Article Text

Abstract
Measurement of fractional exhaled nitric oxide (FeNO) has become a mainstream, NICE-recommended, objective test of asthma severity. We explore the uses and practical issues with the FeNO test using clinically relevant questions for general paediatricians.
- physiology
- adolescent health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Case history
A 12-year-old boy, Jamie, is seen in a DGH respiratory clinic following a recent hospital admission with a life-threatening exacerbation. He has had one previous life-threatening exacerbation of asthma, and is thin, coughs intermittently and denies wheezing or feeling ‘tight-chested’. He is currently on an inhaled corticosteroid, oral montelukast and salbutamol if needed. His mother is a smoker and they are suffering with dampness and mould in their house. He claims to be taking his steroid inhaler regularly but his general practitioner (GP) records note his prescriptions of salbutamol are collected fortnightly, but his steroid inhaler has not been collected in 6 months.
You have heard about an objective test of airway inflammation: fractional exhaled nitric oxide and wonder if this could be useful here.
Introduction
Asthma is defined as airway hypersensitivity and inflammation.1 It is a chronic condition that often affects children, with one in 11 children in the UK living with asthma.2 Globally, there are approximately 300 million people with asthma and annually up to 250 000 die prematurely, with 90% of these deaths thought to be avoidable.2 As a result, it is important to diagnose and treat asthma early to prevent this. In diagnosing asthma, it is important to consider the presence of symptoms with variable airflow obstruction.3 Distinguishing asthma from other causes can present clinicians with a diagnostic challenge.
Asthma is associated with 4.1 million general practitioner (GP) consultations and greater than 25 000 UK annual paediatric hospital admissions, with an associated annual cost of over £1 billion.4 Evidence has shown that asthma control is often suboptimal. The National Review of Asthma Deaths (NRAD) showed that 57% of patients who died from asthma were being supervised in primary care alone, and 46% of deaths were found to be associated with a lack of implementation of asthma guidelines.5 The main aims of asthma management include preventing exacerbations, hospital admissions and monitoring asthma control. Previously, objective and subjective measures have been used to assess this such as questionnaires, peak flow and spirometry. Recently, a more discriminative test has become more widely used in asthma management: fractional exhaled nitric oxide (FeNO), which is now NICE-recommended in the assessment and monitoring of asthma. We aim to outline the test and discuss its usefulness in clinical practice. Online supplemental appendix 1 demonstrates the search strategy for this article.
Supplemental material
Physiological background
Asthma can be divided into extrinsic (allergic, atopic), intrinsic (non-atopic) and occupational.3 Atopy is characterised by a genetic predisposition to produce IgE against environmental allergens. Atopic asthma is related to Th2-lymphocytes which induce airway inflammation.
Nitric oxide (NO) is produced in normal, healthy lungs at a low level.6 In asthma, an eosinophilic pattern of inflammation is observed which leads to an increased production of NO.6 The majority of exhaled NO is produced by inducible NO-synthase (iNOS) in the respiratory epithelium. In asthma, there is often upregulation of iNOS expression due to the activity of IL-4 and IL-13 (types of Th2 cytokines).6 Therefore, exhaled NO signals Th2-lymphocyte-driven inflammation in the bronchial mucosa and may be useful in asthma diagnosis. The American Thoracic Society advocate that compared with other traditional tests, FeNO may have advantages in identifying eosinophilic airway inflammation.7 In this way, one can identify patients who are most likely to benefit from an adjustment in inhaled corticosteroid (ICS) regimen since this type of inflammation responds well to ICS as well as aid in identifying treatment non-adherence.7
Technological background
FeNO measures the levels of NO when the patient breathes out, measured as parts per billion (ppb) in expired air. In schoolchildren, a FeNO level of ≥35 ppb is regarded as a positive test.1
Alongside clinical history, peak flow and spirometry, it helps to confirm an asthma diagnosis. It is useful when the diagnosis is unclear and to determine the specific type of asthma the person has as high levels of NO are indicative of ongoing allergic asthma. In this way, it is useful in aiding clinicians to adjust the management plan. It is suitable for children over the age of five. FeNO testing is available in some GP surgeries and hospital settings. This method is simple to use, can be performed in approximately 10 min and is inexpensive.1 Basic training is needed for non-clinical staff.
There are three separate devices which have been produced to measure exhaled NO, have been evaluated by NICE and are the most broadly used in clinical practice. These are: NObreath, NIOX MINO and NIOX VERO.1 8 All of these models are handheld. Tests such as spirometry and peak flow have been found to be difficult for children to use. In contrast, FeNO is feasible for young children since child-friendly software is available which explains the correct method of use. Figure 1 is an example of the NIOX VERO machine in use, demonstrating the software.

