Article Text

Abstract
Objective Leukaemia is the most common cancer of childhood, accounting for a third of cases. In order to assist clinicians in its early detection, we systematically reviewed all existing data on its clinical presentation and estimated the frequency of signs and symptoms presenting at or prior to diagnosis.
Design We searched MEDLINE and EMBASE for all studies describing presenting features of leukaemia in children (0–18 years) without date or language restriction, and, when appropriate, meta-analysed data from the included studies.
Results We screened 12 303 abstracts for eligibility and included 33 studies (n=3084) in the analysis. All were cohort studies without control groups. 95 presenting signs and symptoms were identified and ranked according to frequency. Five features were present in >50% of children: hepatomegaly (64%), splenomegaly (61%), pallor (54%), fever (53%) and bruising (52%). An additional eight features were present in a third to a half of children: recurrent infections (49%), fatigue (46%), limb pain (43%), hepatosplenomegaly (42%), bruising/petechiae (42%), lymphadenopathy (41%), bleeding tendency (38%) and rash (35%). 6% of children were asymptomatic on diagnosis.
Conclusions Over 50% of children with leukaemia have palpable livers, palpable spleens, pallor, fever or bruising on diagnosis. Abdominal symptoms such as anorexia, weight loss, abdominal pain and abdominal distension are common. Musculoskeletal symptoms such as limp and joint pain also feature prominently. Children with unexplained illness require a thorough history and focused clinical examination, which should include abdominal palpation, palpation for lymphadenopathy and careful scrutiny of the skin. Occurrence of multiple symptoms and signs should alert clinicians to possible leukaemia.
- Haematology
- Oncology
Statistics from Altmetric.com
What is already known on this topic?
Serious illnesses such as cancer are rare in children in primary care (about 1 in 200 children) and are easily missed.
Leukaemia is the most common cancer of childhood, with 4000 new cases annually in the USA and 450 in the UK.
What this study adds?
Over 50% of children with leukaemia have palpable livers, palpable spleens, pallor, fever or bruising on diagnosis.
Abdominal symptoms are not typically included in national cancer guidelines for identifying children with leukaemia, yet are present in 29% (anorexia/weight loss), 12% (abdominal pain) and 11% (abdominal distension) of children, respectively.
Important common musculoskeletal and bleeding manifestations are also omitted, such as mucosal bleeding (25%), joint pain (11%) and limp (15%).
Introduction
In developed countries, cancer causes more childhood deaths than any other serious illness, including meningitis.1 Leukaemia is the most common malignancy of childhood, with an annual incidence of nearly 4000 in the USA and 450 in the UK, and is responsible for a third of childhood cancer deaths.2 ,3 Yet paediatric leukaemia is a low-prevalence disease in primary care, emergency departments and general paediatrics settings. A general practitioner, for example, is likely to encounter a child with cancer only once every 20 years.4 The early presentation of paediatric leukaemia, with non-specific symptoms often mimicking the common, self-limiting illnesses, complicates the diagnostic challenge faced by front-line clinicians.5 ,6
Improving the early diagnosis of cancer is a key priority for many health services. The UK's National Health Service Cancer Plan, for example, stipulates that all patients with suspected cancer, including children, should be seen by a specialist within two weeks of referral.7 Subsequent guidance from the National Institute for Health and Care Excellence (NICE) details a range of specific signs and symptoms that should alert clinicians to consider cancer in children and, in the case of leukaemia, take blood or immediately refer.5 Despite these attempts, the vast majority of cancers in children are still not diagnosed via the 2-week urgent referral pathway. In one recent study, 98% of childhood cancers in the UK were identified by other routes, such as direct presentations to emergency departments or non-urgent hospital referrals from primary care.8
In order to improve our understanding of the early presentation of paediatric leukaemia, we aimed to systematically identify and collate all existing data on its presenting signs and symptoms at, or before, the point of diagnosis.
