Article Text

Abstract
Objective To describe the epidemiology of neonatal infection over the past decade in UK neonatal units.
Design Retrospective analysis of prospectively collected infection surveillance network data from 2005 to 2014.
Setting 30 neonatal units in the UK.
Patients Newborns on participating neonatal units who had a positive blood, cerebrospinal fluid or urine culture and were treated with at least 5 days of appropriate antibiotics.
Results 2171 episodes of neonatal infection in 1922 infants were recorded. The incidence of infection was 6.1/1000 live births and 48.8/1000 neonatal admissions (2.9 and 23.5 respectively if coagulase-negative staphylococci (CoNS) cultures excluded). The incidence of infection showed a statistically significant reduction over time with reductions in the rates of both early-onset sepsis (EOS) and late-onset sepsis (LOS).
The majority of episodes (76%) represented LOS (diagnosed > 48 hours after birth), and infection was more common in premature (<37 weeks gestation) and low birth weight (<2500 g) neonates (84% and 81%, respectively). Commonly identified pathogens included group B streptococci (43%) and Escherichia coli (18%) for EOS, while E. coli (15%), Staphylococcus aureus (14%) and CoNS were prominent causes of LOS.
Conclusions This paper describes the epidemiology of neonatal infection in the UK over the past decade. These data enable benchmarking of practice and inform areas of future research and guideline development. The results support the hypothesis that the introduction of infection prevention care bundles and antibiotic stewardship programmes in the UK has reduced the burden of LOS.
- infectious diseases
- epidemiology
- neonatology
- intensive care
Statistics from Altmetric.com
What is already known on this topic?
Neonatal infection is an important cause of morbidity and mortality, particularly in low birth weight and preterm infants.
A comprehensive and up-to-date understanding of the epidemiology of infection is essential as it may change over time and differ between countries.
Neonatal infection surveillance networks have been successfully established in multiple countries and are used to benchmark practice, establish prescribing guidelines and improve quality of care.
What this study adds?
The incidence of neonatal infection in UK neonatal units has declined over the past decade.
This decline suggests an impact of interventions such as central-line care bundles and intrapartum antibiotic prophylaxis guidelines.
This decline was not seen in neonatal intensive care units without surgical facilities.
Introduction
Neonatal infection is a significant cause of morbidity and mortality in the UK and worldwide, particularly in low birth weight (LBW) and preterm infants.1–3 The causative pathogens may change over time and between countries.4
Neonatal infections are classically divided into two distinct clinical syndromes: early-onset sepsis (EOS) and late-onset sepsis (LOS).2 3 This classification guides choices on empiric antimicrobial treatment.5 A comprehensive understanding of the epidemiology is essential in order to inform clinical practice and ensure adequate empiric antimicrobial coverage of the pathogens encountered.5
The use of neonatal infection surveillance networks has proved to be a successful method for defining the epidemiology of neonatal sepsis in many countries including the USA, Canada, Australia and Germany.6–9 There are, however, differences in the protocols followed by different surveillance networks; the German7 and USA9 networks have focused on VLBW babies cared for in tertiary neonatal units and include both culture-proven sepsis and presumed and possible sepsis. Definitions of sepsis also vary between networks but all consist of a combination of clinical and laboratory parameters. Nevertheless, such networks provide valuable insights into the longitudinal epidemiology of infection, enable benchmarking of practice, and allow assessment of the effectiveness and appropriateness of empiric antibiotic prescribing guidelines.4 6 10 Additionally, it has been shown that these networks can improve the quality of care within hospitals and reduce rates of infection.7
neonIN is a neonatal infection surveillance network that was established in 2004 with the objective of collecting and storing information about the pathogens which cause neonatal sepsis and their antimicrobial resistance patterns on a longitudinal basis. neonIN data from 2006 to 2008 were published in 2010 and showed an infection incidence of 8/1000 live births (LB) and 71/1000 neonatal admissions (NA) (4.1 and 38 respectively if coagulase-negative staphylococci (CoNS) excluded).4
The aim of this analysis was to update these results and describe the epidemiology of neonatal infection over the past decade in the neonIN infection surveillance network. Data regarding antimicrobial resistance levels in the neonIN database have been published separately.11
Methods
neonIN collects data on episodes of neonatal infection. An episode of neonatal infection is defined as a positive culture collected from a normally sterile site such as the blood, cerebrospinal fluid (CSF) or urine (obtained in a sterile manner) for which clinicians prescribed at least 5 days of appropriate antibiotics. Data are collected using a standardised online questionnaire completed by the clinician for each positive culture result.
