Article Text

Abstract
Background: The previous epidemiological study of paediatric nephrolithiasis in Britain was conducted more than 30 years ago.
Aims: To examine the presenting features, predisposing factors, and treatment strategies used in paediatric stones presenting to a British centre over the past five years.
Methods: A total of 121 children presented with a urinary tract renal stone, to one adult and one paediatric centre, over a five year period (1997–2001). All children were reviewed in a dedicated stone clinic and had a full infective and metabolic stone investigative work up. Treatment was assessed by retrospective hospital note review.
Results: A metabolic abnormality was found in 44% of children, 30% were classified as infective, and 26% idiopathic. Bilateral stones on presentation occurred in 26% of the metabolic group compared to 12% in the infective/idiopathic group (odds ratio 2.7, 95% CI 1.03 to 7.02). Coexisting urinary tract infection was common (49%) in the metabolic group. Surgically, minimally invasive techniques (lithotripsy, percutaneous nephrolithotomy, and endoscopy) were used in 68% of patients.
Conclusions: There has been a shift in the epidemiology of paediatric renal stone disease in the UK over the past 30 years. Underlying metabolic causes are now the most common but can be masked by coexisting urinary tract infection. Treatment has progressed, especially surgically, with sophisticated minimally invasive techniques now employed. All children with renal stones should have a metabolic screen.
- nephrolithiasis
- renal stones
- metabolic
- epidemiology
- risk factors
Statistics from Altmetric.com
The last British epidemiological study of paediatric nephrolithiasis, performed in 1973,1 concluded that stones were principally secondary to urinary tract infections, particularly Proteus, that recurrence occurred if there was inadequate eradication of infection,2 and that open surgery was the favoured treatment option. To examine if these findings are still relevant we have studied children presenting to the same centres over the past five years.
METHODS
Since 1997, all children presenting with a renal stone to either Great Ormond Street Hospital or St Peter’s Hospital (within the Middlesex Hospital) were referred for a metabolic evaluation. Each child was reviewed by a consultant paediatric nephrologist (WVH) in a dedicated paediatric renal stone clinic, using a specific list of questions and a standard metabolic screen. All children were screened with a plasma urea, creatinine, potassium, sodium, chloride, bicarbonate, magnesium, calcium, phosphate, alkaline phosphatase, albumin, and urate. Their second voided urine was analysed for infection by formal microscopy and culture, and sent for determination of calcium, urate, oxalate, cystine, and creatinine (by standard laboratory methods). Where possible, stones were analysed in a recognised laboratory for chemical composition. We undertook a retrospective audit of the first five years of this service (January 1997 to December 2001).
Medical and surgical modalities of treatment were obtained retrospectively from the hospital notes. One hundred and twenty one patients were included in the study; two were omitted due to inadequate patient details. Patients were classified as having a metabolic predisposition for stone formation according to the following criteria:
-
Hypercalciuria. Non-fasting, spot urinary calcium:creatinine (Ca:Cr) ratio analysis was compared to the 95th centile of age specific, Western society reference values (table 1).3 If the child was old enough to cooperate, a 24 hour urine was collected; hypercalciuria was diagnosed if the calcium excretion was >4 mg/kg/day (0.1 mmol/kg/day).4 A child who had a raised Ca:Cr ratio that returned to normal after stone removal was excluded.
-
Hyperoxaluria. A raised spot oxalate:creatinine (Ox:Cr) ratio greater than the 95th centile age related normal reference values (birth 0.2 mmol/mmol; 5 years 0.14 mmol/mmol; 10 years 0.085 mmol/mmol; 15 years 0.06 mmol/mmol)5 was used as an initial screen. Repeated abnormalities were confirmed by a 24 hour urine collection into an acidified container6 and urine was also sent for determination of urinary glycolate and l-glycerate concentrations. In cases with persistent hyperoxaluria, primary hyperoxaluria was suspected and a liver biopsy performed to determine levels of alanine glyoxylate aminotransferase (for primary hyperoxaluria type 1) and glyoxylate transferase reductase (for type 2).
-
Cystinuria. Quantitative urinary amino acid determination by ion exchange chromatography showed levels of cystine above 18 mg/g creatinine7 together with isolated increases of the other dibasic amino acids (ornithine, lysine, arginine).
