Article Text

Abstract
Introduction Medical training does not necessarily prepare graduates for the real world of healthcare in which continual improvement is required. Doctors in postgraduate training (DrPGT) rarely have the opportunity to develop skills to implement changes where they work. Paradoxically they are often best placed to identify safety and quality concerns and can innovate across organisational boundaries. In order to address this, educational programmes require a supportive educational environment and should include experiential learning on a safety and quality project, alongside teaching of quality improvement (QI) knowledge and systems theory.
Method Enabling Doctors in Quality Improvement and Patient Safety (EQuIP) has been designed for DrPGT at a London children's hospital. The aim is to prepare trainees for the future of continual improvement to ensure safe and effective services are developed through effective clinical microsystems. This paper describes the rationale and design of EQuIP with evaluation built in the evolving programme. EQuIP supports DrPGTs through a QI project within their department, aligned to the Great Ormond Street NHS Foundation Trust's objectives. This changes the way DrPGTs view healthcare as they become quality champions for their department. A three-level approach to the programme is described. The innovation involves a peer-designed programme while being work-based, delivering organisational strategies.
Results Results of the preprogramme and postprogramme evaluations demonstrate an improvement in knowledge, skills and attitudes. Benefits to both the DrPGTs and the organisation are emphasised and key factors to achieve success and barriers identified by the participants.
Discussion The design and evaluation of EQuIP may inform similar educational programmes in other organisations. This capacity building is crucial to ensure that future clinical leaders have the skills and motivation to improve the effectiveness of clinical microsystems.
- Medical education
- Quality improvement
- Health professions education
- Paediatrics
Statistics from Altmetric.com
Introduction
The development of safe and effective services for patients requires strong clinical leadership. Improvement in microsystems in which clinicians work are where ‘real gains in the quality, value and safety of care’ occur.1 Increased awareness and mindfulness at this level is crucial to improve patient safety.1 This paper reports on a programme, Enabling Doctors in Quality Improvement and Patient Safety (EQuIP), which focuses on developing doctors in postgraduate training (DrPGTs) as future leaders for quality and safety. The purpose of the EQuIP programme at Great Ormond Street Hospital (GOSH) for Children National Health Service (NHS) Foundation Trust is to correct a deficit in current medical training. The aim of EQuIP is to enable DrPGTs carry out quality improvement (QI) projects aligned to the organisational objectives of No Waste, No Waits and Zero Harm. The course converts the emphasis on audit to that of improvement, changing the way DrPGTs view healthcare by becoming quality ‘champions’ for their department. The programme is led and coordinated by a DrPGT, and directed by a Medical Director. We describe the rationale and design of EQuIP and the key learning from the evaluation of the programme. The evaluation design was based on a systematic review of teaching QI to clinicians which recommends that future curricula are evaluated based on whether learner's attitudes, knowledge and skills improve, especially when improvements are ‘associated with intermediate clinical gains’.2 The benefits of the EQuIP programme to both the DrPGTs and GOSH will be explored in this article, as well as factors for success of such a programme.
The problem
Roland et al3 argue for educational intervention at an early stage of a doctor's career in order for change to be ingrained in their everyday work. It is essential to train healthcare professionals in improvement skills and to develop the motivation for improvement.4 The two reports, To err is human5 and Crossing the quality chasm6 have stimulated QI training in the USA for undergraduate and postgraduate students. There has also been a focus on DrPGT participation in change initiatives in the UK NHS following the report High quality care for all (2008).7 The General Medical Council (GMC) has highlighted QI activity in doctors’ appraisal and revalidation,8 and the medical Royal Colleges are developing educational strategies to engage DrPGTs in QI.9–11 DrPGTs have shown a growing interest in QI throughout all regions of the UK.12 ,13 They have the potential ability and motivation to improve quality of care for their patients and are in an advantaged position to see where problems lie, understand processes and safety risks and identify feasible, often innovative, solutions.
