Article Text

Abstract
Objective To assess the prevalence of symptoms of acute stress reactions (ASR) and post-traumatic stress disorder (PTSD) in paediatric trainees following their involvement in child death.
Design A survey designed to identify trainees’ previous experiences of child death combined with questions to identify features of PTSD. Quantitative interpretation was used alongside a χ2 test. A p value of <0.05 was considered significant.
Setting 604 surveys were distributed across 13 UK health education deaneries.
Participants 303/604 (50%) of trainees completed the surveys.
Results 251/280 (90%) of trainees had been involved with the death of a child, although 190/284 (67%) had no training in child death. 118/248 (48%) of trainees were given a formal debrief session following their most recent experience. 203/251 (81%) of trainees reported one or more symptoms or behaviours that could contribute to a diagnosis of ASR/PTSD. 23/251 (9%) of trainees met the complete criteria for ASR and 13/251 (5%) for PTSD. Attending a formal debrief and reporting feelings of guilt were associated with an increase in diagnostic criteria for ASR/PTSD (p=0.036 and p<0.001, respectively).
Conclusions Paediatric trainees are at risk of developing ASR and PTSD following the death of a child. The feeling of guilt should be identified and acknowledged to allow prompt signposting to further support, including psychological assessment or intervention if required. Clear recommendations need to be made about the safety of debriefing sessions as, in keeping with existing evidence, our data suggest that debrief after the death of a child may be associated with the development of symptoms suggestive of ASR/PTSD.
- psychology
- death
- palliative care
- occupational health
- intensive care
Statistics from Altmetric.com
What is already known on this topic?
Paediatric doctors in training are exposed to child death.
Post-traumatic stress disorder (PTSD) develops after exposure to trauma (such as child death).
PTSD can be effectively treated if recognised.
What this study adds?
Royal College of Paediatrics and Child Health trainees experience symptoms of acute stress reactions (ASR) and PTSD following exposure to child death.
Feelings of guilt following the death of a child may be associated with symptoms of ASR/PTSD.
Attending a debrief following child death may be associated with symptoms of ASR/PTSD.
Introduction
Each year in the UK approximately 6000 children die, with the majority of these deaths occurring in the hospital setting.1 2 There are little data to describe the emotional or psychological impact of a child’s death on a paediatric doctor in training. A small study has previously shown that 90% of registrars continue to reflect on their experience about a child death following the event; however, evaluation of the trainees’ mental health status was not included in this study.3
Paediatric trainees are likely to be exposed to child death at some point in their training. The Royal College of Paediatrics and Child Health (RCPCH) curriculum for paediatric trainees includes several competencies focusing on knowledge of practical guidelines, procedures and law relating to the death of a child.4 Training differs widely within the country, and although most regions offer training related to the RCPCH competencies there appears to be a lack of emphasis on resilience training, debriefing skills and strategies to ensure the welfare of those trainees exposed to child death.
There is no clear national guidance or framework for best practice with regard to debrief following the death of a child. Current practice appears to be ad hoc and unregulated. Existing evidence has raised concern that debrief may do more harm than good.5 This seems to be particularly true if debriefing is delivered by people without adequate training.6 Subsequent Cochrane reviews have concluded that there is no evidence that debriefing following a traumatic event is useful, and that in fact it may have adverse psychological outcomes in some individuals.7 8
Post-traumatic stress disorder (PTSD) is known to develop after exposure to an extremely traumatic or catastrophic event and is characterised by symptoms including re-experiencing of the event, avoidance of reminders of the event, hyperarousal and emotional numbing.9 10 If recognised PTSD can be adequately treated.11 Acute stress reaction (ASR) is the diagnosis given to the same collection of symptoms persisting for less than a month and may therefore precede a diagnosis of PTSD.9 There is currently no evidence to show how prevalent ASR and PTSD are in paediatric trainees following the death of a child.
