Article Text

Abstract
Tic disorders including Tourette syndrome (TS) are neuropsychiatric disorders that are common referrals to paediatricians, paediatric neurologists and child psychiatrists. Although differentiating tics and TS from other movement disorders is not difficult, it is essential to detect comorbid conditions and their contribution to TS.
- Neurodevelopment
- Child Psychiatry
- Child Psychology
- Paediatric Practice
Statistics from Altmetric.com
Case scenario
Eight-year-old Tom was referred by his general practitioner (GP) asking whether his movements and behaviour were tics. His parents reported noticing intermittent facial grimacing movements and grunting for the last six months. They report that it happens both at home and in school and was worse a few weeks back when they had consulted the GP. The GP advised that the episodes should be ignored, and since then they have been less frequent.
What are tics?
Tics are sudden recurrent individually recognisable vocalisations, intermittent movements or movement fragments that are almost always briefly suppressible and are usually associated with awareness of an urge to perform the movement.1 Suppression of a tic usually leads to growing discomfort, which is alleviated by performing the tic. Characteristic features of tics are predictability of movement, predictability of onset and triggered by suggestion, sensory cues, stress, excitement or demonstration.1 ,2 Tourette syndrome (TS) is in the spectrum of tic disorders but needs to fulfil certain diagnostic criteria (see below).
Types of tics
Tics can be classified by description (table 1) and by pathophysiology (box 1). Pathologic tics can be further classified into primary sporadic, primary inherited and secondary.
Classification of tics by description
Classification of tics by pathophysiology
Physiologic tics
Motor mannerisms3
Repetitive, distinctive behavioural trait that does not interfere with life or cause self-injury (eg, brushing coat repetitively, persistent hair twirling)
Pathologic tics
Primary
Sporadic
Provisional/transient tic disorder (<1 year)
Chronic/persistent motor or vocal tic disorder (>1 year)
Adult-onset (recurrent) tics
Tourette syndrome
Inherited
Tourette syndrome
Huntington's disease
Primary dystonia
Neuroacanthocytosis
Secondary (‘Tourettism’)
Infections: encephalitis, Creutzfeldt–Jakob disease, post-streptococcal disorders
Drugs: stimulants, levodopa, carbamazepine, phenytoin, phenobarbital, antipsychotics (tardive tics)
Toxins: carbon monoxide
Developmental: pervasive developmental disorders
Brain injury: head trauma, stroke
Genetic: neurocutaneous syndromes, chromosomal abnormalities, neuroacanthocytosis
Psychiatry: schizophrenia, psychogenic tics
Diagnostic criteria and spectrum of tic disorders including TS
Tic disorders can be diagnosed using the Diagnostic and Statistical Manual of Mental Disorders V (DSM-V)4 or the International Classification of Disease (ICD)-105 criteria and be classified as:
provisional tic disorder (DSM-V) or transient tic disorder (ICD-10)—tics that occur on most days with a duration of 4 weeks to a year, not due to TS;
chronic/persistent motor or vocal tic disorder—tics that occur on most days for longer than a year, not due to TS;
TS—two or more motor tics and at least one vocal tic occurring for at least a year.
All the above must start before 18 years of age and not be due to physical conditions or medication side effect. There should not be a tic-free period of >3 months in a year.
Prevalence and natural history
Tics are present in up to 5% of the population, with a lifetime prevalence of ≥20% among boys.6 The prevalence of TS is 7.7 per 1000 children (95% CI 3.9 to 1.51).7 Motor tics usually begin between the ages of 3 and 8, and phonic/vocal tics usually follow the onset of motor tics after several years.8 Uncomplicated tics peak in the early second decade with a marked reduction in tic severity by the age of 19 or 20 years (figure 1).9

Relationship between age and severity of tics and coexisting disorders.
The onset of TS is typically between 2 and 15 years, average of 6.4 years, and is manifested in 96% of patients by 11 years of age.10 The disorder is usually diagnosed 2–3 years after onset of tics. Peak severity of tics are usually at 9–11 years of age. Five to ten per cent of patients have an intensifying course without improvement. In about 85% of patients, however, symptoms diminish during or after adolescence11 (figure 2).