Improvement skills are required by the NHS leadership competency framework14 and will ensure the development of physician leaders who have the ability to embrace change and improve the quality of healthcare in the future.15–17 Wong et al18 and Hostetter19 called for educational reform to address this need. Training on QI is well accepted by DrPGTs.20 It leads to increased knowledge with improvements in the processes of care. Currently, DrPGTs are mostly not engaged, nor are they invited to participate in QI initiatives within their organisation.21 Although they are often frustrated by the status quo and are keen to make changes to improve patient care,22 they are often not empowered by their supervisors to do so. They rarely meet hospital managers who are usually keen to engage front-line clinical staff in improvement.23
It is our contention that educational approaches to teach DrPGTs improvement methodologies should ensure a supportive environment and include experiential learning on a project, alongside teaching of QI knowledge and systems theory.24 While multidisciplinary collaboration is an essential component for improving quality and safety,4 and therefore was encouraged, this is not the only way to develop a programme aimed at DrPGTs. All project work would be within a team, but the specific needs of DrPGTs in terms of their experiences would not be addressed. The programme was designed solely for DrPGTs at this initial stage, as attitudes toward multiprofessional learning can be mixed.4 It was important to ensure strong engagement in the programme, to reassure the learners that their educational objectives would be met. It was apparent that other disciplines in the organisation had previous exposure to QI learning and that DrPGTs were a group who required attention through a tailored programme. A further advantage was the practical aspect of scheduling and adjusting the timescales around their rotations.
The equip programme
We have designed an innovative programme aligned to local initiatives.25 EQuIP is an educational experience for DrPGTs at GOSH. The innovation is to make learning fun while being work-based. DrPGTs work on real QI projects within their department to help deliver organisational strategies and to prepare them for the future of continual improvement. The appointment of a doctor in postgraduate training, on a 1-year secondment as a leadership fellow, to coordinate EQuIP, was crucial to engage with other DrPGTs on a peer-to-peer level.
Preprogramme evaluation of skills and knowledge
At the start of the programme, DrPGTs working at GOSH completed an online anonymous survey regarding their attitude to, knowledge of and skills in QI. This was designed iteratively by a project team including DrPGTs from different London hospitals, incorporating elements from the Patient Safety Attitudes questionnaire,26 Medical Leadership survey,27 and specific questions designed to assess knowledge of and skills in QI. Results of this survey demonstrated the lack of confidence in and experience of QI, with inaccurate definitions and lack of awareness of tools or appropriate resources (see table 1). Despite a lack of knowledge of and confidence in their own skills, all DrPGTs agreed that clinical leadership is important to the development of the health service (89.7% strongly agreed) and that QI is very important in their practice (74.4% strongly agreed).
Preprogramme survey results
Designing EQuIP: an innovative DrPGT-led programme
The results of the survey informed the design of the EQuIP programme. The need to focus on theory, knowledge and skills of QI through experiential learning and signposting to tools and resources was evident. It also demonstrated DrPGT enthusiasm for engagement in QI. There are three levels to the programme to ensure that all DrPGTs at GOSH could be best engaged (see figure 1).
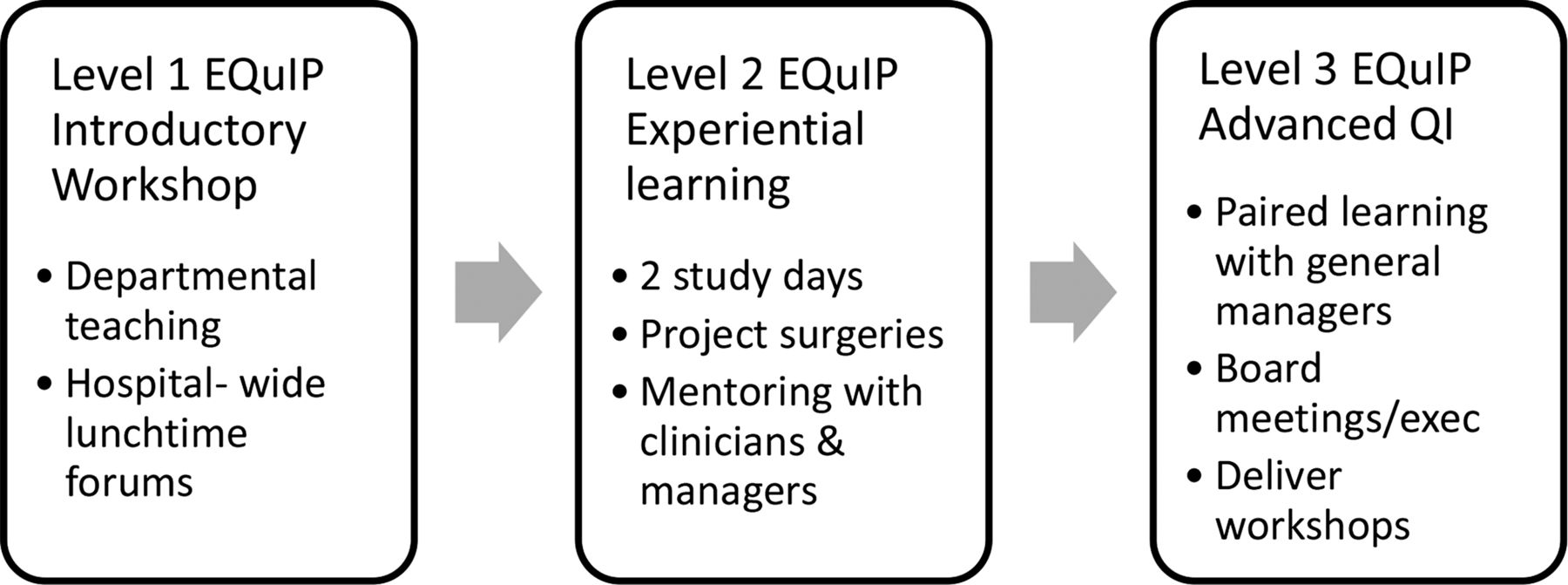
The three levels to the EQuIP programme explained.