Repeatedly positive samples are considered to represent the same episode of infection unless they occurred more than 7 days after the last positive culture result (or 10 days in the case of CoNS or fungal infections). EOS is defined as infection occurring less than 48 hours after birth with episodes thereafter being classified as LOS.
During the study period, 30 neonatal units contributed infection data to the neonIN database. All UK neonatal units were able to participate in this network but were required to make a commitment to contribute high-quality data in a consistent manner. The 30 participating units are based in all parts of England and Wales (see map: www.neonin.org.uk) ensuring good geographical representation.
Neonatal units are designated as local neonatal units (LNUs) (those able to provide full care for neonates more than 27 weeks gestation at birth), or neonatal intensive care units (NICUs) (those specialised in caring for the sickest and most premature infants), according to the criteria of the British Association of Perinatal Medicine.12
Data regarding the total number of LBs and NAs are collected via the online neonIN database. Where denominator data were not entered by a hospital, the figures were extracted from the ‘National Neonatal Audit Programme – Annual Report’ of the appropriate year.12
Data were extracted and analysed in Stata V.14 with statistical significance being defined as a P value of <0.05. A number of statistical tests were used during the analysis process including:
Two-sample Student’s t-tests for comparisons of normally distributed continuous data,
Wilcoxon Mann-Whitney tests for comparisons of continuous data that were not normally distributed,
Χ2 tests for comparisons of categorical data if all data were >5 (or Fisher’s exact tests if not),
Simple linear regression for analysis of relationships between continuous predictor and outcome variables,
Simple logistic regression for analysis of relationships between a predictor variable and a binary outcome variable.
A complete account of the statistical methods is included as an online supplementary document.
Supplementary file 1
Analyses were conducted with and without the inclusion of CoNS, as these are well-recognised potential contaminants of blood cultures. This is particularly so for EOS cultures as CoNS are believed to be extremely unlikely causative pathogens of EOS.
Results
Data were extracted for the 10 years between 1 January 2005 and 31 December 2014. The number of UK units contributing to neonIN increased over this period with the total number per calendar year being 5 in 2005 then 8, 9, 12, 14, 16, 20, 24, 29 and 30 in each subsequent year. Of the participating units, 7 (23%) were LNUs and 23 (77%) were NICUs. Neonatal surgery was provided in 48% (11/23) of the NICUs.
All infections (excluding CoNS)
A total of 2171 episodes of neonatal infection were recorded in 1922 infants over the study period, with 24% of cases (n=514) representing EOS. Infection occurred more frequently in male (n=1089, 57%) than female infants (n=833, 43%; P<0.001 (Χ2 test)). Of the 197 infants (10%) to experience more than one episode of infection, 74 (38%) did so with the same pathogen. Multiple organisms were isolated from the same culture in 4% (n=93) of episodes.
The majority of cases (n=1813, 84%) were premature infants (<37 weeks gestation) of whom 87% (n=1569, 73% of all cases) were born at less than 32 weeks. Likewise, 81% (n=1742) of affected infants were LBW (<2500 g) with 86% (n=1506, 70% of all cases), 68% (n=1180, 55%) and 41% (n=717, 33%) of these being <1500 g (very low birthweight) (VLBW), <1000 g (extremely low birthweight) (ELBW) and <750 g, respectively.
The age at disease was not influenced by gender (P=0.74), but varied significantly by pathogen. GBS had a peak incidence on the first day of life (day 0), while Escherichia coli demonstrated two peaks between days 0–3 and 5–10. Staphylococcus aureus demonstrated a broad peak between days 6 and 12, while Enterobacteriaceae and Enterococcus sp. followed no distinct patterns. The distribution of the most frequently isolated pathogens over the neonatal period is shown in figure 1.

Incidences of common pathogens causing infections in 30 neonatal units in the neonIN network. Shown by postnatal age over the neonatal period (28 days). CoNS, coagulase-negative staphylococci.
The vast majority of episodes were identified by a positive blood culture (n=1961, 91%). However, pathogens were isolated from CSF cultures in 41 cases (mean postnatal age=19 days, 90% (n=37) >48 hours). The source of the remaining pathogens was primarily urine (n=113, 5%) of which 98% were LOS cases with the most common pathogens being Candida sp. (n=34, 30%), Enterococcus sp. (n=23, 20%) and E. coli (n=17, 15%).