The primary objective of this study was to assess the point prevalence of psychological symptoms that could form a potential diagnosis of ASR or PTSD in paediatric trainees following their involvement in the death of a child. Additional data were collected to identify groups of trainees who were more at risk of developing ASR or PTSD symptomatology.
Methods
Ethics
Ethical approval for this study was granted by the Hull York Medical School Ethics Committee.
Participants
Paediatric school administrators for all health education deaneries within the UK were contacted via email and asked to send the study information and an electronic survey link to paediatric trainees in their region who currently held an RCPCH National Training Number. Contact details for the lead investigator were provided for questions or concerns. Consent was implied by completion of the survey. Four weeks later the RCPCH paediatric school board trainee representatives were asked to send the same information to act as a reminder.
Survey design
The survey design and administration was via Qualtrics software (Qualtrics 2016). Data collected included trainee demographics, previous experience, exposure to child death, experience of debrief and child death training, and a series of psychological questions regarding the nature and duration of symptoms experienced following the death of a child. These questions were designed to identify trainees meeting potential diagnostic criteria that suggested an ASR (a constellation of symptoms lasting less than 1 month) or PTSD (the same symptoms but lasting more than 1 month) as per ICD-10 (International Classification of Diseases 10th Revision) and DSM-V (Diagnostic & Statistical Manual of Mental Disorders 5th Edition).9 10
Data analysis
Following data collection researchers performed descriptive statistical analysis to organise and sort the data set. For all categorical data a Χ2 test was used. Bonferroni correction was used for pairwise correction should significance occur between multiple groups. For all tests, a p value of <0.05 was considered significant. Analysis took place using IBM SPSS Statistics V.23 (2015).
Results
Survey demographics
Six hundred and four surveys were distributed. Three hundred and three surveys were completed (response rate 50%). Response rates varied for each question.
Women accounted for 231/283 (82%) of respondents. Men were slightly under-represented with 52/283 (18%) compared with the 2012 RCPCH workforce data, which suggested that 31% of UK paediatric trainees are men and 69% are women.12 Distribution across training grade was evenly spread, with the exception of ST8 trainees who were under-represented. Further trainee demographics are summarised in table 1.
Respondent demographics
Training
Table 2 summarises the respondents’ training experiences.
Respondent training and previous experience
Experience of child death
Two hundred and fifty-one (90%) of 280 trainees reported that they had been involved with the death of a child during their training. Seventy-one (29%) of 249 had been the team leader during a resuscitation in which the child had died. Many trainees had experienced more than one death (figure 1).

Number of child deaths experienced by individual trainees.
Trainees experienced child death in a variety of locations: 193/250 (77%) in an emergency department, 82/250 (33%) on a paediatric ward, 155/250 (62%) on a paediatric intensive care unit, 10/250 (4%) out of hospital, 11/250 (5%) in a hospice and 7/250 (3%) on an adult intensive care unit.
The majority of these deaths were unexpected (217/250, 87%). The remainder were either expected palliative care deaths (160/250, 64%) or deaths following redirection of life-sustaining treatment (174/250, 70%).
Experience of debrief
The trainees were specifically asked about their most recent experience of the death of a child. A debrief took place after 118/248 (48%) of these deaths, and 25/117 (21%) of respondents could not attend the organised debrief. Reasons for non-attendance included priority of clinical commitments (14/25, 56%), lack of invitation (4/25, 16%), annual or study leave (4/25, 16%), being on a night shift (3/25, 12%), and 4/25 (16%) of people were unable to attend due to other commitments. No one selected the option ‘did not want to attend’.
Of these debriefs 95/115 (83%) were led by a consultant, 7/115 (6%) by a trainee, 4/115 (4%) by nursing staff, 4/115 (4%) by the psychologist and 2/115 (2%) by the hospital chaplain. Nineteen (7.7%) of 248 trainees had received training on how to facilitate a debrief.