Level 1 EQuIP: engaging and inspiring
This 1 h workshop provides an approach to basic methodology focusing on the model for improvement.28 It communicates the message that the organisation values DrPGT engagement in improvement and interprofessional project work to improve patient care. DrPGTs are encouraged to consider potential QI projects of interest and to meet with their departmental managers to ensure their ideas are aligned with the organisation's objectives, not duplicating other work, and to identify other members of a team, if appropriate. All DrPGTs at the Trust were requested to attend this level 1 workshop, although it was not mandatory.
Level 2 EQuIP: educating and supporting
This 6-month voluntary programme includes two full-day workshops, 1 month apart, on improvement methodology and patient safety alongside project surgeries facilitated by improvement managers (managers appointed to the Quality, Safety and Transformation team to lead on improvement work within their clinical division). Topics covered on workshop day 1 include writing a Specific, Measurable, Achievable, Relevant and Time-specific (SMART) aim for their chosen project, applying the Model for Improvement28 to their project, process mapping, driver diagrams, run charts and stakeholder engagement. Day 2 includes fundamental concepts of patient safety and human factors, the importance of clinical leadership (delivered by the hospital medical director), the challenge of change, reliability theory and an interactive afternoon of rapid-cycle feedback on the learner's projects.
Project surgeries, accessible on a twice-weekly basis for up to three learners at a time with managers and improvement leads, allow group reflection and project review and critique throughout the programme. All participants must attend one project surgery between the first two study days and at least three in total. Level 2 participants are allocated a clinical improvement lead (clinician with QI training and responsibility for improvement work in their department) for mentoring. Participants were strongly encouraged to meet the clinical improvement leads on a weekly basis, but this was not a requirement.
Participants are given a precourse reading pack: a selection of leading QI articles from recent journals, including reviews of QI tools and techniques, and lists of resources to seek further information and project guidance. The postcourse survey suggested that all participants had referred to the reading pack; 55% found it very useful, 30% found it somewhat useful and 15% a little useful (4-point Likert scale, from ‘not at all useful’ to ‘very useful’). They are also given access to a free online learning group, which was a simple web-based portal for sharing papers, presentations from study days and for posting useful information throughout the programme.
Level 3 EQuIP: spreading and sustaining
More senior DrPGTs have the opportunity to progress to level 3 training lasting 9 months, acting as a ‘QI champion’ for their department. This allows sustainability of projects in their department through coordinating the handover of projects when colleagues leave and engaging new DrPGTs. There are no additional study days or formal workshops, but this programme includes informal learning on how the organisation functions through meetings with general managers and executive leaders for coaching, and opportunities to attend management meetings, patient safety walkarounds and paediatric trigger tool reviews. DrPGTs consolidate their skills by facilitating level 1 training in their departments, thus helping to engage other DrPGTs and their supervisors in collaborative QI project work.
Innovative interprofessional approach
The innovative approach of this programme is the focus on experiential project learning alongside managers (see figure 2). Rapid-cycle project feedback workshops at the study days and project surgeries have been developed to critique progress and ensure peer learning. This unique aspect, allowing DrPGTs to present their progress (five slides in 7 min maximum, using the following headings: ‘The problem’, ‘Driver diagram’, ‘SMART aim’, ‘Measuring improvement’ and ‘Next steps’) and receive expert and peer input through questioning and group discussion, has been evaluated highly in free text comments in the postprogramme survey. Both participants and facilitators have informally indicated that these presentations with rapid-cycle feedback have been the most successful aspect of the programme.

