclusion criteria were: (1) symptoms suggestive of gastro-oesophageal reflux disease (GORD) or irritable bowel syndrome; (2) a history of documented peptic ulcer disease or GORD; (3) a history of oesophageal or gastrointestinal surgery; and (4) the patient needed to have been off acid suppressive therapy with proton pump inhibitors and off antibiotics and bismuth for four weeks, and off H2 receptor antagonists for one week prior to inclusion.
The studies started with a one week run in period of baseline observations followed by a seven day treatment period. Patients were randomised to treatment with omeprazole 20 mg twice daily, amoxycillin 1000 mg twice daily, and clarithromycin 500 mg twice daily (OAC), or placebo (ORCHID), or omeprazole 20 mg once daily and placebo antibiotics (OCAY). Patients were followed up for a period of 12 months, and were seen at follow up on day 7 and at one, three, six, nine, and 12 months. To determine H pylori status, a 13C urea breath test was undertaken and endoscopy was performed, with biopsies taken from the antrum and body, at the start of the studies and at three and 12 months.
OUTCOME MEASURES
The primary objective in both studies was to compare the efficacy of H pylori eradication therapy with that of either placebo (ORCHID study) or omeprazole (OCAY study) in relieving dyspeptic symptoms 12 months after eradication therapy. Secondary objectives were to determine whether dyspepsia subgroups help to predict treatment response and whether there is a relationship between healing of gastritis and symptom relief. The studies also examined the effect of treatment on gastrointestinal related quality of life.
Several outcome measures were used. Patients were required to complete diary cards during the week preceding the follow up visits, documenting the severity of symptoms. The primary outcome measure was the seven point Likert scale for assessment of severity of epigastric pain or discomfort, as shown in table 1. A responder was defined as a patient who had either none or minimal symptoms (score 1 or 2) during the seven days preceding the final visit at 12 months. In addition, during the follow up visits two validated questionnaires were administered: the gastrointestinal symptom rating scale (GSRS) and the psychological general well being (PGWB) index. GSRS is a well validated gastrointestinal specific questionnaire that uses seven point ordinal (Likert) scales to measure five dimensions: abdominal pain, reflux, indigestion, diarrhoea, and constipation.4 The questionnaire has 15 questions, and GSRS is expressed as the mean item score. A total score can also be calculated—the lower the score, the better the patient feels. The PGWB index is an instrument that measures subjective well being and has been used in duodenal ulcer and GORD trials.5,6 The 22 questions of the scale are ranked on six point Likert scales. The instrument has six dimensions: general health, vitality, anxiety, depressed mood, self control, and positive well being. The score ranges from 22 to 132—the higher the score, the worse the quality of life. Both scales can detect a decrease in quality of health, and improvement following treatment, in patients suffering from duodenal ulcers and GORD when compared with healthy controls.6,7
Healing of chronic gastritis
Healing of gastritis was defined as a score of 0 or 1 for chronicity (mononuclear cells) on the four point scale of the Sydney system for classification of gastritis8 at 12 months. Furthermore, H pylori had to be absent and there had to be no activity (polymorphonuclear cells).
Dyspepsia subgroups
Patients were classified into three dyspepsia subgroups: ulcer-like, reflux-like, and dysmotility-like. This was done retrospectively and based on questions from the GSRS. For ulcer-like dyspepsia, patients needed to have a severity of at least 4 out of 7 for stomach ache and hunger pain; for reflux-like dyspepsia, a score of at least 4 for heartburn or reflux; for dysmotility-like dyspepsia, a score of at least 4 for two or more of the following symptoms: nausea, bloating, belching, and rumbling. Subgrouping was not mutually exclusive and patients could therefore end up in more than one subgroup.
RESULTS
Patients
A total of 603 H pylori positive patients (275 in the ORCHID study and 328 in the OCAY study) were included in the intention to treat (ITT) analysis, of whom 476 completed the 12 month follow up, 241 in the eradication therapy group and 235 in the placebo or omeprazole only groups. In total, 96 centres recruited patients for both studies. The following average numbers of patients were randomised per centre: less than three patients in 23 centres, three to five patients in 24 centres, and more than five patients in 49 centres. The groups were well balanced for sex (39% male), age (49 and 48 years), smoking (26% and 27%), and duration of disease.