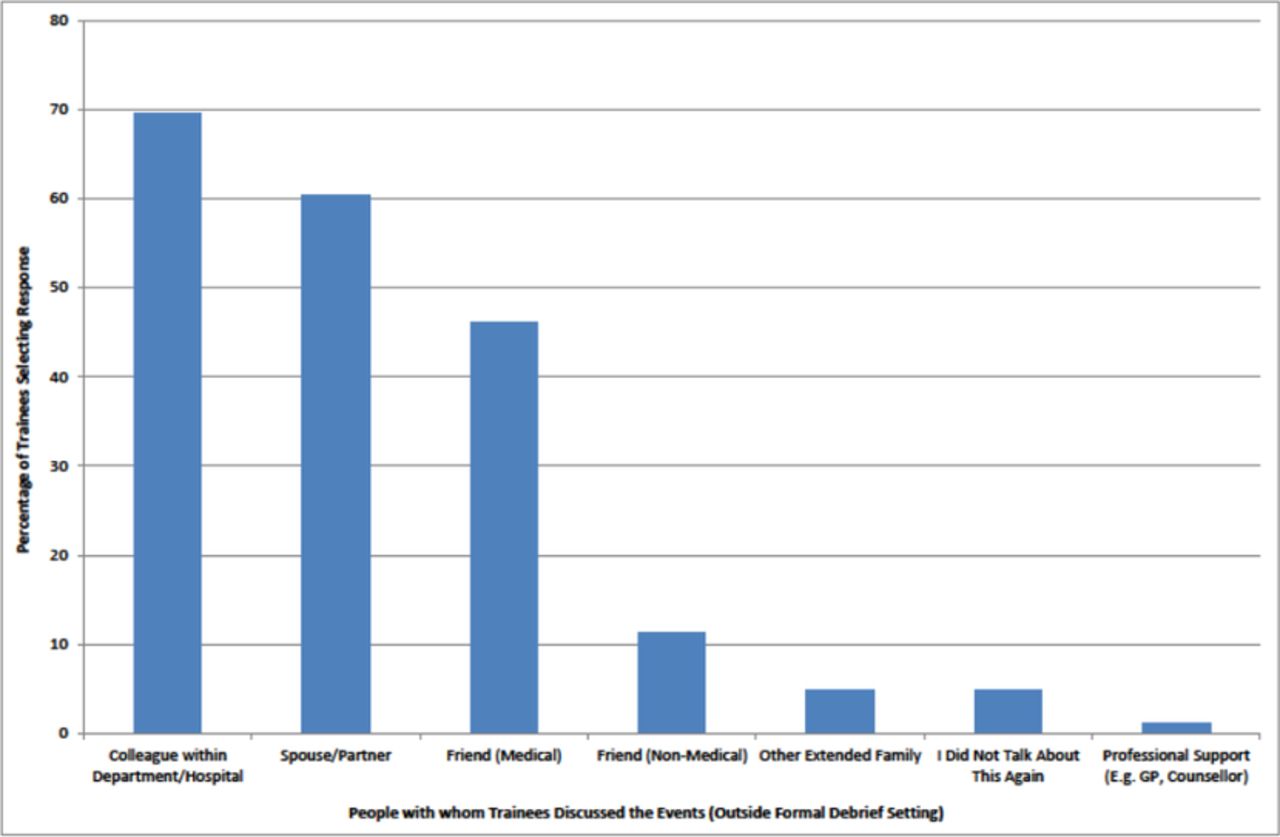
In addition to the formal debrief, trainees were asked to identify alternative avenues of communication following the event. Figure 2 describes the alternatives identified.
{kind=link}
{kind=link}
Alternative sources of discussion outside the formal debrief setting. GP, general practitioner.
Support following the death of a child
Two hundred and five (83%) of 248 trainees felt well supported by their seniors following child death, yet 43/248 (17%) felt unsupported. One hundred and fifty-eight (68%) of 233 trainees felt ready to return to work following the death of a child. However 75/233 (32%) felt that they were definitely or possibly expected to return to work before they felt ready.