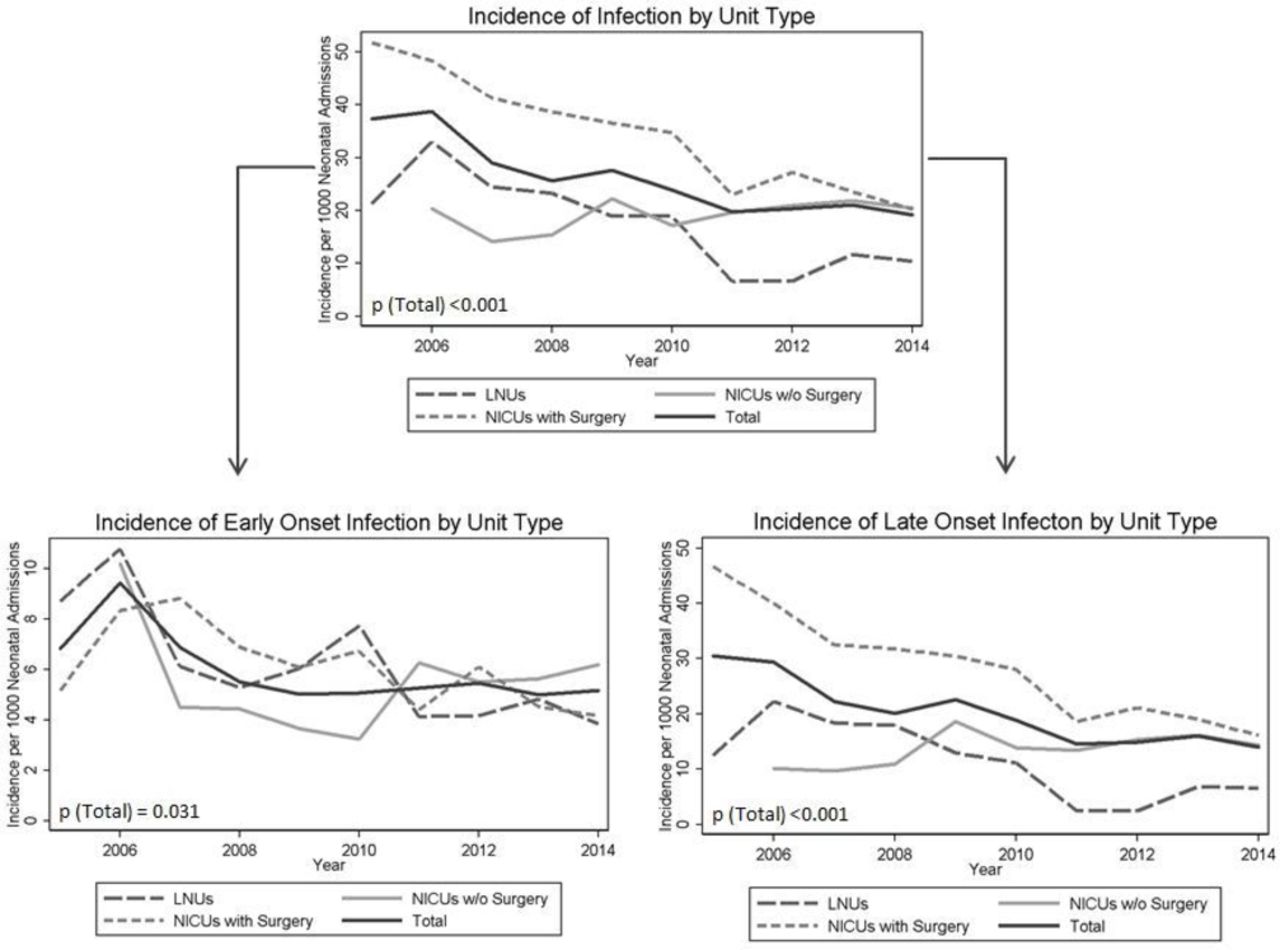
The overall incidence of infection (excluding CoNS) was 2.9/1000 LBs and 23.5/1000 NAs. The highest incidence was found in the surgical units (3.6 and 30.3, respectively). Linear regression analysis revealed a statistically significant reduction in the overall incidence of infection by both LBs and NAs over the study period (P<0.001 for both). This trend was observed for both LNUs (P=0.005) and NICUs with surgery (P<0.001). However, NICUs without surgical facilities demonstrated a statistically significant increasing trend (P=0.041) (figure 2).