Primary objective
In the ITT analysis, OAC treatment achieved cure of H pylori infection in 82% (244 of 297) of patients, as assessed at three months by histology and the urea breath test. In contrast, eradication was seen in only 3% (9 of 306) of patients randomised to either placebo or omeprazole only. Cure of infection at three months was associated with healing of gastritis. Using the predetermined definition of healing of gastritis, 231 (78%) of the 297 patients treated with OAC had complete healing of gastritis compared with 24 (8%) of the 306 patients on placebo/omeprazole only.
A patient was defined as a responder if he/she had no or minimal symptoms (score 0 or 1) on the seven point Likert scale during the seven days prior to the 12 month follow up visit. The proportion of responders in the ITT analysis was 26% (77 of 297) in the group of patients treated with OAC and 21% (65 of 306) in those treated with placebo/omeprazole only (NS). If the results were stratified according to whether H pylori was successfully cured, the results were also not statistically different among the treatment groups: 30% (76 of 253) in H pylori negative patients and 23% (68 of 297) in H pylori positive patients.
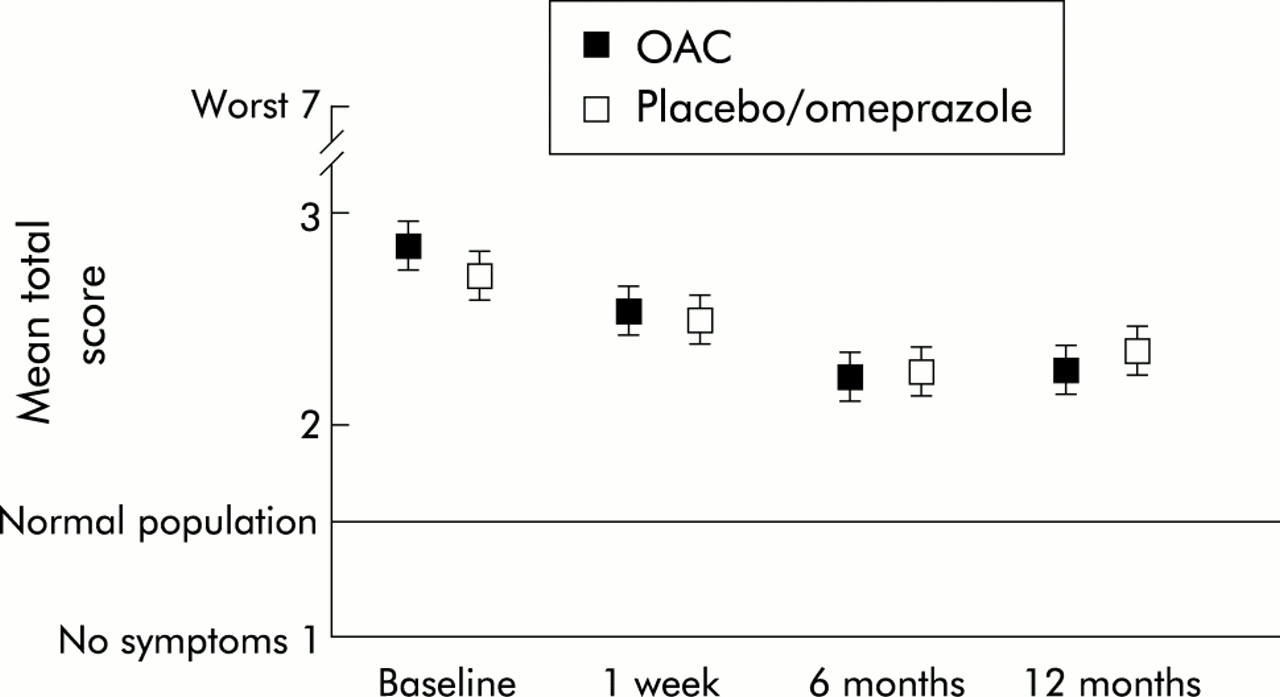
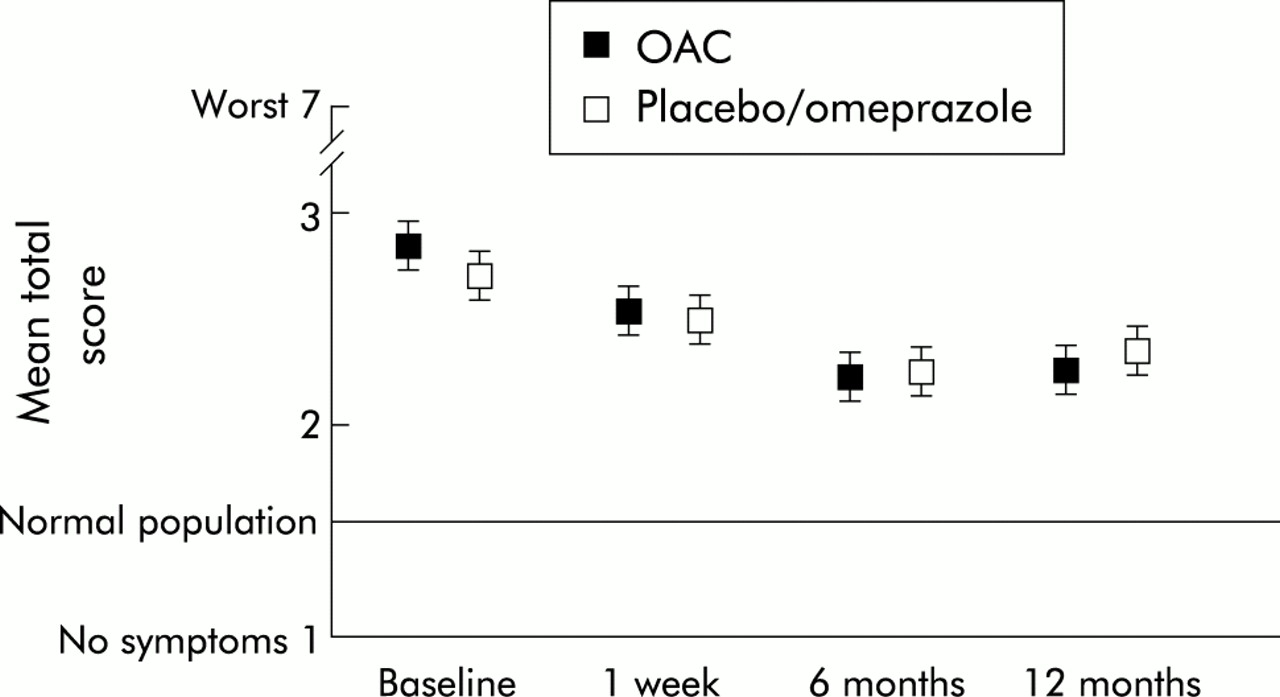