-
Hyperuricosuria. Repeated increased spot urines of urate:creatinine level greater than age specific reference values (1.6 mmol/mmol at <6 months of age decreasing to 0.4 mmol/mmol in adolescence).8 These were then confirmed with 24 hour collections against age specific references.9
Random non-fasting urinary calcium:creatinine ratios; 95th centile reference range
The aetiology of the stone was considered infective if no metabolic abnormality was detected and the child presented with, or had a past history of urinary tract infection (UTI). Stone formation was termed idiopathic if there was no preceding history of UTI and no metabolic abnormality.
Statistics
When comparing groups for risk factors, odds ratios with 95% CI were used in the Instat software package. In defining the population characteristics the median age was used as this was considered most representative.
RESULTS
Incidence, age, and sex at presentation
One hundred and twenty one patients (82 boys and 39 girls; 2.1:1 boys:girls), were included over the five year period (fig 1). The median age of presentation was 36 months for males (range 3–180 months) and 48 months (range 4–137 months) for females.

Age at presentation, sex distribution, and aetiological type of paediatric stones presenting to Great Ormond Street and the Middlesex hospital 1997–2001. (A) Males (n = 82). (B) Females (n = 39).
Presenting features
Presentation with the classic combination of renal colic and macroscopic haematuria was uncommon. Sixty six (55%) children had macroscopic haematuria, 61 (50%) abdominal pain, but only 36 (30%) patients had both symptoms. In 21 (17%) patients the stones were apparently asymptomatic and fortuitously detected. Interestingly the median height and weight of children on presentation was lower than average, on the 25th centile in 93 children (77%) who were measured (range 0.4th to 91st centile).
A positive family history of renal stones was present in 19 (16%) first degree relatives, rising to 40 (33%) if both first and second degree relatives were considered. Sixteen (13%) children were born prematurely (<37 weeks), and in 10 (8%) there was a history of prolonged immobility, principally secondary to neurological impairment. In 58 (48%) there was a previous history of urinary tract infection. This study did not aim to address the frequency of congenital renal anomalies in the children with stones. However, at least eight (7%) were known to have vesicoureteric reflux, six (5%) had stenosis within the urinary tract, and one child bilateral renal cortical cysts (the cause of which remains under investigation). Of these 15, three were defined as metabolic, four infective, and eight idiopathic stone formers.
Aetiology
Fifty three (44%) had an underlying metabolic abnormality, 36 (30%) were classified as having an infective aetiology, and in 32 (26%) no aetiological factor could be detected. Metabolic stone formers presented throughout childhood, in contrast to infective aetiologies which were more common in the under 6 age group, with 89% presenting in this period (fig 1).
Metabolic aetiologies
Of the 53 patients with a metabolic abnormality: 30 had hypercalciuria (57%), 12 cystinuria (23%), one hyperuricosuria (2%), five intermittent hyperoxaluria (9%), four primary hyperoxaluria (8%), and one child an unclassified hypercalcaemic condition (2%).
Within the hypercalciuric group, one child from a consanguineous marriage had the hypomagnesaemia, hypercalciuria (Michaelis-Manz) syndrome.10 Immobility and prematurity contributed to eight cases. The remainder had idiopathic hypercalciuria, with no other obvious exacerbating factors such as calciuric inducing medications. Interestingly, of these, 48% had a family history of nephrolithiasis. One child had persistent hypercalcaemia and an inappropriately raised parathormone level, but repeatedly normal 24 hour and spot urine calcium excretion (the underlying diagnosis in this boy is under ongoing investigation).
The hyperoxaluric group consisted of four children with primary hyperoxaluria: three with type 1 and one child with non-type 1/type 2 (none had type 2). Four children had enteric hyperoxaluria secondary to small bowel pathology. Three of these were born prematurely, two of whom had bowel resections for necrotising enterocolitis. One child who was born at term had bowel resected for a rhabdomyosarcoma. The single child with uric acid stones underwent further investigation of the purine metabolic pathways but no underlying defect was detected.
Excluding the single patient with hyperuricosuria, between 45% and 58% (total mean 49%) of children with each of the defined metabolic abnormalities had presented with a urinary tract infection. Children with a metabolic abnormality presented at a median of 40 months (range 3–168 months) compared to 36 months (range 6–180 months) in the infective/idiopathic group. There were proportionally more males in the infective/idiopathic (male:female, 2.6:1) compared to the metabolic group (male:female, 1.7:1). The risk of presenting with bilateral stones was increased significantly in children with an underlying metabolic abnormality, with 14 of 53 (26%) having bilateral stones in the metabolic group compared to 8 of 68 (12%) in the non-metabolic group (odds ratio 2.7, 95% CI 1.03 to 7.02)
Infective stones
These occurred in 36 patients with a median age of presentation of 30 months. The male to female ratio was 1.6:1. Boys presented at an earlier age than girls (median of 24 months compared to 48 months). Two children with multiple stones had xanthogranulomatous pyelonephritis, resulting in chronic renal failure.
