Article Text

Statistics from Altmetric.com
Information about current guideline
‘Development of guidelines for skeletal survey in young children with fractures’ is an American guideline by Wood et al published in the journal Pediatrics in June 2014.1 The aim of this study was to devise guidelines on when to carry out an initial skeletal survey (SS) in children less than 24 months of age with fractures, based on available evidence and expert opinions from diverse paediatric specialties.
Previous guideline
There are no previous published guidelines on the exact indications to when an initial SS should be performed in children less than 24 months of age.
In 2008, the Royal College of Radiologists (RCR) and the Royal College of Paediatrics and Child Health (RCPCH) published guidance on standards in radiological investigations of suspected non-accidental injury (NAI).2 They recommend that ‘a full skeletal survey should always be performed’ as an initial imaging method in children under 2 years of age who are undergoing a clinical investigation for suspected physical abuse. This guidance is also cited in the RCPCH child protection companion published in 2013.3 In 2009, the American Academy of Pediatrics (AAP) also highlighted that a SS is ‘mandatory in all cases of suspected physical abuse’ in this age group4 and reiterated this in their updated 2014 publication that provides further guidance to health professionals when to consider NAI as the cause of fractures5 (box 1).
Resources
Link to paper ‘Development of guidelines for skeletal survey in young children with fractures’ http://pediatrics.aappublications.org/content/early/2014/06/10/peds.2013-3242.full.pdf+html
Link to 2008 RCH/RCPCH Standards for radiological investigations of suspected non-accidental injury. http://www.rcpch.ac.uk/sites/default/files/asset_library/Publications/S/StandardsforRadiologicalInvestigationsD.pdf
Link to 2009 paper by the AAP, ‘Diagnostic imaging of child abuse’ http://pediatrics.aappublications.org/content/123/5/1430.full.pdf+html
Link to 2014 paper by the AAP, ‘Evaluating children with fractures for child physical abuse’ http://pediatrics.aappublications.org/content/133/2/e477.full.pdf+html?sid=3417f97b-11a8-4b1e-8625-cfbb3b2e40ac
The RCR/RCPCH and AAP agree that a SS has a high yield of showing occult fractures in children less than 24 months but less so in older age groups where the need for a SS has to be considered on a case-by-case basis.
Controversial and key issues addressed
Fractures are a common presentation of injury in young children that may be both accidental and non-accidental in nature. Despite the valuable guidance offered by RCH/RCPCH and AAP (box 1), there are no clear recommendations on what is meant by ‘suspected cases’ of abuse, including which specific fracture scenarios should raise the clinician's suspicion to order a SS.
Failing to recognise such injuries can result in increased morbidity and mortality for the child. On the other hand, routinely performing SSs in children where occult injuries are unlikely can lead to unnecessary exposure to radiation that is unadvisable by the AAP.
Lack of clear guidance can lead to disparities in the quality of care to children with suspicious injuries. This often results in certain vulnerable groups being investigated more than others. In these guidelines, Wood et al aim to provide the clinician with specific criteria to when a SS is indicated in children less than 24 months of age in order to reduce such disparities in cases where NAI is not otherwise suspected.
Underlying evidence base/methodology
A modified Delphi process was used in this study. A literature review (1990–2011) was initially performed and 41 studies were used to identify clinical scenarios for which a SS was appropriate and necessary in cases of young children presenting with fractures. Some of the scenarios were specific to a particular fracture group (including femur, humerus, rib, tibia/fibula, skull and clavicle), whereas other scenarios described the mechanism of injury (eg, whether it was a result of domestic violence), any delay in presentation and other findings present on physical examination. A panel of 13 experts from key paediatric specialties including emergency medicine, radiology, orthopaedics and child abuse were recruited. They independently analysed the clinical scenarios that were identified from the literature review in three different rounds. Guidelines were synthesised from the results obtained from the study groups in the second and third rounds whereby results were categorised according to whether a SS was necessary, uncertain or unnecessary
What do I need to know?