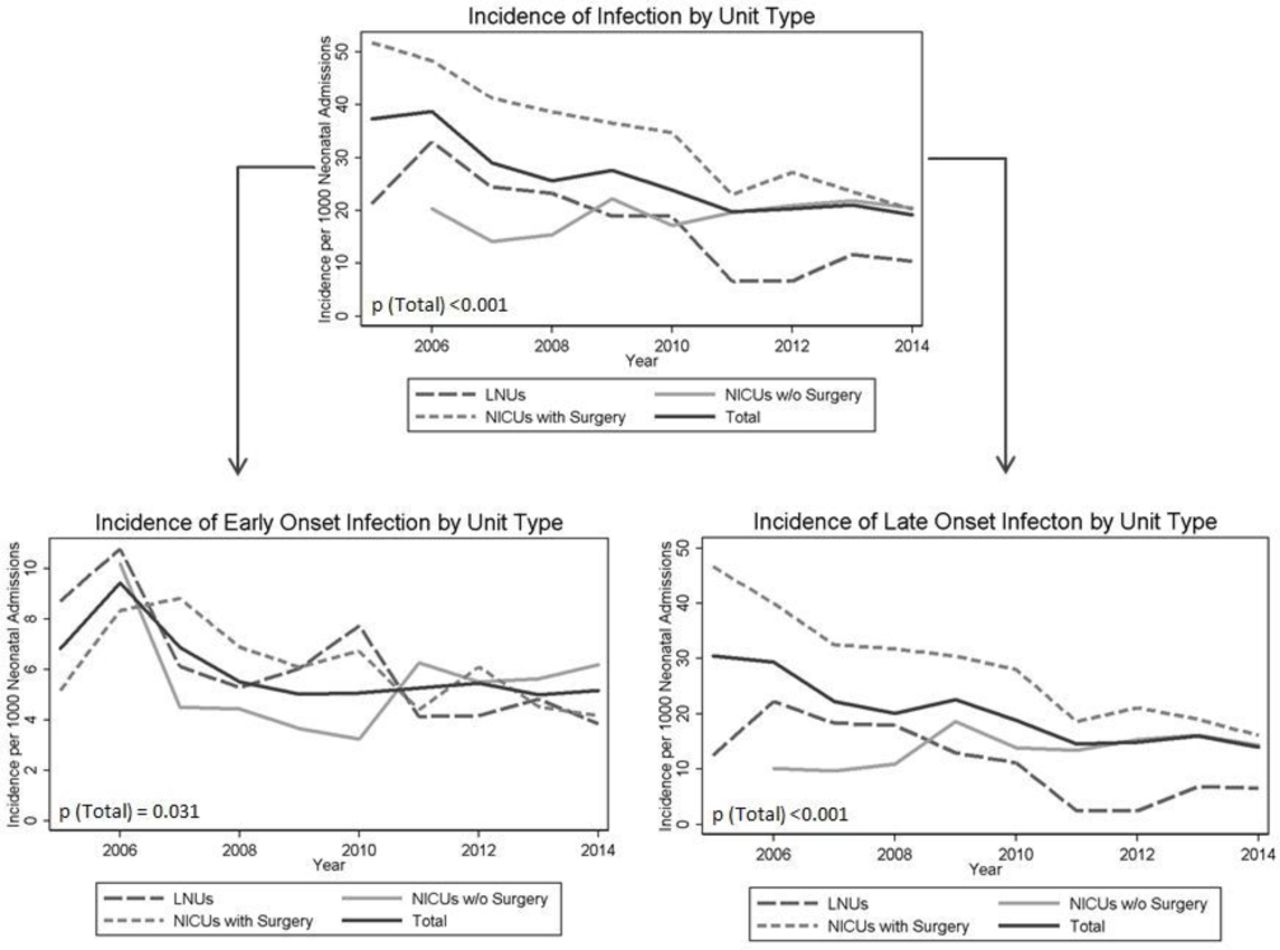
Incidence of infection over the neonIN study period, shown by type of neonatal unit. Incidences calculated per 1000 neonatal admissions. LNU. local neonatal unit; NICU, neonatal intensive care unit.
Early-onset sepsis
EOS incidence was 0.7/1000 LBs and 5.6/1000 NAs. A statistically significant downwards trend was noted over the study period (P=0.031 (linear regression)) (figure 2). A large proportion of EOS cases were diagnosed in term infants (>37 weeks) (n=213, 42%). Likewise, 50% (n=251) of affected infants weighed >2500 g with only 32% (n=164) of babies being <1500 g (VLBW).
Of the 514 episodes of EOS, 74% (n=379) were caused by Gram-positive (GP) organisms, 25% (n=130) by Gram-negative (GN) organisms and the remaining 5 cases by Candida sp. (n=4) and Mycobacterium sp. (n=1). Group B streptococcus (GBS) was the most frequently isolated organism (n=221, 43%), while E. coli comprised 18% (n=95) of cases. Infants with EOS GBS infection had a median birth weight of 3026 g (IQR=2088–3618) and a gestational age at birth of 38 weeks (35-40).