Stone distribution
The stones were upper tract in 104 children (86%), unilateral on the left in 44 (36%), on the right in 38 (31%), and bilateral in 22 (18%). In four cases (3%) the stones were located in the bladder, and in seven (6%) in both the bladder and upper tract. In six (5%) the stones were passed, before determination of location.
Stone composition
The majority of stones analysed were composed of calcium oxalate or calcium phosphate (50%). Triple phosphate stones were detected in 32%; however in two cases (3%) of those analysed, the stone consisted of both triple phosphate and cystine, and both these children had cystinuria. These were diagnosed by virtue of their urinary investigations. In 44% of children stone analysis could not, or was not, undertaken (usually because they had undergone lithotripsy before metabolic evaluation and no fragments were available).
Stone removal
One hundred and eight (89%) children underwent a procedure to remove the stone(s) (fig 2). Commonly, a combination of techniques was used to achieve stone clearance. In 25 (21%) cases open surgery alone was performed. A review of the surgical management of a subset of these patients (treated between 1997 and 1999) has recently been presented.11
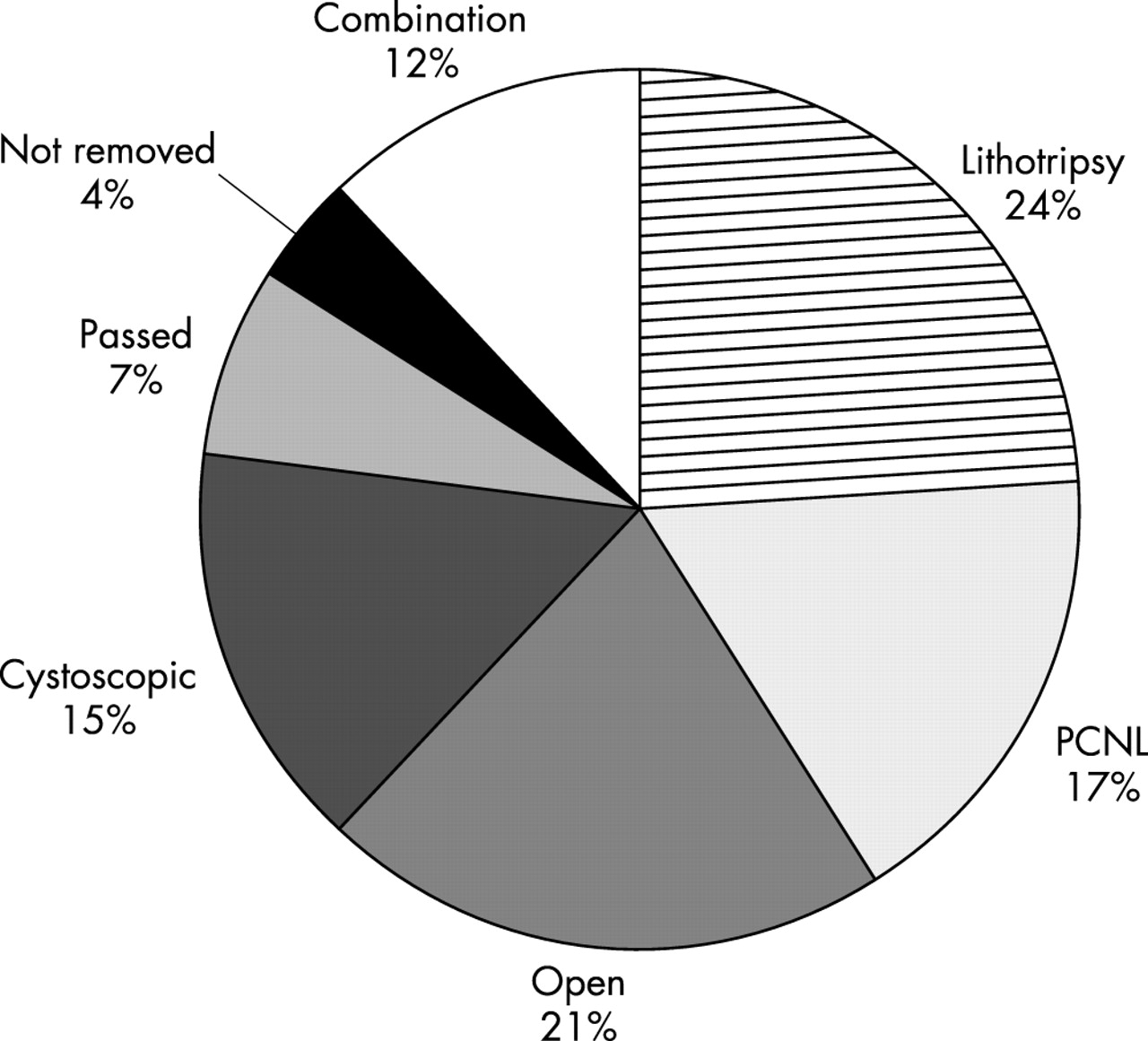
Surgical modalities of stone removal (n = 121).