The clinical course of Tourette syndrome.
Tics in TS affects more males than females (4.3:1).12 They are characteristically waxing and waning.2 Frequency and severity of tics in childhood is hardly predictive of tic severity in adulthood. Tics and TS are associated with other neurobehavioural conditions, particularly attention-deficit hyperactivity disorder (ADHD) and obsessive-compulsive disorder (OCD) (figure 1).
Pathophysiology
The disorder likely results from a disturbance in the striatal–thalamic–cortical (mesolimbic) spinal system, in which dopamine plays an important role, which leads to disinhibition of the motor and limbic system.13 Alterations in the cortico–striato–thalamo–cortical circuits in patients with TS have been found on MRI and electrophysiological studies.14 Family studies strongly indicate a genetic component in TS, with shared genetic influences between tics and OCD. The link to ADHD, however, is unclear.14 Several loci have been identified as candidate susceptibility regions, and mutations in SLITRK1 gene15 and HDC gene16 appear to be a rare cause of TS.
Differential diagnoses
Other hyperkinetic movement disorders (dystonia, choreoathetois, myoclonus, tremor, stereotypy)
Dystonia is usually triggered by and interferes with voluntary movement, but tics are usually suppressed by and do not interfere with voluntary movement.1 Tics can be differentiated from athetosis, chorea and myoclonus by the lack of continuity of the movement, the intervening periods of normal movement and the lack of interference with ongoing tasks. Tics are predictable and repeatable compared with chorea and myoclonus. The clear initiation and termination of each individual tic movement and the lack of rhythmicity in timing of initiation of movement distinguishes it from tremor and stereotypies.1 Unlike tics, stereotypies usually start before the age of 2 years. Stereotypies are repetitive simple movements, vocalisation or behaviour such as head banging, waving or flapping that are present for >4 weeks and lack premonitory urge.3 Table 2 outlines the key features of various movement disorders.
Key features of hyperkinetic movement disorders
Obsessive-compulsive disorder
It can be difficult differentiating a tic from obsessive-compulsive behaviour (table 3) as they share many similarities and are indeed often comorbid. Both decrease with concentration, increase with emotional excitement and are suppressible (tics for a shorter term than OCD).14
Clinical differences of tic disorders and obsessive-compulsive disorders
Other conditions that mimic tics
Tics can also be mistaken for other conditions such as epileptic seizures, sleep disorders, attention problems and functional disorders (table 4).
Clinical conditions that could be mistaken for tics and vice versa
Comorbidities
TS is commonly associated with comorbidities (table 5).12 Motor and vocal manifestations are more frequent in boys, whereas girls are more likely to have behavioural problems such as OCD.
Comorbid conditions in patients with Tourette syndrome
ADHD symptoms in TS occur in the majority of cases before tic onset (figure 1). In our personal experience, we found that comorbid ADHD, when present, occurred in nearly 70% of affected children before the onset of TS. ADHD symptoms tend to decrease in 20% of children during adolescence, usually following a decrease in tics. ADHD in patients with TS are associated with increased irritability and rage attacks, increased vulnerability for drug abuse, depression and antisocial behaviour. TS plus ADHD appears to be a more severe condition than ADHD alone.17
Comorbidity of TS with OCD can make distinction between complex motor tics and compulsions difficult.1 Comorbid obsessive-compulsive symptoms start at a later age (around 10 years) than tics (figure 1). Normal obsessive-compulsive-like symptoms are present in many young children, peaking at 2.5 years of age. This disorder, when associated with tics, generally has a pre-pubertal age of onset. OCD can lead to periods of depression. In our personal experience, we found OCD occurred in 50% of children with TS. Comorbid OCD and ADHD are associated with poorer psychosocial functioning.14
Assessment
Salient features of clinical assessment and investigations are outlined in table 6. Obtaining a video recording of the episode on a camera or a mobile phone is most useful in making the correct diagnosis.