A comparison of EOS pathogens using 48 and 72 hours cut-offs revealed that there was no significant difference between these two thresholds either with respect to individual pathogens (P>0.20 (Χ2 and Fisher exact tests used as appropriate)) or overall (P=0.087) (online supplementary table S1). Furthermore, extending the EOS period proportionally made the most difference to S. aureus (+27%), a pathogen more commonly associated with LOS, and least difference to GBS and Listeria which are both associated with vertical transmission.
Supplementary file 2
The incidence of EOS GBS over the study period was 0.30/1000 LBs and 2.39/1000 NAs. This increased to 0.33/1000 LBs when a 7-day cut-off for EOS was applied. Over time, the EOS GBS incidence demonstrated a statistically significant decrease (P=0.004 (linear regression)), falling from 0.45/1000 LBs in 2005 to 0.29 in 2014. Interestingly, while linear regression revealed a significant decreasing trend in the incidence of premature infants with EOS GBS (P=0.046), the incidence in term infants showed no significant trend over time (P=0.161).
Late-onset sepsis
The median postnatal age for late-onset infection was 20 days (IQR=10–42 days). The overall incidence of LOS over the study period was 2.2/1000 LBs and 17.9/1000 NAs and demonstrated a statistically significant downwards trend (P<0.001 (linear regression)) (figure 2).
LOS was primarily diagnosed in premature infants (<37 weeks gestation) (n=1519, 92%) with 91% (n=1379, 84% of all cases) of these occurring in those <32 weeks. Similarly, 90% (n=1487) of affected infants were LBW (<2500 g) with 90% (n=1342, 82% of all cases), 72% (n=1074, 65%) and 44% (n=654, 40%) of these being VLBW, ELBW and <750 g, respectively.
Overall, GP organisms accounted for 45% of the 1657 cases of LOS (n=751) with GN making up 45% (n=748), and fungi the remaining 10% (n=158). S. aureus was the most commonly isolated GP pathogen (n=233, 31%), while E. coli was the most frequent GN (n=241, 32%) and Candida albicans the most prevalent fungus (n=100, 63%) (table 1).
Causative pathogens of late-onset sepsis found in 30 UK neonatal units in the neonIN network
CoNS infections
There were 2408 episodes of CoNS infection involving 2169 infants. The overall incidence of infection (including CoNS) over the study period was 6.1/1000 LBs and 48.8/1000 NAs.
The majority of CoNS episodes presented as LOS (93%, n=2233), representing 57% of all recorded LOS cases. CoNS infection primarily occurred in extremely premature (<32 weeks) and ELBW infants (83% and 62%, respectively) (P<0.001 for both (Χ2 tests)), and was isolated almost exclusively from the blood (98%).
Age at disease by pathogen