Self-reported confidence
Trainees were asked to consider the statement ‘I feel prepared to deal with the death of a child…’, and 120/279 (43%) strongly or somewhat agreed, 60/279 (22%) neither agreed nor disagreed, and 99/279 (36%) disagreed or strongly disagreed.
Psychological impact
It was common for trainees to report ASR/PTSD symptoms or behaviours following the death of a child. Two hundred and three (81%) of 251 trainees who have been involved in a child death reported one or more of the individual symptoms or behaviours (taken from ICD-10 classification and DSM-V) that are collectively required for a potential diagnosis of ASR/PTSD9 10 (table 3).
Symptoms/behaviours reported by trainees after child death (total respondents=251)
In 21/203 (10%) of trainees the reported symptom(s) persisted for more than 1 month after the experience involving the death of a child. Furthermore 5/232 (2%) of trainees took time off work following their experience with the death of a child.
PTSD and ASR
Two hundred and three (81%) of 251 trainees with experience of child death displayed some diagnostic features of ASR/PTSD. Of these, 23/251 (9%) had symptoms that would allow them to meet the full criteria for a potential diagnosis with ASR and an additional 13/251 (5%) to meet the criteria for diagnosis of PTSD due to the duration of symptoms being over 1 month.9 10 In other words, 14% of the trainees in this cohort could potentially meet a psychiatric diagnosis.
Associations with development of ASR and PTSD symptomatology
Following the death of a child, 115/234 (49%) trainees reported specific feelings of guilt. Twenty-eight (24%) of 115 trainees who felt guilty displayed symptoms that could suggest ASR/PTSD (χ2, χ(1)=15.216, p<0.001). Therefore, trainees who demonstrated feelings of guilt after the death of a child displayed a significant increase in ASR/PTSD criteria compared with those who do not feel guilty.
Eighteen (20%) of 92 trainees who attended a formal debrief displayed symptomatology that suggests a potential diagnosis of ASR/PTSD. Conversely, 16/155 (10%) of those who did not attend a debrief met the ASR/PTSD criteria (Χ2, p=0.036).
Table 4 summarises associations between trainee characteristics and symptom patterns that may suggest a diagnosis of ASR/PTSD.
Associations with development of ASR and PTSD symptomatology
Discussion
Principal findings
This is the first study exclusively exploring the psychological impact of child death in paediatric trainees. Following their involvement with the death of a child, we found a 9% (23/251) point prevalence of potential ASR and a 5% (13/251) point prevalence of potential PTSD in our cohort of RCPCH paediatric trainees. There was no statistically significant association between developing symptoms suggesting ASR/PTSD and seniority, gender, age, working pattern, paediatric intensive care unit (PICU) experience, child death training or participation in exercise. However, our results do show that the development of symptoms of ASR/PTSD may be associated with feelings of guilt after the death of a child and with attendance at a debrief.
Although previous studies suggest a lifetime prevalence rate of PTSD in adults of 8%,11 13 our respondents were relatively early on in their paediatric careers, raising the likelihood of a higher lifetime prevalence rate than the 5% point prevalence demonstrated in our survey.
Kessler et al 13 report that the majority of people will experience ‘at least one traumatic experience in their lifetime’. The National Institute for Health and Care Excellence (NICE) guidance on PTSD suggests that following a traumatic experience 25%–30% of people may develop PTSD.11 Previous studies have confirmed the increased risk of PTSD presented by trauma surgery and emergency first response in the ambulance service.14 15 In one study, ambulance workers cited dealing with ‘cot death’ or ‘incidents involving children’ as their highest potential stressors.15 Two hundred and fifty-one (90%) of our 280 sample of paediatric trainees had been involved with the death of a child, and 44/249 (18%) had been involved with over 10 deaths, identifying paediatric trainees (and subsequently consultants) as a high risk group for exposure to recurrent trauma. Although the cumulative effect of trauma is unknown, it seems likely to represent a further risk factor for the development of PTSD during a career in paediatrics.