What should I stop doing?
Requesting a routine SS, when there is no further suspicion of NAI, in
Ambulatory children (12–23 months) with
a distal spiral fracture of the tibia/fibula with a history of falling while walking/running;
a distal radial/ulna buckle fracture with a history of a fall onto the outstretched hand.
Cruising infants (9 months old or older) with a history of a fall presenting with a distal radial/ulna buckle fracture or toddler fracture of tibia/fibula.
In infants greater than 6 months who have a linear, unilateral skull fracture with a history of a significant fall (eg, a fall greater than 1 m or a fall with the caregiver landing on the child) (The RCPCH companion states that unilateral skull fractures in children less than 1 year of age have been equally reported in intentional and unintentional head injuries. The authors of this guidance are proposing against a routine SS in infants greater than 6 months when the mechanism of injury is likely to be accidental and no other suspicions of NAI are suspected).
Infants less than 22 days who have an acute clavicular fracture related to birth or infants greater than 30 days with a healing clavicular fracture.
What should I ensure I have started doing or doing differently?
Requesting a SS in
All children 0–11 months of age with any type of fracture with rare exceptions listed above and summarised in figure 1.
Children 0–23 months old with a history of
confessed abuse;
injury within the context of domestic violence;
impact from an object (eg, toy) causing a fracture;
not seeking care after 24 h in any child less than 11 months of age or in children 12–23 months of age when the fracture is associated with significant pain and/or physical findings;
additional injuries on examination unrelated to fracture (eg, burns and bruises);
no trauma/explanation for fracture.
Children 12–23 months, with the following fracture types:
rib fracture
classic metaphyseal fracture
complex/depressed skull fracture
humeral fracture with epiphyseal separation due to a short fall (<1 m)
femur diaphyseal fracture attributed to a fall from any height.
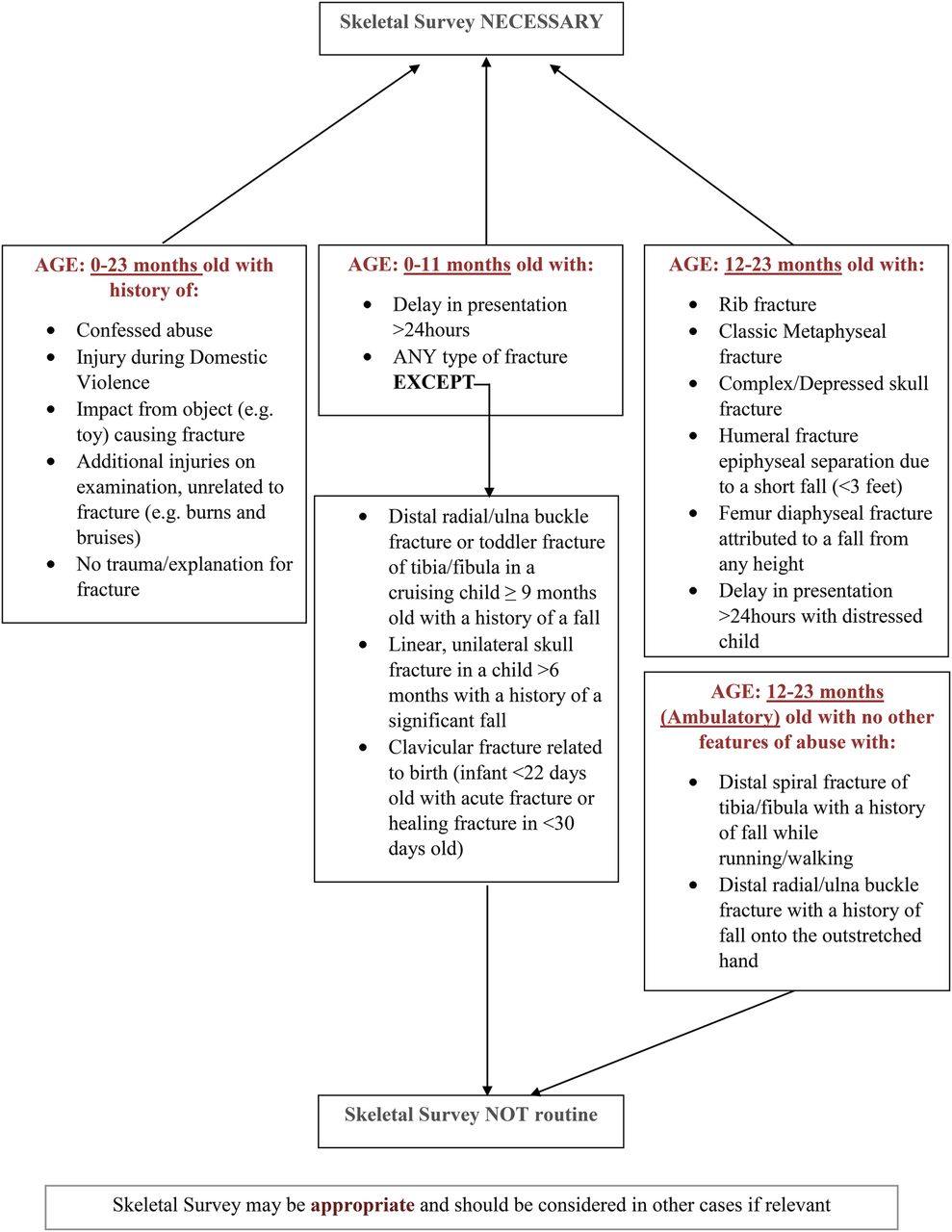
{kind=link}
Indication for skeletal survey when there is a fracture in a child less than 24 months of age.
What can I continue to do as before?
Requesting a SS in any other case that is deemed relevant according to clinical judgement.
Unresolved controversies/limitations
