Article Text

Statistics from Altmetric.com
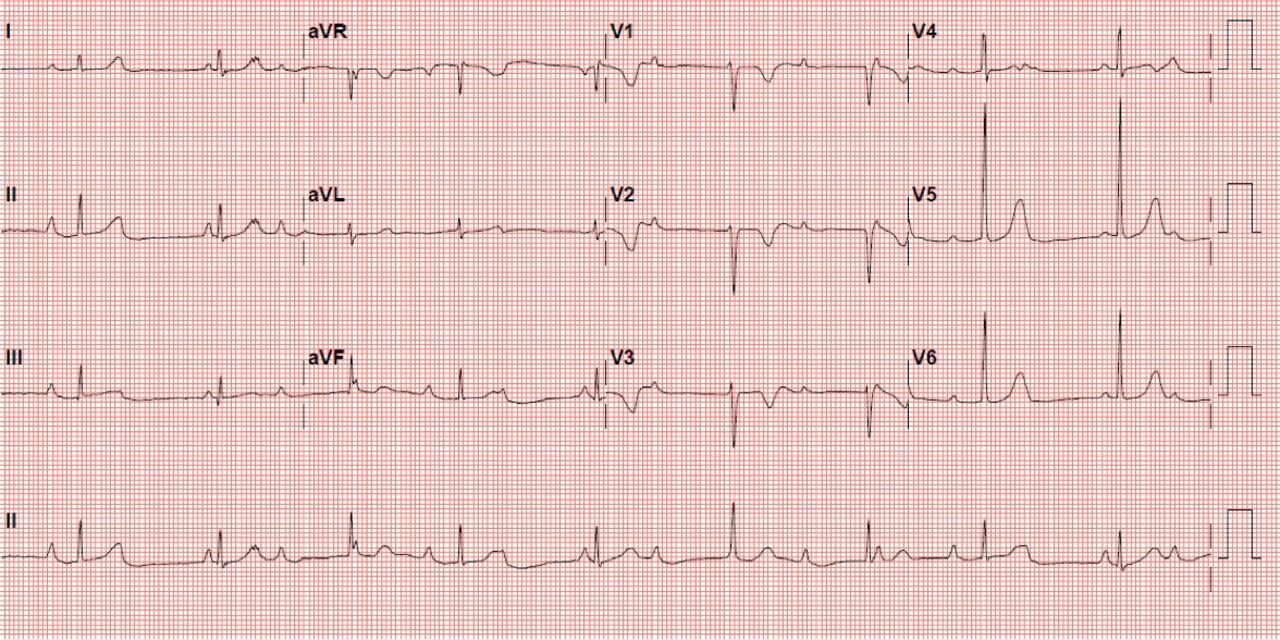
A fit, well, asymptomatic 6-year-old girl was referred to clinic for a murmur. Her ECG is shown in figure 1.

{kind=link}
Patient’s ECG.
Using the ECG checklist, which categories highlight possible concerns?
Rate, rhythm and PR interval
The median heart rate for a 6-year-old girl is 89 bpm (range 68–115 bpm (2nd–98th centile)).1 Here, the ventricular rate is 5–6 large squares (50-60 bpm), signifying bradycardia. The atrial rate is faster (three large squares, 100 bpm). Some P waves are obscured within T waves or QRS complexes. The P waves are not related in the normal way to the QRS complexes. Therefore, the PR interval cannot be calculated.
What does the ECG show?
Complete heart block (CHB)
The atrial and ventricular rates are different, with a complete lack of relationship (dissociation) between atrial and ventricular depolarisation. In this case, the escape rhythm originates from the His Bundle resulting in narrow QRS complexes. More often, the escape rhythm originates in the ventricle, resulting in broad QRS complexes due to depolarisation via the ventricular myocardium.
What conditions are commonly associated with this abnormality?
Maternal autoimmune disease, eg, lupus, congenitally corrected transposition of the great arteries (ccTGA), double inlet left ventricle (DILV), left atrial isomerism (LAI)
Congenital CHB is associated with structural and non-structural heart disease. In the presence of a structurally normal heart, CHB is seen most commonly in children born to mothers with autoimmune conditions, such as systemic lupus erythematosus or Sjogren’s syndrome, with positive serology for anti-Ro and/or anti-La antibodies. However, congenital CHB occurs in only 2% of fetuses where there is maternal positive serology. The risk of recurrence in future pregnancies rises to 20%.2
There are three principal, but rare, structural congenital heart lesions that are associated with CHB. These are congenitally corrected transposition of the great arteries (ccTGA), double inlet left ventricle (DILV) and left atrial isomerism (LAI). ccTGA is an uncommon condition in which the atriums, ventricles and great vessels are discordantly arranged, but the circulation is physiologically ‘correct’. ccTGA is often associated with other structural heart lesions (VSD, pulmonary stenosis, ebsteinoid tricuspid valve), but in the absence of these, may be entirely asymptomatic. The conduction system is not infrequently abnormal. CHB may be the first presentation of this condition.
DILV occurs where the dominant ventricle is of left ventricular morphology, with only a rudimentary right ventricle. Conceptually, it can be thought of as part of the spectrum of ccTGA and so the conduction anomalies that apply in ccTGA also apply in DILV.
LAI is a laterality defect in which there are two left atria, one in the position of the right atrium. There is often therefore a congenital absence of the sino-atrial node, which, by definition, is associated with conduction abnormalities. LAI is also commonly associated with significant structural heart disease including unbalanced atrioventricular (AV) septal defect.2
What are your management options for this abnormality?
Placement of a permanent pacemaker
The definitive management is the implantation of a permanent pacemaker. The timing of this will depend on the history and symptoms. Class 1 indications3 for permanent pacemaker insertion include:
Advanced second or third degree AV block with symptomatic bradycardia, ventricular dysfunction or low cardiac output state.
Sinus node dysfunction with symptomatic bradycardia.
Postoperative advanced second or third degree AV block that is not expected to resolve or persists for at least 7 days after surgery.
Congenital third degree AV block with wide complex escape rhythm, complex ventricular ectopy or dysfunction.
Congenital third degree AV block in an infant with a ventricular rate of <55 bpm (or 70 bpm in presence of structural congenital heart disease).
This patient is clinically asymptomatic (no syncopal or presyncopal episodes, normal exercise tolerance). Repeat ambulatory monitoring showed no evidence of significant pauses. There is a small but increasing risk of sudden death in such patients, and so transvenous pacemaker implantation is usually undertaken electively in the early teens, even in the absence of symptoms.
Ethics statements
Patient consent for publication
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.