Article Text

Abstract
Embracing failure for the purpose of learning is a key trait in successful teams. Failure, however, is not the only source of learning. The majority of interventions in healthcare are successful, yet our prevailing efforts to extract learning intelligence tend to focus almost exclusively on failures, such as harm and errors. By considering the learning potential across the whole landscape of work from success to failure, we can widen the range of learning opportunities. The key steps to learn from excellence are first to recognise excellence, which can be highly subjective, and second to provide positive feedback. Positive feedback enhances learning through a number of routes, including increasing self-efficacy and intrinsic motivation. It may also help to improve relationships within teams and to offset negativity associated with blame cultures.
- psychology
- qualitative research
Statistics from Altmetric.com
The ability to recognise and embrace failure is a key learning behaviour in high reliability organisations.1 Failure, however, is not the only source of learning. To focus all improvement efforts on failure would be missing the point: we should aim for a learning culture, in which we learn from all available opportunities—from failure, from everyday success, and crucially from excellence.
Dictionary definitions of excellence are easy to grasp, but they leave out one critical component, that excellence is often subjective, seen through the eye of the beholder. For example, a neonatology trainee who has recurrently failed to intubate a newborn infant achieves success after making an adjustment to practice. From different viewpoints, this success is excellent (from the trainee’s view) or routine (from the observing consultant’s and the patient’s view). A nurturing supervisor will recognise the excellence and will provide positive feedback to consolidate learning and improve motivation.
This type of excellence is highly prevalent in healthcare, yet there is a prevailing assumption that the most valuable learning opportunities are failures. Problems and deficiencies are seen as the best sources of improvement, and we tend to assume that we should learn primarily from negative feedback. The following are typical sources of learning opportunities used in improvement in healthcare:
Safety and quality metrics: the patient safety industry is unilaterally focused on identifying error and harm to prevent recurrence. The hypothesis is that positive change will happen because of elimination of the negative. Similarly, quality and benchmarking exercises tend to focus on reducing negative metrics such as harm rates and never events, rather than building on opportunities or inflating positive metrics.
Improvement project aims: quality improvement (QI) projects typically start with the question ‘what problem do we want to solve?’2 An alternative approach is to ask ‘what opportunity do we want to create’ or ‘on what success do we want to build?’
Educational feedback: when seeking educational feedback, we tend to seek out constructive feedback—‘how can I improve’, rather than ‘what am I good at?’ In their 2017 paper, ‘Shopping for confirmation’, Green et al 3 noted ‘personal improvement is generally thought to require a constant evaluation of one’s deficiencies’. Even if we do not actively seek negative feedback, it is the feedback to which we are most sensitive and to which we give the most value.4
Our preference for negative feedback is a deficit-based model. Yet most interventions in healthcare are successful, so there are many opportunities to embrace excellence and learn from success (a strengths-based model), as a complementary approach to studying failure. However, the strengths-based approach does not come naturally: our preference to learn from failure is well described and relates to several factors, including our innate negativity bias (we tend to pay more attention to negative events than to positive events of equal value4 and to media reporting—most media reports are negative, resulting in public perception and discourse which almost entirely focuses on weaknesses and deficits).
While it is essential to recognise and to learn from failure, a unilateral focus on poor performance is not enough if our goal is to achieve mastery. To capitalise on learning from success (both routine and outstanding success) we need methods to capture the right insights.
The idea that we can learn from everyday success is a feature of Safety-II, a concept developed by Hollnagel et al.5 In Safety-II, safety is considered a condition in which as many things as possible go right, rather than a condition in which as few things as possible go wrong. Reframing safety in this way reveals learning opportunities across the whole landscape of work from failure to success (table 1). This approach can be extended outside the domain of safety—for example, to the performance of a team or learning a new task.
Reframing safety: key elements of ‘Safety-II’5
In fact, success may be more instructive than failure for several reasons:
Success in healthcare is much more common than failure, so learning opportunities are easier to find.
In most cases, there are fewer ways to do things right than to do things wrong, so studying success will result in a brief list of ‘things to do right’, rather than a lengthy list of ‘(rare) things to avoid’.
Research from neuroscience and psychology has shown that, in many contexts, positive feedback (learning from success) is superior to negative feedback (learning from failure):
Negative feedback is of course still vitally important, particularly when used as corrective feedback for dangerous or serious errors.9 Our sensitivity to negative feedback may enhance our ability to recognise it and respond to it. However, it must be used carefully—in some cases it may impair learning10 and may also decrease intrinsic motivation.11 This latter effect is of relevance in healthcare where there is a growing awareness of psychological morbidity in staff, a contributory factor of which is a deficit-based culture of fear and blame.12
What practical steps can we take to embrace excellence and positive feedback?
The first step is to notice excellence. While this may sound obvious, due to the prevailing negativity bias it does not come easily without practice. It is important to remember that excellence can be subjective. A change in perspective is required, which requires positively framed reflection on our work. Timing is crucial: a tick-box approach to reflection with the prompt ‘what went well’ during a meeting such as a safety huddle may lead to forced recollection of events which lack learning value. An alternative approach is to reflect during transition points in work (eg, during or immediately after an interaction or procedure). This may trigger more sincere recognition of excellence and provide an opportunity for in-the-moment positive feedback.