Method
Search strategy
We searched MEDLINE and EMBASE from inception to December 2014 using a combination of subject headings and free text incorporating the terms ‘leukaemia’ and ‘diagnosis’, and limited to infants, children and adolescents. Reference lists of included studies were also searched for potentially relevant studies. No language restrictions were applied. The complete search strategy is detailed online (see online supplementary appendix eSearch).
Study selection
We considered for selection all primary research studies, either retrospective or prospective, of any study design (eg, cohort), describing the frequency of signs and symptoms at time of diagnosis for a minimum of 10 children (0–18 years) with any type of leukaemia. Duplicate studies were removed. Studies that selected cases based on the presence of only certain clinical features of leukaemia (eg, only musculoskeletal or gastrointestinal manifestations) were excluded to avoid giving disproportionate weight to those features in the data synthesis. We also excluded studies that reported data on both adults and children, but where we were unable to extract the paediatric data. Any uncertainties regarding studies selection were discussed between the authors.
One researcher (RTC) screened titles and abstracts of all papers, excluding clearly irrelevant studies. Two researchers (RTC and MJT) independently reviewed the full text of remaining papers to assess eligibility.
Quality assessment
Once we had assembled a shortlist of studies eligible for potential inclusion using the criteria above, two reviewers (RTC and MJT) independently assessed the risk of bias in these studies' results to ensure that only those studies with an acceptable risk of bias were included in this review (see online supplementary eTable1). There is no single, well-validated quality checklist for assessing retrospective cohort studies, and so we constructed a checklist based on relevant items from the MOOSE (meta-analysis of obeservational studies in epidemiology) reporting guideline for observational studies,9 the STROBE (strengthening the reporting of observational studies in epidemiology) reporting guideline for cohort studies,10 the Newcastle-Ottawa scale for non-randomised studies11 and CASP (critical appraisal skills programme) guidelines for case–control and cohort studies.12 ,13
Quality was assessed as ‘acceptable’ or ‘unacceptable’ in three domains: definition of leukaemia, selection of cases and methods for extracting data on included cases. ‘Acceptable’ for case definition required cases to be defined according to bone marrow findings. ‘Acceptable’ for case selection required at least two of participants' baseline characteristics clearly documented; characteristics of cases representative of children with that type of leukaemia (ie, the age and sex distribution of cases matched the known epidemiology of paediatric leukaemias); and the sample comprising all consecutive cases over the study period or, if non-consecutive, reasons for omission of cases documented. ‘Acceptable’ for data extraction required use of a standardised data collection proforma and/or the objective measurement of signs (eg, ultrasound confirmation of suspected organomegaly). Disagreements between the two reviewers were discussed with a third reviewer (AVDB). Only studies considered by all reviewers to pass in two or more domains were included in this review.
Data extraction
Data were extracted from included studies by one reviewer (RTC) using a standardised proforma and checked by a second reviewer (MJT). We extracted study characteristics including period of study, number and type of centres, study design, recruitment methods, sample size and age of children. Presenting signs and symptoms were recorded as described in each study, and numbers of children presenting with each feature noted. When a symptom or sign was not recorded in a study, no assumption was made about whether or not that feature had occurred in that population (ie, we did not assume that absence of recording was equivalent to absence of that feature). Authors cross-checked each others' data extraction to ensure accuracy. We did not contact authors of included papers for missing information.
Statistical analysis
We used STATA V.11.1 to calculate simple proportions and SEs of proportions for each presenting feature in each included study. Where considered clinically appropriate, features that the authors considered similar were aggregated (eg, ‘petechiae’, ‘purpura’ and ‘petechiae/purpura’ were combined into a single category, ‘petechiae/purpura’). Features were not aggregated when it was not clinically sensible or when they were reported with insufficient clarity to avoid possible double counting.