{kind=link}
{kind=link}
Innovative approach to EQuIP demonstrating structure, process and outcomes.
Results
The first year of this programme has been experimental and has aimed at continual improvement. Benefits to both DrPGTs, the organisation and most importantly, patients, continue to be demonstrated.
Benefit to DrPGTs
Twenty level 1 workshops have been held across different departments since November 2011. Monthly fora continue, with a total of 40 DrPGTs leading their own projects on the level 2 programme. Results of the postprogramme survey have shown an increase in DrPGT confidence in using improvement methodology tools (table 2).
Preprogramme and postprogramme results
In the postprogramme survey, 100% agreed (83.3% strongly agreed) that the project was a valuable learning experience, and 91.7% said they had developed new skills as a result. All respondents said they plan to do another QI project. There are plans to improve the response rate postprogramme, and follow-up the participants in 2–5 years’ time to survey their ongoing involvement in QI initiatives.
DrPGTs were also asked for their three main areas of learning after the level 2 programme. Approximately one-third of responses outlined learning of QI methodologies, including process mapping and Plan-Do-Study-Act (PDSA) cycles, and 10% said they learned most about the benefits and importance of QI. Over half the comments referred to the practical application of knowledge and process of QI. Some of these responses demonstrated awareness of the importance of stakeholder engagement and many referred to learning from challenges they faced in their projects. Preprogramme and postprogramme surveys demonstrated the benefits of this initiative in improving the skills and attitudes of DrPGTs to QI, leadership and patient safety. DrPGTs feel valued and empowered to make changes within their department to improve patient care and have a better understanding of QI.
DrPGTs on EQuIP have had the opportunity to present their work to the Trust executive team, regionally at the Inaugural London Deanery QI conference,25 nationally at The Network casebook event,13 and internationally at The International Society for Quality in Healthcare (ISQua). One EQuIP participant won an award from the Health Foundation, providing funding to continue his project for another year.
Benefit to patients and the organisation
DrPGTs in the EQuIP programme have identified inefficient processes, waste in the system, and issues of patient safety.
Example of EQuIP project
The theatre list for emergency chemotherapy appeared to be running efficiently to the supervising consultants. Previous serious incidents involving the administration of intrathecal vincristine had led to recommendations, which had resulted in some changes. However, one of the EQuIP participants recognised that the smooth running of the list was not reliable. This anaesthetic registrar was frustrated by the chaotic process so worked on an EQuIP project with the clinical nurse specialist and improvement manager. Their aim was to reduce delays and the over-running of the list, both of which are patient safety risks. By accurately measuring the actual length of different procedures, they could modify the theatre list booking form to ensure procedures were allocated to lists appropriately. Team briefings were organised to discuss prioritisation of patients for the list the following day, and the process for preparing patients on the morning of the procedure was standardised. Initial results have shown a reduction in over-running of the list, and there are plans to involve patients and their families in making further improvements.
Examples of success
EQuIP projects have demonstrated evidence of improvement. In the postprogramme survey, 63% of DrPGTs thought the objectives of their project had a significant impact on improving clinical practice and 75% felt they had made a difference to patient care. Table 3 illustrates examples of projects, all of which were aligned to the organisation's objectives of No waste, No waits, Zero harm.
SMART aims and results/progress to date
It was evident that DrPGTs could learn from successes and failures of similar projects in other departments within the Trust as well as outside of the organisation. DrPGTs have had the advantage of working across silos both within their organisation (cross-covering clinical areas on call and at shift handover with DrPGTs from other departments) and outside (rotating through different hospitals every 6–12 months). This high turnover through training rotations ‘makes constant locally relevant re-examination of systems possible’.3
The challenge of change
The implementation of change in healthcare can be a challenge.29 Small changes at a local level with a SMART aim are recommended for DrPGTs on the EQuIP programme, but even these can be challenging.30 Important factors are transitions to new roles, organisational culture, clinical team and leadership support, supervision, working environment and hours and opportunities for ongoing learning. DrPGTs on the EQuIP programme were asked to comment on the factors for success or failure of their projects (see table 4).