Similarly, the mean symptom scores over the 12 month period showed no differences between the two treatment groups (see fig 2). Interestingly, fig 2 shows that there was an overall improvement over the 12 month period in both treatment groups. Most of the improvement occurred early in the studies.

Improvement in mean symptom score using the seven point Likert scale and recorded on diary cards in the intention to treat population over 12 months. OAC, omeprazole 20 mg twice daily, amoxycillin 1000 mg twice daily, and clarithromycin 500 mg twice daily, for seven days. Values are mean (95% confidence interval).
Secondary objectives
Relationship between healing of gastritis and symptom relief
There was a statistically significantly higher symptom success rate if gastritis had healed: 31% (78 of 255) of patients with complete healing had a score of 0 or 1 on the severity scale compared with 21% (58 of 280) of patients with incomplete healing (p=0.01, Fisher's exact test, two sided).
Dyspepsia subgroups
As shown in table 2, in the dyspepsia subgroup analysis patients with ulcer-like and reflux-like dyspepsia were more likely to be a responder if H pylori was eradicated (ulcer like, p=0.06; reflux-like, p<0.005) whereas no statistically significant difference was seen in the dysmotility-like dyspepsia group (p=0.263; data in table 2 are grouped by H pylori status). The results were similar if subgroups were correlated with success or failure of treatment in curing H pylori infection. Table 2 shows the pooled data for all the possible definitions of subgroups.