We calculated pooled proportions of children presenting with each feature using the metan command. Anticipating high heterogeneity between included studies, we performed random-effects meta-analysis using the DerSimonian and Laird method and standard methods to calculate I2 as an estimate of the heterogeneity. In addition, we conducted three a priori subgroup analyses to explore reasons for heterogeneity and generate new hypotheses: (1) type of leukaemia; (2) year of publication and (3) income status of the country in which the study was performed, as defined by the Organisation for Economic Cooperation and Development criteria at the time the study was conducted. We conducted subgroup analyses based on type of leukaemia, country income level and publication date of study as, based on the existing literature, we felt that these might plausibly affect the speed of presentation of children, accessibility of health, care and changes in health-seeking behaviour, as well as the possibility of different clinical features depending on leukaemia type. We used exactly the same technique, DerSimonian and Laird, as for the main analyses.
Results
Search results
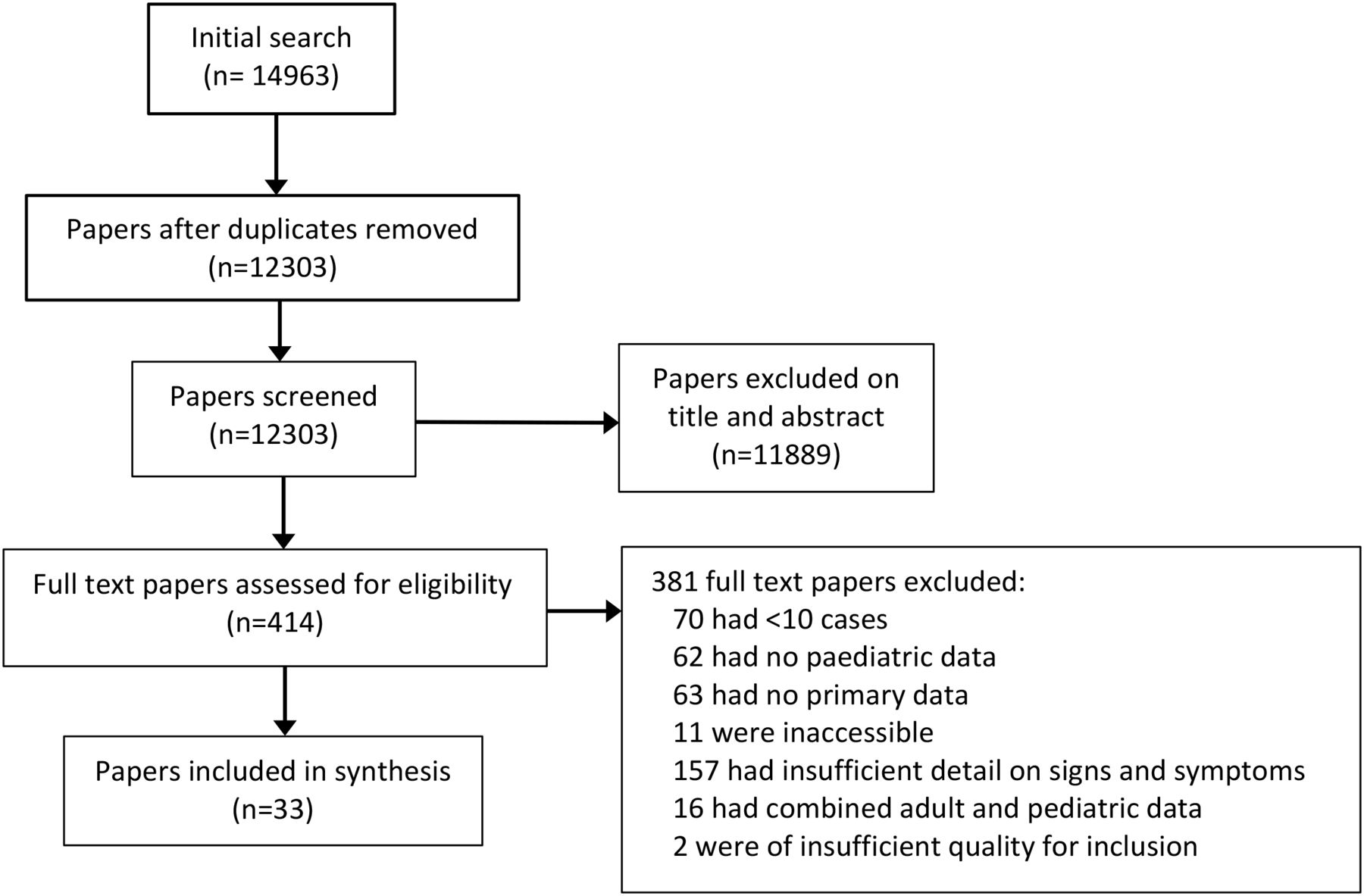
After removal of duplicates, we identified 12 303 papers. We excluded 11 889 after screening titles and abstracts, and a further 381 after full-text assessment (figure 1). Reference lists of included studies did not yield additional eligible studies. There were no differences between authors regarding whether a particular study should be included.