Assessment of tics
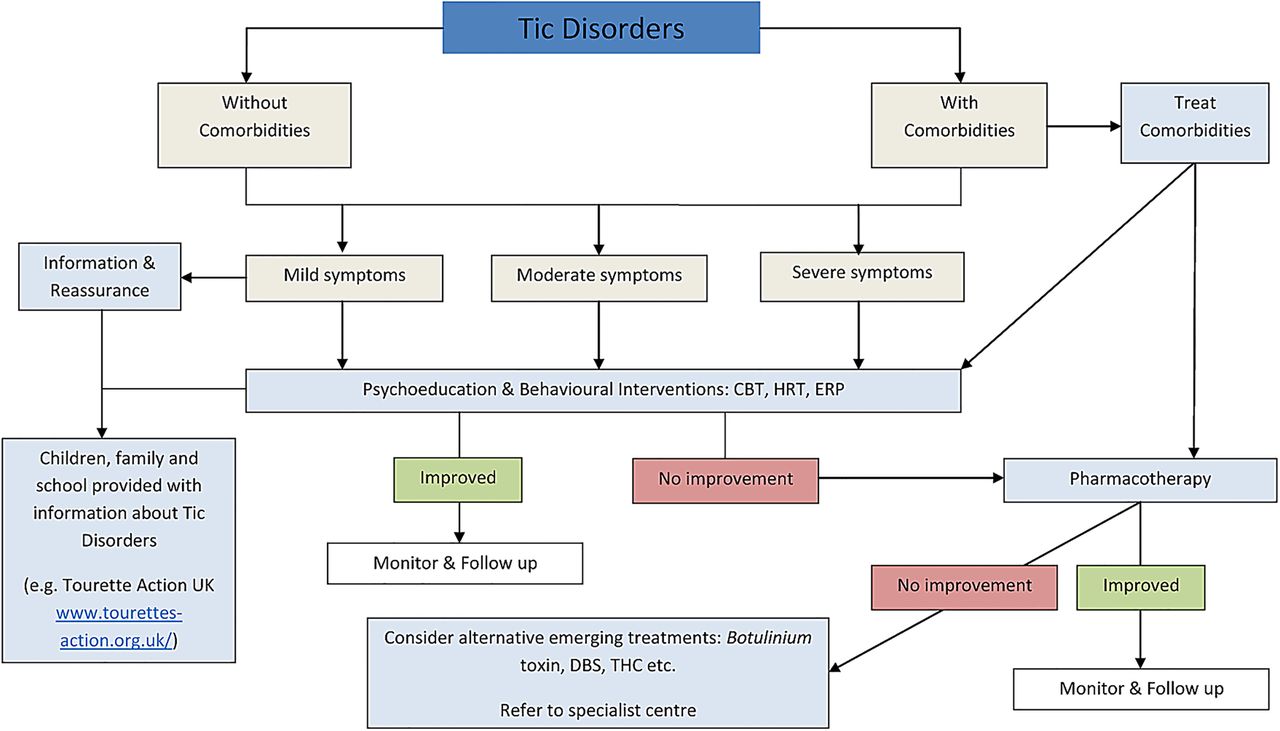
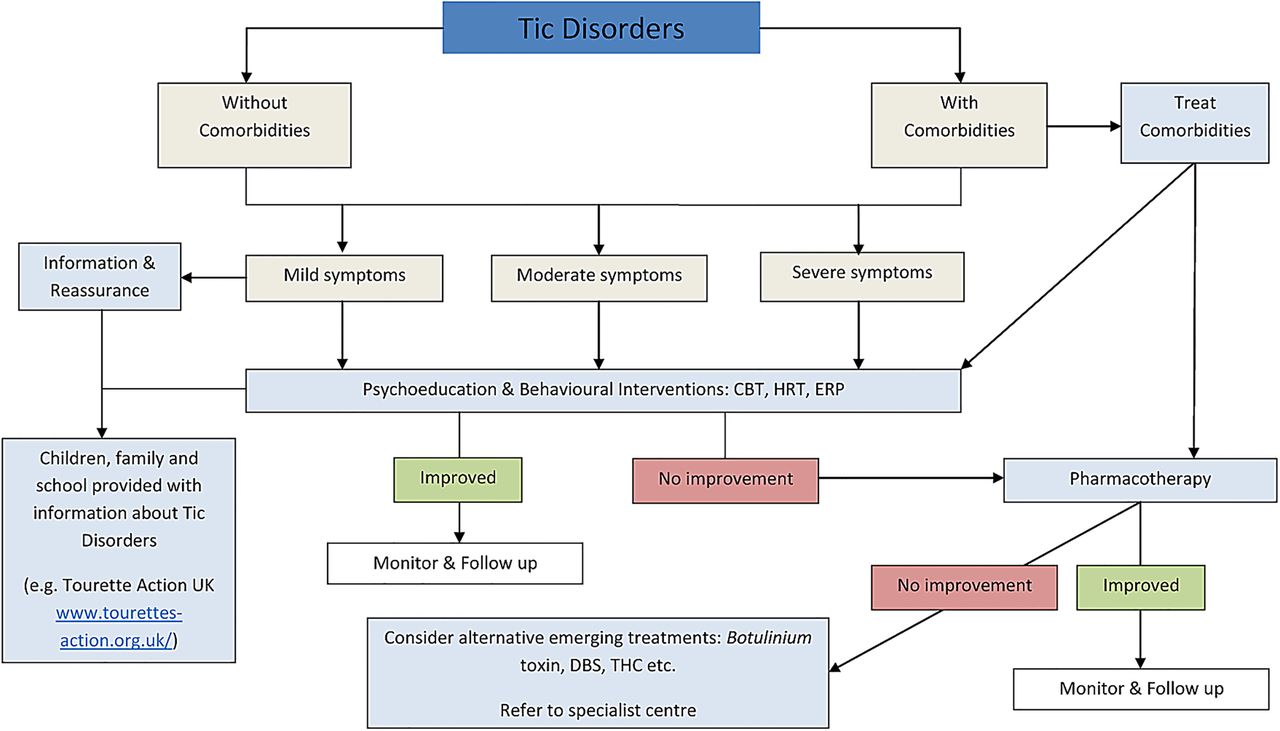
Management (see algorithm) (figure 3)
Most children with simple motor tics do not require treatment. Knowledge of the temporal patterning of tics is fundamental for clinicians as it informs decisions about when to initiate or change management and when to ‘watch and wait’ after psycho-education and reassurance.2
Non-pharmacological and/or pharmacological interventions should be considered in addition to psycho-education for children with clear impairment associated with the tics19 (box 2).
Indication for treatment of tics
Tics cause subjective discomfort (eg, pain and/or injury)
Tics cause sustained social problems for the patient (eg, social isolation or bullying)
Tics cause social and emotional problems for the patient (eg, reactive depressive symptoms)
Tics cause functional interference (eg, impairment of academic progress)
In the presence of comorbid conditions (ADHD, OCD, depression), it is better to treat the comorbidities first, as successful treatment of them will often diminish tic severity.9
Non-pharmacological
Behavioural interventions
Habit reversal training (HRT) and exposure with response prevention (ERP) have the most evidence among the behavioural treatments for tics20 and are considered first line. Treatments that are considered second line or ‘add-on’ are contingency management, function-based interventions and relaxation training. HRT offers a set of techniques to increase patients’ awareness of occurrence of a tic, followed by a response training to inhibit the tic. In ERP, tics are viewed as conditioned responses to stimuli. By confronting the sensation, the stimuli evokes (exposure) and resisting the tic (response prevention) patients might learn to tolerate the sensation (habituation).