Training
The results of this survey suggest that training in child death has no association with the development of symptoms of ASR/PTSD. It is concerning that many trainees felt they had not been adequately prepared for child death. It is however difficult to know whether the problems lie solely in inadequate provision of child death training or whether the current teaching programmes are simply not addressing the needs of the trainees. Our findings may reflect a lack of focus on the emotional and psychological impact of child death during training sessions, with more weight being placed on the clinical aspects of dealing with child death. More research is necessary to establish the most effective methods of preparing trainees for the potential psychological sequelae of involvement in the death of a child. Resilience training has been evaluated in other sectors, and there is evidence that it has beneficial outcomes in mental health and subject well-being analysis.16 The role of resilience training has not been explored in doctors who are at risk of developing PTSD, and it seems that this area could be a focus for further research and review. We feel that current education in child death is inadequate and that a greater emphasis needs be placed on training staff to recognise the importance of identifying and supporting colleagues experiencing difficulties following the death of a child.
Debrief
Paediatric trainees responding to this survey showed a significantly increased prevalence of symptoms suggesting PTSD if they had attended a debrief compared with those who had not. This suggests a potential association between attendance at a debrief following exposure to a child death and psychological harm. In support of this finding, both NICE and the Department of Health recommend that one-off debrief sessions after traumatic events should be avoided.10 These recommendations are based on several Cochrane reviews that conclude that single and multiple session debriefing, following a traumatic event, can have adverse outcomes in select individuals.7 8
The seemingly random and unmonitored nature of debriefing following the death of a child is a concern particularly in the context of its causing potential harm to attendees. The vast majority of trainees surveyed in our study had no training on how to lead a debrief, and yet as consultant they would be potentially facilitating these sensitive and highly emotional sessions. There is currently a lack of standardisation with regard to timing and leadership of debriefing following child death in the UK. This needs to be addressed with careful attention paid to the growing body of evidence that suggests debriefing following traumatic events may not be the right way to reduce psychological harm.
Study limitations
We acknowledge that there may have been selection bias in this survey with trainees who chose to complete the survey potentially holding stronger opinions or having more relevant experience of child death than those choosing not to complete it.
We elected to ask questions of trainees addressing all symptoms that feature in the diagnostic criteria for ASR/PTSD (identified in the ICD-109 and DSM-V10). This enabled an assessment of point prevalence of individual symptomatology. The validated PTSD questionnaires that are available are screening tools and would not allow us to gain a full insight into the distribution of all psychological symptoms experienced. It is important to therefore recognise this is a point prevalence assessment using a non-validated tool. We appreciate that our survey could not ‘diagnose’ ASR/PTSD, which would require a full, clinician-led assessment.
Conclusion
Paediatric trainees should be recognised as a vulnerable group at high risk of developing ASR and PTSD. Assessment of psychological impact of child death on paediatric trainees should be a priority both at a local and national level. The feeling of guilt should be identified and acknowledged to allow prompt signposting to further support, including psychological assessment or intervention if required. Clear recommendations need to be made about the safety of debriefing sessions after the death of a child as, in keeping with existing evidence, our data suggest that debrief after the death of a child may be associated with the development of symptoms suggestive of ASR/PTSD.
Acknowledgments
We would like to thank all the trainees who took the time to complete this survey and give honest answers, and to thank the deaneries that supported the project and distributed the survey to their trainees. We would like to thank Dr John Pappachan (Associate Professor of Paediatric Intensive Care Medicine) for his critical review of this document.
Footnotes
Twitter Michael J Griksaitis @MJGriksaitis
Contributors CEH and CW were involved in survey design, data analysis and production of the first draft of the paper. JH was involved in survey design and contributed to the psychological aspects of the project. GMF was involved in study design, ethics application and contributed to educational aspects of the paper. MJG was involved with project design, data analysis, survey design/distribution and supervised production of the manuscript. All authors read, contributed and approved the final manuscript.
Competing interests None declared.
Ethics approval Hull York Medical School Ethics Board.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement All data are included in the paper.