This guidance was based on the limited evidence presented in the literature on the use of SSs in children and the likelihood of abuse in children presenting with fractures in addition to the opinion of expert professionals. Thus, only post-implementation evaluation can highlight whether this guidance is deemed useful in standardising care, increasing detection of abuse and avoiding the use of routine SSs in low-risk situations. Further points relating to the holistic approach needed in safeguarding cases are discussed in box 2.
Authors' review
This guidance can be helpful in providing the clinician with concrete examples on when to perform a skeletal survey in children under 24 months of age. Time will tell whether clinicians will find such guidance useful in clinical practice. We felt the need to further highlight the importance of using such guidelines in conjunction with the holistic approach required when infants present with any fracture. It is important to include an in-depth history and general physical examination, while maintaining a high degree of clinical suspicion in a non-judgemental manner. This may be challenging, especially in the busy A&E department where many of these children present and where the relevant background information may not always be available. Health professionals must remember to ‘think the unthinkable’ in certain situations as recommended by the serious case review of Daniel Pelka.6 Updated training in safeguarding children with active participation will help health professionals gain the skills to better adopt such an approach. Decisions should be taken after consulting with senior colleagues and/or the safeguarding team. Grey cases, especially those that present out of hours, should be discussed within a multidisciplinary team where further information can be shared. This will help the team to decide the need for further investigations and/or review in a paediatric setting.
Clinical bottom line
A thorough evaluation must be performed in young children with fractures to help distinguish cases of accidental from non-accidental injury.
Skeletal survey (SS) is an important radiological tool in children less than 24 months of age to detect occult fractures related to abuse or fractures that are not suspected from the history and/or examination.
SS exposes children to radiation and should not be routinely performed in children at low risk of occult injuries.
Footnotes
Correction notice This paper has been amended since it was published Online First. We omitted the first author's second affliation. We would like to apologise for this oversight.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.