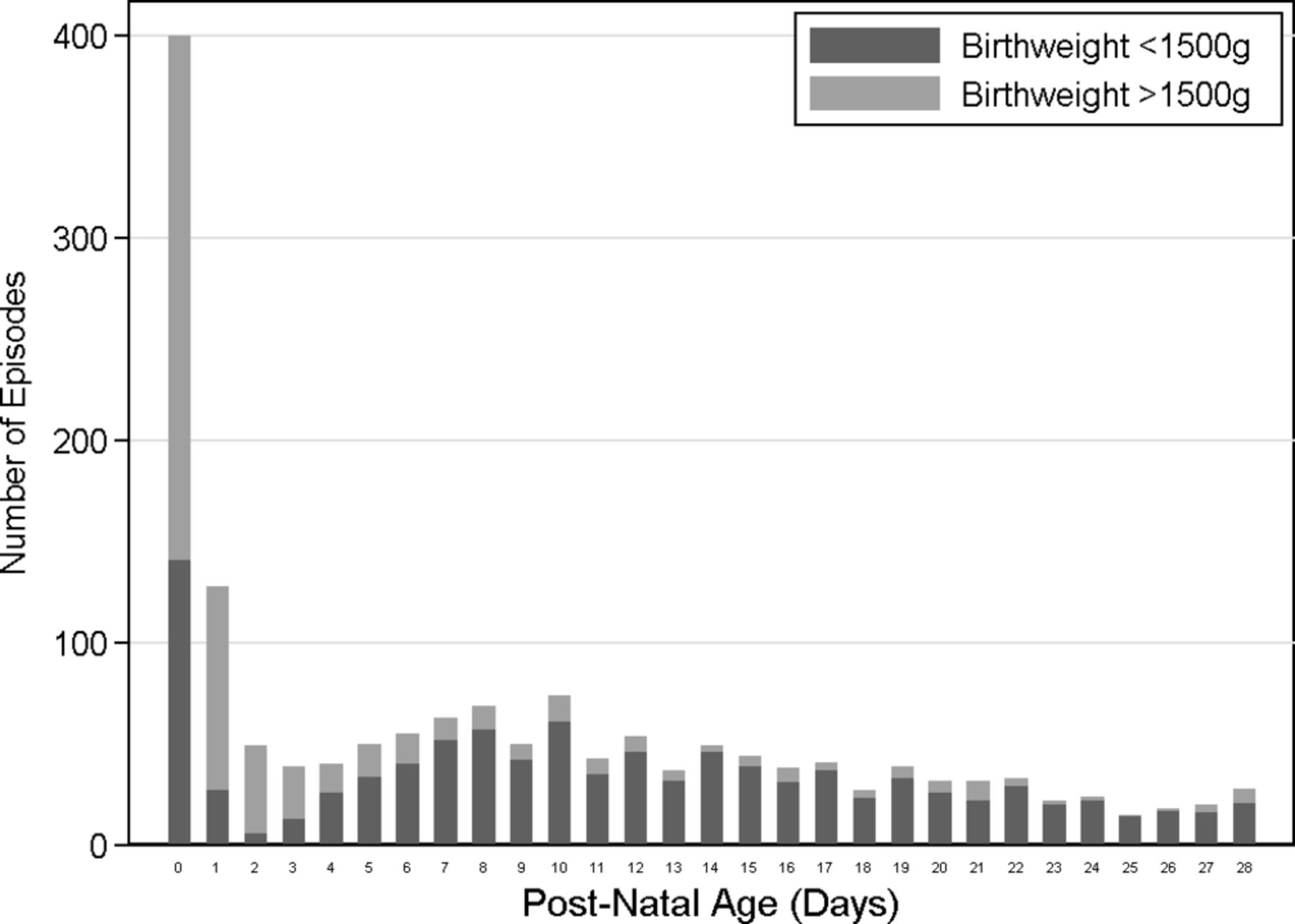
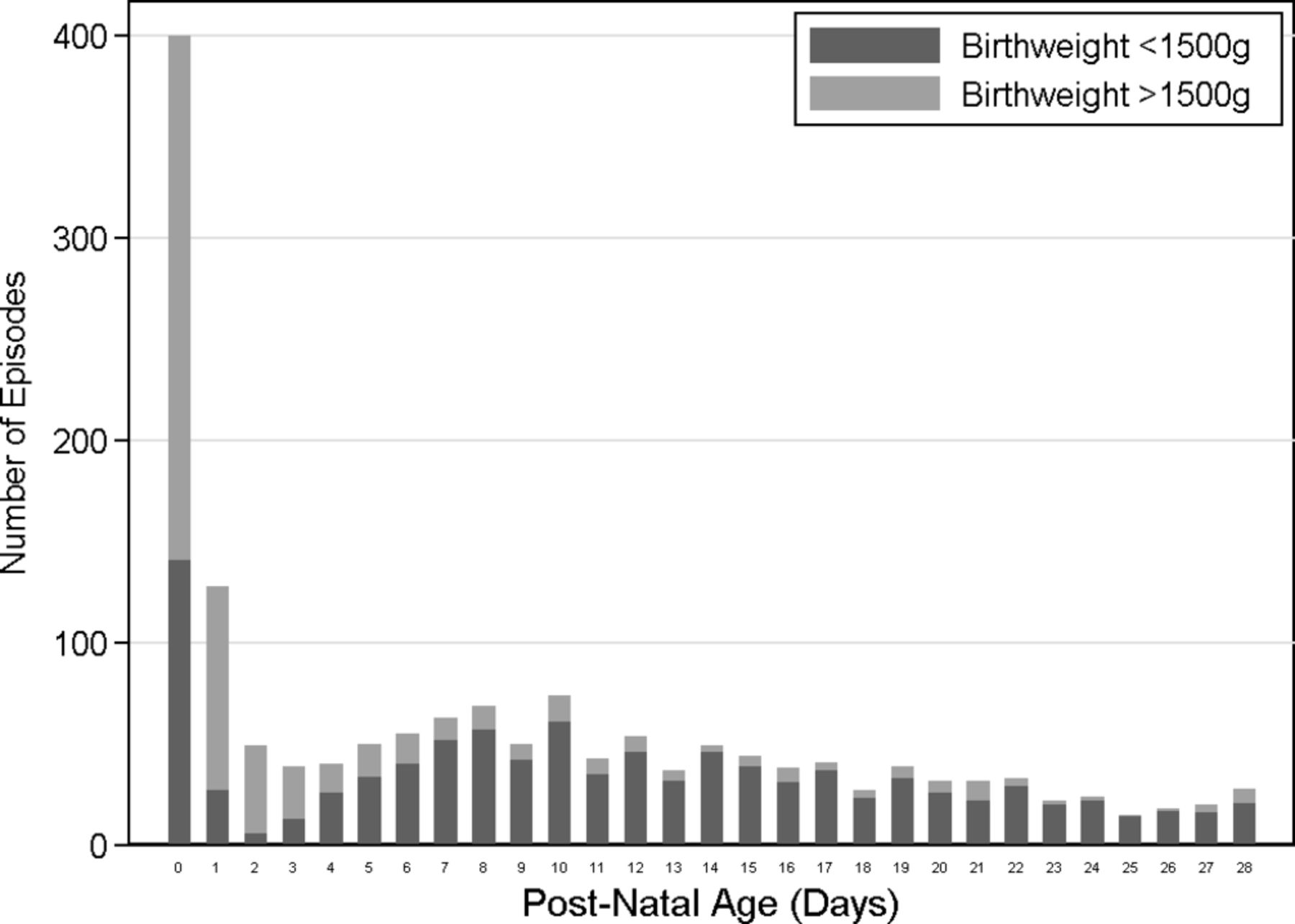
Roughly a quarter of all neonatal infections represented EOS with the vast majority of these (76%) occurring on the first day of life. EOS infection was highly associated with a birth weight of >1500 g or a gestational age of >32 weeks (69% and 63%, respectively) (P<0.001 for both (χ2 tests)), whereas the vast majority of cases of LOS occurred in infants <1500 g (82%) and <32 weeks (83%) (P<0.001 for both). The later the onset of infection, the stronger the associations with gestation and birth weight (P<0.001 for both (linear regression analyses)) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Proportion of infections occurring in neonates <1500 g in 30 neonatal units in the neonIN network. Shown by day of infection over the neonatal period (28 days).
Discussion
This study shows that preterm and VLBW infants carry the highest burden of infection, particularly LOS. These results are consistent with the existing literature.3 4 13 14 Infection was also significantly more common among males (56%), an association that has been well described.1 4 The reason for this association remains unclear but likely reflects the preponderance of male gender among preterm births in general.15
Comparisons can be made between the neonIN-derived data and those of several other studies from the UK and internationally. A single-centre study by Haque et al 16 reported a comparable incidence of neonatal infection while a laboratory surveillance programme throughout England and Wales reported a similar distribution of pathogens.17 Comparisons with previous neonIN analyses reveal a slightly lower incidence of infection in the current study and a similar pathogen distribution.4 The increased proportion of NICUs in the early years of the neonIN database and the decreasing overall incidence of infection are two factors which may explain this discrepancy. For these reasons, the data in this study supersede those previously published.
US and Australian studies report consistently higher rates of E. coli and fungal infections, although this is partially compensated by lower rates of GBS and CoNS.8 18–21 It is possible that much of this difference relates to different approaches to GBS screening and intrapartum antibiotic prophylaxis (IAP) use in these countries.4 8 18 21 Comparisons of LOS incidence with that of the German NeoKISS22 system reveal similar incidences of infection among VLBW infants and a similar distribution of pathogens, although overall Neo-KISS demonstrates a higher prevalence of S. aureus and Enterobacter sp. and a lower prevalence of E. coli and Enterococcus sp. than neonIN.22 This reinforces the necessity of having local surveillance networks for informing clinical practices and optimising neonatal care.