Flow chart for selection of studies.
Characteristics of included studies
Thirty-five studies met the eligibility criteria and were considered for inclusion, with two of these being excluded on quality grounds, as detailed below (see online supplementary appendix eTable1). The 33 included studies14–42 were conducted in 21 countries and described presenting symptoms and signs in a total of 3084 children (table 1). All were retrospective cohorts of between 10 and 406 participants, and none compared cases with controls.
Characteristics of included studies
The majority of studies (n=26) identified cases from medical records alone; others also used national and regional registries of childhood leukaemias (n=4), death certificates (n=2), pathology reports (n=1), clinical trial data (n=1) and primary care records (n=1). All 33 studies extracted data from written hospital records. One study also obtained data from primary care records,41 and another supplemented hospital records with data from a patient and/or parent-completed questionnaire.42
Risk of bias of included studies
All included studies defined cases using bone marrow criteria and clearly documented participants' baseline characteristics such as age and sex, which were consistent with the known epidemiology of paediatric leukaemias (see online supplementary appendix eTable1). Only 13 studies (39%) included all consecutive cases within the study period, with a further 3 studies (9%) describing why a proportion of potentially eligible cases were excluded. In the remaining 17 studies (4%), the proportion of consecutive cases included was unclear.
One weakness of the included studies was lack of clarity about how the list of clinical features of leukaemia was generated and at which point in the diagnostic pathway clinical features were recorded. Fifteen studies explicitly stated that they reported signs and symptoms occurring ‘at diagnosis’, while two studies also reported symptoms from the point of symptom onset through to diagnosis. The remaining 16 studies were unclear as to whether the symptoms reported occurred at and/or prior to diagnosis.
Pooled frequencies of symptoms and signs from meta-analysis
The number of different signs and symptoms reported in individual studies ranged from 6 to 23 (median=11). Overall, 95 separate signs and symptoms were reported. We were able to aggregate 15 features into 6 overarching categories. These were petechiae/purpura (category derived from ‘petechiae’, ‘purpura’ and ‘petechiae/purpura’), mucosal bleeding (including ‘mucosal bleeding’ and ‘bleeding gums’), anorexia/weight loss (including ‘anorexia’, ‘weight loss’ and ‘anorexia/weight loss’), weakness/fatigue (including ‘weakness’, ‘fatigue’, ‘weakness/fatigue’), malaise/fatigue (including ‘malaise’ and ‘malaise/fatigue’) and infections (including ‘infection’ and ‘recurrent infections’).
In total, 55 out of a possible 86 meta-analyses were conducted. For the remaining 31 features, meta-analysis was not required since the features were each present on only one study. The high heterogeneity (I2) statistics in the meta-analyses (usually >90%) indicated that the degree of heterogeneity between studies was greater than that expected by chance alone and confirmed the appropriateness of random-effects meta-analysis to generate pooled proportions (figure 2).

Frequency of signs and symptoms present in ≥10% in children with leukaemia. URTI, upper respiratory tract infection.