Factors for success and barriers to success of projects, identified by EQuIP trainees
Solutions
To address time constraints, the EQuIP programme focuses on DrPGTs who have completed their postgraduate specialist examinations. It offers a flexible approach to study day attendance and project surgery booking. As DrPGTs rotate out of the Trust, the sustainability of projects has been a concern. EQuIP was designed to ensure handover of projects to other trainees by requesting DrPGTs leaving the trust to identify colleagues in their department to join the EQuIP programme and continue their project (levels 1 and 2 workshops were scheduled to coincide with rotation changeover periods). Peer feedback and discussion with other DrPGTs on the programme has ensured transfer of learning across departments within the organisation itself, with spread of improvement initiatives and ideas. This aims to build capacity and future faculty with the appointment of ‘QI champions’.18 ,31
Summary of key factors to achieve success of a QI educational programme for DrPGTs:
-
structured educational programme with experiential project learning
-
innovative approach through peer support and rapid-cycle project feedback
-
senior executive support
-
mentorship by supervising clinicians
-
engagement of improvement managers and operational managers
-
accessible expert advice through open project surgeries
-
flexibility around clinical commitments
-
achievable projects integral to clinical work
Barriers to success of a QI educational programme for DrPGTs:
-
time and clinical commitments
-
poor engagement of clinical teams in improvement work
-
availability of trained faculty for mentoring
-
organisational culture not receptive to change
Conclusion
The investment in training doctors for the future with the skills to lead improvement in all settings is valuable for their future roles and for the organisation. The growing popularity of this programme to both DrPGTs, evidenced by increasing numbers of level 2/3 applicants, and improvement managers, who increasingly refer to EQuIP projects in reports and presentations, is a reflection of the benefits accrued. As a result of this programme, DrPGTs have reported through written and verbal feedback that they feel valued and empowered to make changes within their department to improve patient care. They work alongside managers leading to a better understanding of each other's roles and responsibilities. Preprogramme and postprogramme evaluation has demonstrated an improvement in DrPGT knowledge, skills and behaviour, and participants perceived the programme to be a valuable learning experience. Many individual projects have changed service delivery, with results for the organisation and benefits to patients aligned to the Trust's objectives. This type of programme could be introduced in every healthcare organisation and will accelerate the changes required for the future delivery of healthcare. The skills they have learnt are applicable anywhere in the health service, at any level, and they now have the capacity to inspire and educate others and help prepare for the future.
There is a need to further develop faculty trained in improvement to provide adequate mentoring support for similar programmes.32 This capacity building is crucial to ensure microsystems within organisations are effective. It could be argued that the success of the EQuIP programme may be attributed to the culture of the organisation, with clinical leaders who understand and support QI, and a strong Quality, Safety and Transformation team with engaged improvement managers (many of whom have completed or mentored on TIMP (Transformation Improvement Methodology Programme), a programme for managers, administrative and other clinical staff). A programme such as EQuIP may be more challenging to replicate and sustain in organisations without this culture. However, organisations have much to learn from the ‘frontline’ DrPGTs who work and innovate across organisational boundaries. Cooke et al33 argue that transformation requires new pedagogies in which QI is an integral part of all clinical encounters with health professionals working together to improve patient outcomes and systems of care. QI educational approaches, such as EQuIP which, not only up-skill the future clinical leaders, but motivate them to improve quality of healthcare at a time when morale in the workforce is low, are one step towards this transformation.
Acknowledgments
The authors would like to acknowledge the Quality, safety and Transformation team for their support with coordinating the programme; Kevin Jones for statistical analysis; Dominique Allwood for independently coding qualitative evaluation data; and the EQuIP participants Owen Arthurs, Sophie Swinson, Kerry Robinson, Tom Watson, Susie Goodwin, Ellen Rawlinson, Marianne Elloy, Sanj Gupta, Monica Neil, Kim Ng, Sarah Cowman, Sharon Pickworth, Justin Wakefield, Hannah Bateman, Diana Haider, JJ Kim, Krishna Kotecha, Elise Randle, Henning Clausen, Sainath Raman, Muthana Al Obaidi, Emma Parish, Lisa Brent and Karen Ansell for providing project details for inclusion in this paper.
References
Footnotes
-
Contributors JR and PL designed the EQuIP programme and drafted the paper. BM and JR designed the programme evaluation. JR also analysed the evaluation data and is guarantor. BM revised the paper.
-
Funding The authors would like to acknowledge the support of the London Deanery/NHS London Darzi Clinical leadership Fellowship Programme that provided funding for Dr Jane Runnacles and The London Deanery leadership centre for the initial funding of the programme.
-
Competing interests None.
-
Ethics approval This programme was a quality improvement programme approved by the GOSH QI Committee as per the approved guidelines for QI in the Trust.
-
Provenance and peer review Not commissioned; internally peer reviewed.