As with negative feedback, positive feedback should be specific and descriptive; it should aim to identify excellence in practice, not in other characteristics, such as personality. Sincerity is key; rather than ‘thank you for your hard work’ from the team leader to the entire shift, it can be more effective to seek out individuals and describe to them what they did well.
If it is not practicable to provide in-the-moment feedback, written feedback is an excellent alternative, ideally delivered as soon as possible after the event. Written feedback can be stored and used for formal reflection, as recommended by the General Medical Council’s reflective practitioner guidance.13 Written feedback can be provided by email, card or via a Learning from Excellence reporting system,14 which has a variety of names in the National Health Service (NHS), such as ‘Greatix’.15
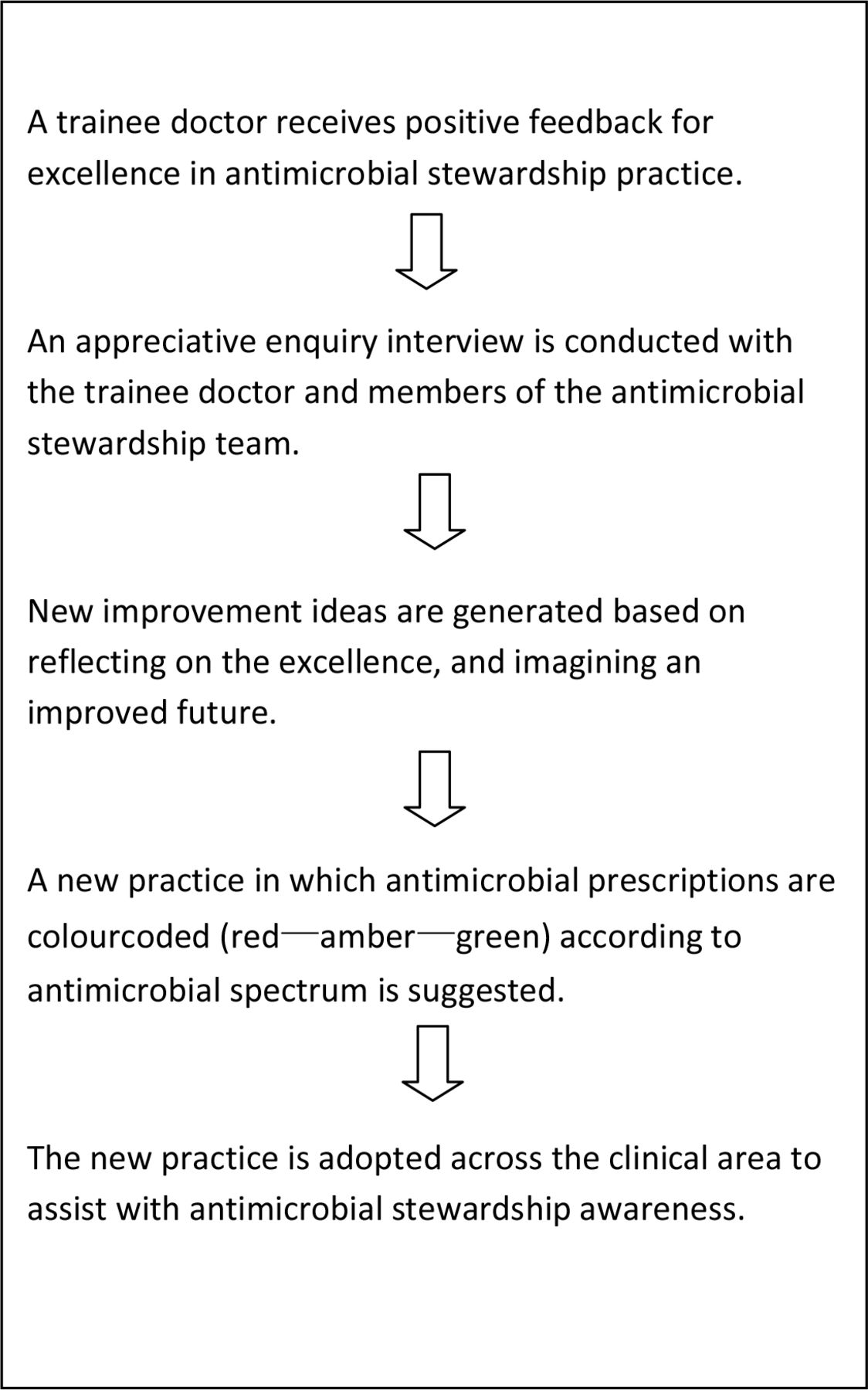
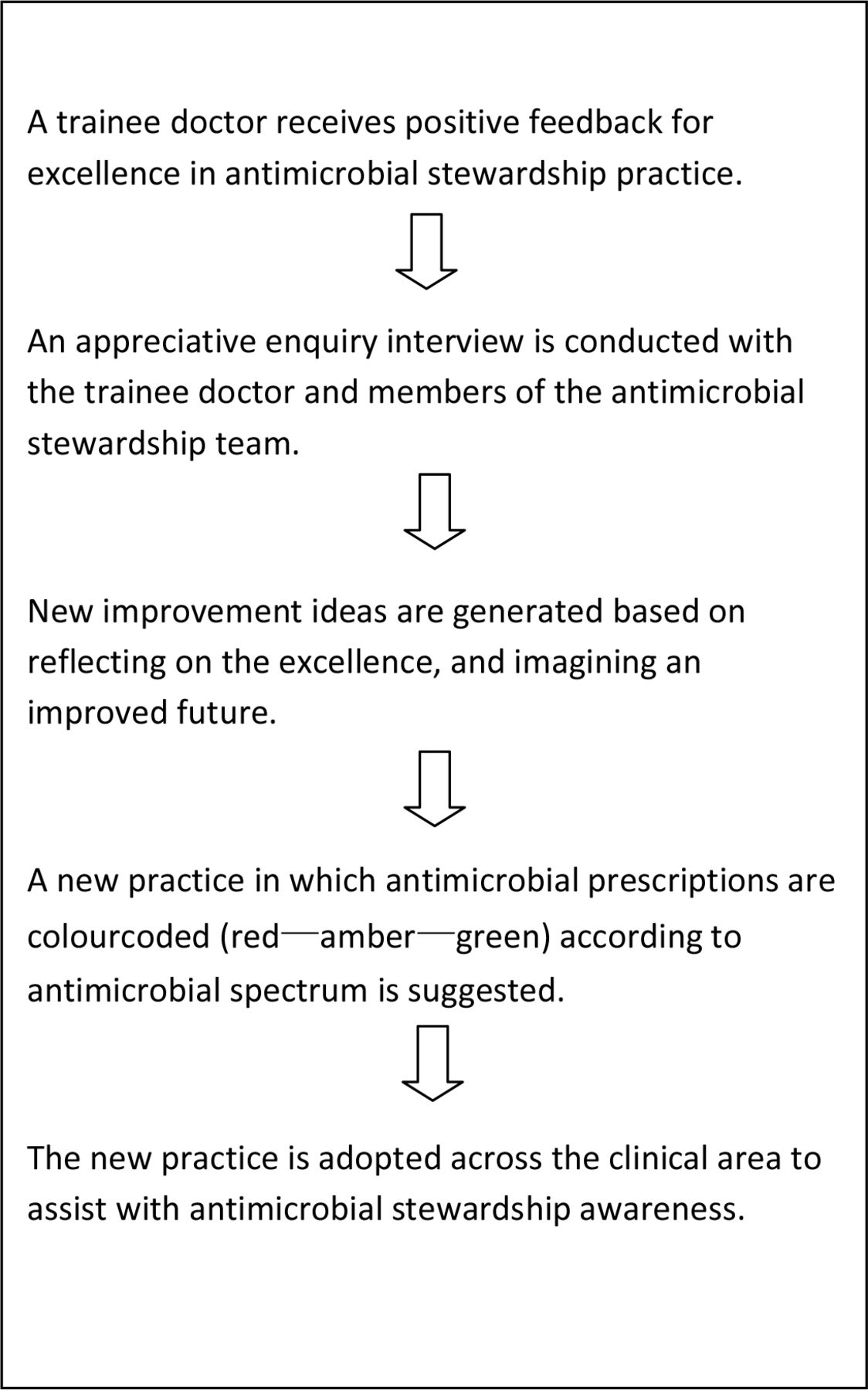
Selected episodes of excellence can be examined using appreciative enquiry, most known by its US English spelling, appreciative inquiry or ‘AI’.16 AI is a strengths-based semistructured conversation designed to consolidate learning and generate improvement ideas (table 2). This approach has been successfully used with positive feedback via excellence reporting as a QI intervention in healthcare,17 highlighting the potential of strengths-based approaches to organisational learning and QI. A simple example of this approach is shown in figure 1.
Phases of appreciative enquiry
{kind=link}
Example of a generative impact of appreciative enquiry.17
Patients and relatives provide a vital source of feedback. Most patient feedback is positive, yet this is rarely mined for actionable intelligence. Positive feedback from patients can reveal characteristics of high-quality healthcare and reinforce important behaviours and service delivery.18 Patient feedback is usually characterised by gratitude, the expression of which has many benefits for staff as well as patients and families. Expressing gratitude provides positive reinforcement for ‘good’ behaviours.19 The role of this effect in healthcare organisations may have untapped promise—not only in QI,17 but also in cultural change, for example, as a complementary approach to stamping out unwanted behaviours. Expressing gratitude is also beneficial to well-being, an important concept in today’s NHS. This applies to the individual who is doing the expressing,20 as well as the recipient, and the positive effects extend to improvements in relationships21—a key component of healthy teams.
In conclusion, excellence is highly prevalent in healthcare, and yet it is not routinely examined for improvement insights due to the prevailing tendency to focus our learning efforts on failure. A more balanced approach to learning, through increased recognition and positive feedback for excellence, can improve our ability to learn as individuals and teams, and may also offset the negativity associated with blame which tends to hinder our ability to learn from failure.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @lfecommunity
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.