Dyspepsia subgroups, number of patients, and percentage symptom relief in each group and in all combinations (pooled)
Effect of treatment on quality of life
Figure 3 shows that although the average GSRS scores improved over time in the studies, there were no differences between patients treated with OAC and those who received placebo/omeprazole only. In addition, no differences were seen in gastrointestinal related quality of life, as measured by the GSRS, and overall quality of life, as measured by the PGWB index (data not shown).
{kind=link}
{kind=link}
{kind=link}
Average change in gastrointestinal symptom rating scale (GSRS) scores over 12 months. GSRS is expressed as mean item score. The total summary score of the GSRS can be calculated by multiplying the mean item scores by the number of items (n=15). OAC, omeprazole 20 mg twice daily, amoxycillin 1000 mg twice daily, and clarithromycin 500 mg twice daily, for seven days. Values are mean (95% confidence interval).
Effect of treatment on reflux symptoms
Reflux symptoms, as assessed by questions on heartburn and reflux on the GSRS questionnaire, decreased slightly over the 12 month period. There were no differences between the active and control groups, and there was no evidence in the combined analysis for an increase in reflux symptoms following cure of H pylori infection.
Ulcers during follow up
In the ORCHID study, no data were given on ulcers found during the 12 month endoscopy. In the OCAY study, one patient in the antibiotic group had a gastric ulcer compared with six patients with ulcers (four gastric and two duodenal) in the control group.
DISCUSSION
The main conclusion from the ORCHID and OCAY studies is that cure of H pylori does not lead to a sustained improvement in dyspeptic symptoms in patients with investigated functional dyspepsia compared with control patients with persistent infection. The point about investigated dyspepsia is important because in patients with uninvestigated dyspepsia who are H pylori positive (by non-endoscopy based diagnostic tests), there will be a subgroup of patients with true peptic ulcer disease. Such patients are likely to benefit from H pylori eradication treatment.
The results of the combined analysis of the ORCHID and OCAY studies are in direct contrast with the positive results obtained in the studies of Gilvarry and colleagues9 and McColl and colleagues.10 In the study by Gilvarry et al, a symptom score with a range of 0–20 was used to measure outcome.9 The score included an assessment of the frequency and severity of the following symptoms: day pain, night pain, heartburn, flatulence, and nausea. In addition, the attending physicians were asked to divide patients into subgroups of ulcer-like, reflux-like, and dysmotility-like dyspepsia. Gilvarry et al reported the average improvement stratified by whether or not H pylori was successfully cured. They found a statistically significant difference in favour of the H pylori eradicated patients. There was a decrease in summary score from 14 to 9 in patients successfully treated with eradication therapy of bismuth, metronidazole, and tetracycline compared with a change from 14 to 12 in patients in whom the infection persisted. The study did not a priori give a definition of a patient responder. Consequently, they did not report the proportion of patients achieving the desired amount of improvement, as measured on their symptom score. However, the study showed that patients with ulcer-like and reflux-like dyspepsia improved but not patients with dysmotility-like dyspepsia.
The UK Medical Research Council (UK/MRC) trial by McColl et al used a previously validated multidimensional outcome measure to determine treatment success,10 the Glasgow dyspepsia severity score (GDSS). This instrument had previously been validated in patients with duodenal ulcer.11 It assesses the frequency of dyspeptic symptoms, the impact that they have on daily activities, the number of visits to the doctor and diagnostic tests for dyspepsia, and the need for either over the counter medication or prescription drugs to treat the symptoms. In the UK/MRC study, a patient was considered to be a treatment success if the GDSS was either 0 or 1, indicating that the patients had either no or minimal symptoms. In the study, 21% of patients treated with H pylori eradication therapy (14 days of omeprazole, amoxycillin, and metronidazole) had a GDSS of 0 or 1 compared with 7% of patients randomised to omeprazole and placebo antibiotics (p<0.001). Importantly, the GDSS requires patients to rate their symptoms retrospectively over the preceding six month period. This is different from the global scale to assess the severity of dyspeptic symptoms used in the ORCHID and OCAY studies in which patients were asked to complete their responses prospectively on a diary card during the seven days prior to the final study visit. Whether the time frame over which symptoms were assessed to define treatment success is an explanation for the positive results in the UK/MRC trial and the negative results in the ORCHID and OCAY studies is unclear.