The 36 features that were present in ≥10% of children are shown in figure 2. We grouped these features into seven distinct clinical categories according to main underlying pathological process or body system affected: infiltrative, haemorrhagic, infective, systemic, musculoskeletal, gastrointestinal and cutaneous. The most common infiltrative symptoms were hepatomegaly (64%) and splenomegaly (61%). Bruising, the most common haemorrhagic symptom, occurred in 52% of children. Fever (53%) was the most common infective symptom, and the most prominent musculoskeletal features were limb pain (43%) and bone pain (26%). Systemic features such as pallor (54%) and fatigue (46%) were also common. Finally, the most common gastrointestinal feature, anorexia/weight loss (29%), was present in almost a third of children. Those features reported in a third or more of children are summarised in table 2, while those reported in <10% of children are included in online supplementary appendix eTable2.
Signs and symptoms present in more than one-third of children with leukaemia
There were no data on the frequencies of combinations of symptoms, nor any data from control children. Nor was it possible to extract data on the timing of specific features, such as which presented first and last.
Subgroup analyses
There were 14 specific features for which it was possible to calculate presenting frequencies across the subgroups ‘acute’ and ‘chronic’ leukaemia (figure 3). Certain features of acute illness, such as fever, were more common in acute leukaemia (62%, CI 51 to 73) than chronic leukaemia (31%, CI 13 to 49), whereas certain more progressive, infiltrative features, such as splenomegaly, were more prominent in chronic leukaemia (77%, CI 62 to 92) than acute (56%, CI 40 to 73). Studies from high-income settings also showed a greater prevalence of splenomegaly (76%, CI 67 to 85) compared with that in moderate-income/low-income settings (51%, CI 36 to 64). Conversely, other clinical features, such as fever, pallor and anorexia/weight loss, were more common in low-income/moderate-income settings (70%, CI 62 to 77, 73%, 15 to 52, 43%, CI 14 to 73, respectively) than in high-income settings (37%, CI 26 to 47, 34%, CI 15 to 52, 22%, CI 15 to 28, respectively). All three of the planned subgroup analyses (ie, by leukaemia type, publication date and income status of country) exhibited high heterogeneity, and most I2 statistics were >90% (online supplementary appendix eTable3). We cannot exclude the difference in prevalence being due to confounding factors other than the subgroup criteria we selected.

{kind=link}
{kind=link}
{kind=link}
Frequency of signs and symptoms in children according to leukaemia type.
Discussion
Principal findings
We identified >90 different presenting clinical signs and symptoms in children diagnosed with leukaemia. At time of diagnosis, >50% of children with leukaemia had palpable livers, palpable spleens, pallor, fever or bruising, concurring with those features identified in current NICE guidance as potential alert symptoms for leukaemia.5 Our study also highlights several important potential omissions in NICE guidance. Abdominal symptoms, such as anorexia/weight loss (prevalence 29%), abdominal pain (12%) and abdominal distension (11%), do not feature in the NICE referral pathway for leukaemia. Nor do some of the haemorrhagic manifestations of leukaemia, such as mucosal bleeding, particularly from gums (25%). Instead, the guidance highlights only bruising and petechiae. Our results suggest this might be better replaced by ‘unusual bleeding’ phenomena to include all bleeding manifestations. Finally, although persistent/unexplained bone pain is highlighted in NICE guidance, other musculoskeletal manifestations of leukaemia, such as limp (11%), joint pain (15%) and functional impairment (23%), are unrepresented.
Strengths and weakness
This is the first systematic review to describe how leukaemia presents in childhood. It collates data from >3000 children in 33 studies from 21 different countries. Our review adhered to rigorous methods, including a systematic search strategy, unrestricted by date or language, and explicit inclusion criteria.46 The findings therefore present the most comprehensive and internationally relevant data on presenting features available for clinicians worldwide.