There was a decreasing trend in the overall incidence of infection (P<0.001). This was accounted for by decreases in the rates of both LOS (P<0.001) and EOS (P=0.031). It is possible that the decreasing trend in LOS is the result of implementation and adherence to programmes focusing on the prevention of late-onset hospital-acquired infections; a significant initiative in UK healthcare facilities over the past decade.23 24 However, not all European neonatal units have seen such a decline, leading to a call for greater adherence to interventions including hand-hygiene policies and central-line care bundles.23–26
EOS reflects vertical transmission of maternal pathogens and its incidence will be affected by other factors.1 The major pathogen that contributes to EOS is GBS, and a statistically significant downward trend was noted in its incidence over the study period (P=0.035).1 27 This might reflect the introduction of risk-based IAP protocols in the UK in 2003.21 28 29 As neonIN only includes infants admitted to neonatal units, any impact may be limited to premature infants with GBS, who form a minority of the total burden of GBS disease. This hypothesis is supported by the fact that neonIN infants with EOS GBS had a lower median birth weight and gestational age (3026 g and 38 weeks) than those in the recent national surveillance study (3300 g and 39 weeks).30 The decreasing incidence in preterm but not term infants is also consistent with the findings of this study and may reflect a tendency for clinicians to particularly target IAP towards certain groups of preterm births, as recommended in the recent National Institute for Health and Care Excellence antibiotic for early-onset infection guidelines.31
The reduction of infection incidence was not seen in all unit types but only in the LNUs (P=0.005) and the NICUs with surgical facilities (P=0.001). NICUs without surgery demonstrated an increased incidence over the same period (P=0.041). These opposing trends are intriguing and require further analysis; one possible explanation is the transition of the UK hospital system to a ‘network-based’ system from 2004 to 2007.32 This resulted in reduced neonatal admissions of infants <27 weeks in LNUs and a corresponding increase in admission rates of these very premature babies to the associated NICUs within the same networks.32 This hypothesis may be supported by the observation that there was a trend towards a reduction in the proportion of infants <27 weeks gestation in LNUs over the study period (P=0.083).