The ORCHID and OCAY studies used the GSRS and the PGWB index, both well validated quality of life instruments. The GSRS has been shown to be responsive in patients with duodenal ulcers and GORD, demonstrating significant improvements following treatment.6,7,12 Similarly, the PGWB index has shown consistent changes in response to therapy in patients with duodenal ulcer and GORD.7 Although there were small improvements in both the GSRS and the PGWB index over the course of the ORCHID and OCAY studies, there were no significant differences between the treatment groups.
Most functional dyspepsia studies have shown improvements in symptom severity and quality of life over time.6 As can be seen from fig 1, a lot of the improvement took place early in the ORCHID and OCAY studies. As a normal endoscopy was required as an inclusion criterion, it is certainly possible that the reassurance effect of the endoscopy is the explanation for this early improvement. Patients will have been relieved by the knowledge that no serious disease had been discovered. It has been well documented that concern about disease, particularly the possibility of cancer, is frequently on the minds of patients prior to endoscopy.13,14 In a recent study by Wiklund et al, quality of life was measured using the PGWB index and gastrointestinal symptoms using the GSRS in patients just prior to endoscopy and seven days later.15 In patients in whom no significant endoscopic abnormalities were found, overall quality of life as measured by the PGWB index improved even though there was little change in symptom severity. This supports the concept that endoscopy has a powerful placebo effect through reassurance of patients.
A subgroup analysis was carried out to determine if dyspepsia subgroups help explain why certain patients may respond to treatments and others do not. It is important to stress that subgroup classification was done retrospectively and was based on individual questions from the GSRS. It was shown that patients who fulfilled the criteria for ulcer-like and reflux-like dyspepsia were significantly more likely to be a responder if H pylori was eradicated compared with the control groups. In contrast, no such differences were found in patients who fulfilled the criteria for dysmotility-like dyspepsia. Although this finding coincides with the belief that acid may play a role in the symptom complex of dyspepsia, further prospective studies are needed to confirm that classification into dyspepsia subgroups does help to identify patients who are more likely to respond to H pylori eradication therapy. There are a few other studies in the literature that have reported similar findings9,16 but the sample sizes in these studies were small.
A second subgroup analysis was also performed to determine whether complete healing of the mucosal inflammation of the gastric mucosa was a predictor of treatment success. Using the study definition of healing of gastritis, treatment success was achieved in 31% of patients in whom gastritis had completely healed compared with 21% of patients with incomplete healing. Although these data suggest that healing of gastritis may be an explanatory variable for treatment response, this needs to be confirmed in prospective studies. In clinical practice, it seems unlikely that the severity of gastritis will be a determining factor in deciding whether or not to treat patients with H pylori eradication therapy.
In the OCAY study, seven patients were found to have ulcers during follow up endoscopy. This highlights the fact that a certain proportion of functional dyspepsia patients have a true ulcer diathesis. Such patients are likely to benefit from anti-H pylori therapy.
CONCLUSION
The combined data of the ORCHID and OCAY studies have failed to show a therapeutic benefit with regard to complete or near complete resolution of dyspeptic symptoms, as assessed during a 12 month follow up period. In a subgroup analysis, patients with reflux-like and ulcer-like dyspepsia showed a benefit from treatment over the control groups but this needs further confirmation. The same is true for the observation that complete healing of gastritis increases the chances that a patient will have complete resolution of dyspeptic symptoms.
REFERENCES
Footnotes
-
Conflict of interest: This symposium was sponsored by AstraZeneca, makers of omeprazole. The authors of this paper have received sponsorship for travel and an honorarium from AstraZeneca. NJ Talley has been a consultant and received research grants from TAP, Takeda, Ledede, Pharmacia, and Janssens.