DISCUSSION
The epidemiology of paediatric nephrolithiasis appears to have changed in the past 30 years. This study does not address whether the incidence of stone disease in children has changed, which has been reported to account for between 0.13 and 0.94 cases per 1000 hospital admissions in the western world,12 but does indicate an apparent change in the aetiology of stone formation. Males continue to suffer more renal stones than females, a predominance that is confirmed in some13–15 but not all16 paediatric series from elsewhere in the world. Most stones affect the upper tract as has been noted in the UK since the industrial revolution.12,17
Diagnosing stone disease is known to be difficult13,16,18 as the presentation in children can frequently be atypical (only 50% children in this study were perceived to have had pain). In 17% the stone was detected fortuitously. We observed that children presenting with renal stones often have feeding and growth problems. The reduced mean height and weight (on 25th centiles) in the sample (77%) measured prior to stone removal, may support this observation, although reduced growth after prematurity or other concurrent illness may also be contributory factors.
The most striking difference that we have observed is the apparent reduction in the proportion of infective stones and the increase in underlying metabolic abnormalities from 16% thirty years ago1 to 44% today (fig 3). In this study, we investigated every child, even if they presented with a UTI or had a triple phosphate stone. In previous studies some of these children may have been labelled as having “infective” stones. Our data suggests that a high proportion (49%) of such children have an underlying metabolic abnormality. Although urinary tract infection can lead to stone formation, the presence of a stone can itself also lead to a UTI. As in the previous study, we excluded transient hypercalciuria as this is commonly associated acutely with the stone episode and disappears after the stone is removed.1,19 It is also possible that the reduced proportion of children with infective stones is related to the increased awareness, identification, and rapid treatment of urinary infection in children.21 For whatever reason, it seems that the apparent incidence of underlying metabolic abnormalities found, using the diagnostic criteria of this study, is now similar to those found in parts of the United States16,21–23 and other countries throughout the world.24

{kind=link}
{kind=link}
{kind=link}
Underlying stone aetiologies. Comparison between previous study (1966–71) and present study (1997–2002).
Identifying the underlying metabolic abnormality is beneficial as it seems to predict more severe stone disease; these patients are more than twice as likely to present with bilateral disease compared to the infective/idiopathic group. It also permits the opportunity to identify siblings who have similar pro-lithogenic metabolic abnormalities to be detected before they develop overt stones. This allows treatment to be initiated early to help prevent stones forming.
The techniques and technologies available for clearance of renal stones in children have dramatically changed in the past few decades.25–29 Thirty years ago stones were exclusively managed by open surgery, whereas in this study, 68% children were managed either by lithotripsy, percutaneous nephrolithotomy, or endoscopic approaches. The difficult stone may need a combined approach, and in 21% open surgery alone was performed. Changes in the medical management of stone disease have been more limited.
The results of this study indicate a change in the aetiology of renal stones in children in the UK in the past 30 years. Children with renal stones do not necessarily present with the classic symptoms of pain and haematuria. They are more likely to have an underlying metabolic abnormality, and can now be treated with minimally invasive surgical techniques. We recommend that every child with a stone should have a metabolic evaluation, primarily to initiate preventive treatment early, but also to allow siblings to be screened if necessary.
REFERENCES
Linked Articles
- CORRECTION