Debate exists over what represents the most appropriate cut-off point for EOS, with 48 and 72 hours the most commonly used alternatives.4 10 This study found no statistically significant increase in the pathogens captured by a 72-hour cut-off when compared with 48 hours. The validity of a 48-hour cut-off is also shown by the finding that the majority of pathogens observed between 48 and 72 hours were those normally associated with horizontal (nosocomial) transmission (eg, S. aureus and enterococci).4 5 Furthermore, GBS, the the most common EOS pathogen and one known to be vertically transmitted, displayed the smallest proportional increase.28 29
The primary strength of the neonIN database is its size and longitudinal design. A number of limitations of this study however must also be acknowledged. First, the infection definition may be considered too simplistic or subjective given its reliance on the clinician’s judgement that a treatment course should be given. This subjectivity may lead to over-reporting of cases, particularly of common skin contaminants such as CoNS. An alternative would be to incorporate more clinical and laboratory markers into the study definition, but it is essential that the infection definition remains simple or it will affect the completeness and quality of the data entered.
Second, it is important to note that some neonates have more than one recorded infection episode, with repeat infections representing 11% of all infection episodes. While it is possible that these events may therefore not be independent of one another, these represent positive cultures that have occurred after the previous infection has been treated with a minimum of 5 days of appropriate antibiotics. Furthermore, 62% of these cultures grew a different pathogen to that isolated in the original infection episode. These therefore still represent distinct episodes of infection which are important to consider when we look at the overall epidemiology.
It is also important to note that the varying number of neonatal units contributing data per year creates a potential source of bias as it is possible that the decreasing rate of infection may be influenced by the addition of new units with lower incidence rates. However, of the six most consistently reporting neonatal units over time, four demonstrated a decreasing trend in infection incidence, three of which were significant trends. We therefore believe that while this is a potential limitation of these data, the decreasing trend in infection is still most likely representative of the overall database. Data completeness is another potential limitation of neonIN as it relies on voluntary reporting of infection episodes by hospital staff.6
This study provides unique insights into the epidemiology of infectious diseases in neonates in the UK. It describes the incidence of infection in UK neonatal units and the relative prevalence of the causative pathogens. The results support the hypothesis that the introduction of infection prevention care bundles and antibiotic stewardship programmes in the UK has reduced the burden of LOS. These data inform areas of future research and guideline development which work towards addressing better health outcomes in our neonatal populations.
References
Footnotes
Contributors BC and CK contributed to the design of the analysis, conducted the analysis of the data, drafted the manuscript and revised it according to feedback from co-authors. PH developed the neonIN network, designed the current analysis and provided critical appraisal as well as final approval of the manuscript. JB, SP, AG, JM, AR and NK made substantial contributions to the acquisition of data for the analysis, critically revised the manuscript and provided final approval for the version to be submitted. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval The neonIN database received ethics approval from the London-Surrey Borders Research Ethics Committee in April 2005 (05/Q0806/34) and this was extended in December 2013 (05/Q0806/34+5) for a period of 5 years.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data from this study are available only to members of the neonIN team and may form part of future analyses. Generalised statistics however are freely available on the neonIN website at https://www.neonin.org.uk/.
Collaborators neonIN network collaborators: Medaht Ezzat; Marion Bohatschek; Clare Cane; Imogen Storey; Sam Wallis; Ruppa Geethanath; Jonathan Campbell; John Chang; Timothy Watts; Olga Kapellou; Suzanne Luck; Mark Turner; Sakina Ali; Edward Gasiorowski; Mithilesh Lal; Nick Embleton; Paul Clarke; Sajeev Job; Mark Anthony; Tim Scorrer; Shanmuga Sundaram; Andrew Collinson; Nigel Osborne; Mike Hall; Elizabeth Pilling; Leika Hamilton; Gaurav Atreja; Jonathan Davis; Peter Reynolds; Prakash Satodia