The main limitations of the study reflect deficits in the design and reporting of the included studies. Although studies primarily collected contemporaneous data from medical case notes, all were conducted retrospectively. Given that included studies provided data on cases only, and not on controls, we were unable to determine diagnostic accuracy of clinical features. The high heterogeneity between included studies, which was not accounted for by our a priori subgroup analyses, is unsurprising, given the lack of detail in most studies about how the list of presenting features was derived. Without this, it is difficult to account for variations between studies in either the number of included features reported (which ranged from 6 to 23) or their frequencies. Additionally, the meta-analysis is complicated by inconsistent, vague or ambiguous language used in individual studies to describe signs and symptoms (such as ‘bleeding tendency’). Conversely, some of the terms used clearly overlap to some degree (such as ‘bruising’, ‘bruising/petechiae’, ‘cutaneous bleeding’, ‘cutaneous/mucosal bleeding’, ‘petechiae/purpura’, all of which may or may not be identical to ‘bleeding tendency’ in leukaemia), which contributed to the analyses of an unwieldy 97 different presenting features.
Comparison with existing literature
Systematic reviews of the presentation of other main childhood cancers (such as central nervous system tumours) have also highlighted gaps in current protocols and guidelines that need to be addressed in updated guidelines.47 Qualitative studies indicate that even those symptom lists identified from systematic reviews may be incomplete since they may fail to capture the full range of parent-reported symptoms, in which behavioural and affective changes in children feature prominently.48
Implications for practice
Some of the most commonly presenting features we identified, such as fever, pallor and fatigue, also feature prominently in the presentation of many common, self-limiting diseases of childhood and are therefore unlikely to assist front-line clinicians in discriminating between those children who do or do not have leukaemia. Others—hepatomegaly, splenomegaly, lymphadenopathy and petechiae, for example—are more specific for leukaemia, and hence of greater value as potential red flags. Our findings emphasise the importance, in any child with unexplained illness, of a focused clinical examination that should include abdominal palpation, examining for lymphadenopathy and careful scrutiny of the skin. Abdominal palpation can be particularly challenging in children under 5 years, the peak presenting age group for paediatric leukaemia, but a palpable liver or spleen is an important red flag that should prompt urgent referral for further investigation.
The lack of evidence on combinations of clinical signs and symptoms is disappointing as research in other domains, such as serious infections in children, has shown that combining relatively non-specific features may result in useful prediction rules.49 We suggest that any child presenting with unusual symptom clusters, for example, bruising and fever or limb pain and pallor, should warrant an active search for other corroborative clinical features and consideration of a full blood count and blood film.
Implications for future research
Our study highlights three key limitations in the current evidence base for how paediatric leukaemia presents, which are priorities for future research in this area. First, we have no data on the frequency and time of onset of symptoms from the point of onset of the first symptoms at home, through to final diagnosis. Second, we do not know how frequently different symptom clusters occur and whether different clusters occur at different time points in the illness trajectory prior to diagnosis. Third, we cannot estimate the diagnostic accuracy of individual or combinations of clinical features as none of the studies included data on control children. Large-scale cohort studies using electronic routine data from primary care and hospital settings would address these gaps, though such studies are likely to be biased towards signs and symptoms already known to have a relation with leukaemia.47 An alternative and complementary approach could use qualitative methods to explore patients', parents' and clinicians' accounts of the diagnostic process, generating a richer understanding of the potential determinants of delay.
Acknowledgments
The authors gratefully acknowledge the work of Nia Roberts in conducting the literature searches for this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors RTC and MJT conceived and designed the study. RTC collected the data, which RTC and MJT analysed. RTC wrote the first draft of the manuscript, and all authors contributed to subsequent drafts. RTC is the guarantor.
Funding This report is independent research arising from a Career Development Fellowship supported by the National Institute for Health Research.
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The following are freely available as supplementary appendices: (1) full search strategy, (2) quality assessment of included studies, (3) signs and symptoms in <10% of children and (4) subgroup analyses.