One of the oldest described behavioural treatment, massed (negative) practice or voluntary ‘over-ticcing’, involves repeated, rapid, voluntary performance of the tic for specified periods of time interspersed with brief periods of rest with an expectation that this may reduce tic frequency at other times. Current evidence suggests that this is of limited therapeutic value.20 There is also no evidence that ‘masking’ tics help. Masking may not provide the same satisfaction as performing the tic unmasked and potentially could increase tic frequency in some children.
Psychosocial interventions
Psychosocial interventions include psycho-education, group work, information and support from voluntary organisations. Psycho-education in TS aims to improve the tolerance for symptoms and to support stress reduction. Psycho-education involves providing information about the long-term and short-term variability of tics, about the natural course and about possible coexisting problems. Psycho-education alone may be used in families who do not engage with or need more comprehensive treatments due to very mild tics or cannot access treatments due to lack of services.20 Other psychosocial interventions are used as adjuncts to other therapies.
Pharmacotherapy
Pharmacotherapy should only be instituted by clinicians or units who have experience of managing tic disorders and of using the medication itself. These medications are not commonly used by most paediatricians and caution needs to be exercised as their use can be associated with significant side effects. In most instances where medication is being considered, it is preferable to refer the child to a specialist unit and an experienced clinician.
There is a paucity of studies directly comparing efficacy and safety of pharmacological agents, hence no firm recommendations can be made. Pharmacotherapy probably has the fastest onset of response compared with behavioural treatments, but this experience has never been tested in a clinical trial. In our personal practice, indications for pharmacological treatment are subjective discomfort, social isolation with bullying and harassment, reactive depressive symptoms and impairment of school performance. We use non-neuroleptics like clonidine as a first-line medication. We use neuroleptics as second line when non-pharmacological treatment and first-line treatment have been unsuccessful. As tics are thought to involve the dopaminergic pathway, modulating this, particularly by blocking the post-synaptic D2-receptors, is the main action of pharmacotherapy in tics.19 Medication choice, doses and level of evidence of effectiveness are provided in table 7.
Indications, efficacy and monitoring requirements of medications used for treatment of chronic tic disorders and TS
{kind=link}
{kind=link}
{kind=link}
Suggested management algorithm for children with tic disorders. CBT, cognitive-behaviour therapy; DBS, deep brain stimulation; ERP, exposure with response prevention; HRT, habit reversal training; THC, tetrahydrocannabinol.
Alternative and emerging therapies
It is recommended that in severe cases of TS not responding to conventional therapies other agents could be tried in specialised centres19 (see algorithm). This includes the use of tetrahydrocannabinol, botulinum toxin injection, deep brain stimulation and transcranial magnetic stimulation.
Schools and tics
Providing educators with general information relating to the aetiology, presentation and course of TS will help them to implement effective individualised strategies to manage classroom behaviour, thus maximising child’s learning potential.20 There is good resource on Tourette Action UK website for educators (http://www.tourettes-action.org.uk/?&filter=teachers).
Conclusion
Tic disorders are common and are increasingly referred to paediatricians from primary care physicians, therapists and from local education authorities. A better understanding and support is needed for children and families. If these children are adequately managed with support from colleagues in psychology and educational authorities, they can achieve their maximum potential.
Test your knowledge
Jake (8 years old), a fit and well boy has had grunting and eye-blinking tics for the last nine months for most days without a tic-free period of >2 weeks. What is his current diagnosis?
Provisional/transient tic disorder
Chronic motor tic disorder
Chronic motor and vocal tic disorder
Tourette syndrome
Which two comorbid conditions are most common with Tourette syndrome?
Conduct disorder and ADHD
Depression and OCD
ADHD and OCD
ADHD and specific learning difficulties
What should the initial management be of a 9-year-old girl with mild obsessive compulsive behaviour, shoulder shrugging and simple phonic tics for more than a year who is doing well at school and has good social support?
Psycho-education
Habit reversal therapy
Manage her obsessive compulsive behaviour
Atypical neuroleptics
Answers to the quiz are at the end of the references.
Answers
1. A
2. C
3. A
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement Data regarding personal experience are available from SRM.