A photo demonstrating the NIOX VERO machine in use and the software available on the screen for children.1
Cost
A cost-analysis was performed by the NICE (NG80) guideline committee, summarised by table 1.1 This analysis concluded that the average total cost per FeNO test is £10.01–13.66. This takes into account the consultation duration, staffing and the machine cost.
A table to show the estimated cost of FeNO1
It is also important to consider the annual medication costs of managing children with asthma.1 By using a diagnostic strategy integrating FeNO with a high diagnostic specificity, it would be possible to reduce costs from overprescribing for children without asthma as well as supporting safer inhaler switching. A systematic review of 67 randomised controlled trials (RCTs) assessed the clinical and cost-effectiveness of different therapeutic management strategies including ICS and long-acting beta2 agonists in adults and children (≥12 years) with chronic asthma. They estimated the cost-saving from inhaler-switching to be up to £201 per patient per year.9
The NICE guidelines (NG80) concluded that the most cost-effective strategy in diagnosing asthma incorporates spirometry, bronchodilator reversibility, FeNO, peak flow and a methacholine challenge test in varying combinations depending on whether the spirometry result was obstructive or non-obstructive. The incremental cost-effectiveness ratios of adopting this strategy were less than £20 000 per quality-adjusted life year (QALY).1 A sensitivity analysis was performed which showed that when the cost of FeNO increases above £93 per use, none of the diagnostic strategies were cost-effective at a £20 000 per QALY threshold.1 This threshold would only be reached if the machine was used less than 28 times over 5 years. Above this level of use, practicable in most GP practices, would make FeNO cost-effective.
Clinical questions
Can the test be used to diagnose asthma? Is FeNO more accurate than spirometry or peak flow diaries?
Asthma is a clinical diagnosis and as a result, there is no single diagnostic test. NICE guidelines recommend that for children under 5 years with suspected asthma, their symptoms should be treated according to clinical judgement and have regular reviews. Once they reach 5 years, symptomatic children should undergo objective testing, including spirometry, bronchodilator reversibility or FeNO testing.1
Asthma can be diagnosed if the patient has symptoms suggestive of asthma and a FeNO level of ≥35 ppb with positive peak flow variability or obstructive spirometry with positive bronchodilator reversibility (table 2). In children, a FeNO level of ≥35 ppb makes asthma (and a response to ICS) very likely.3
A table to show the positive test thresholds for objective tests used to diagnose asthma in children and young people (aged 5 years and older)1
Current guidance advocating serial monitoring (peak flow readings or spirometry) to confirm diagnosis may miss mild asthma as abnormal airway physiology may be undetectable, suggesting these tests used serially have a low sensitivity.2 3
Research has shown that the predictive values for FeNO are higher than that of traditional diagnostic methods.10 Table 3 below summarises the diagnostic accuracy of FeNO compared with traditional methods.3 4
Diagnostic accuracy of FeNO testing (≥35 ppb) in diagnosing asthma compared with traditional methods3 4
Diagnostic accuracy
This indicates that FeNO has a moderate to high sensitivity and a high specificity, based on high-quality evidence.3 NICE recommend that FeNO can only be used to assist in the diagnosis of asthma in children (alongside other investigations) if there is diagnostic uncertainty such as either normal spirometry or obstructive spirometry without bronchodilator reversibility demonstrated.1 This is because there is scope for significant misdiagnosis of asthma, with both false positive and negative errors. Although asthma pathophysiology is often associated with eosinophilic airway inflammation, this is not always the case. This is useful in interpreting FeNO results since in cases of asthma that are not due to airway eosinophilia, FeNO levels may be low.7 Furthermore, there is overlap between FeNO levels observed in patients without asthma and in patients with atopic asthma.7 This means that a raised FeNO level is supportive of a diagnosis of asthma, but is not conclusive.
Figure 2 is a flowchart summarising the asthma diagnostic pathway, incorporating FeNO. This is based on current NICE and BTS guidelines. Overall, the BTS guidelines conclude that a positive FeNO test increases the probability of asthma but a negative test does not exclude asthma. Nevertheless, FeNO has a high diagnostic accuracy relative to all other diagnostic tests performed in primary care. Therefore, it is appropriate to give all patients who have undergone a spirometry test and bronchodilator reversibility testing, a FeNO test.8

A diagram to summarise the asthma diagnostic pathway, adapted from the NICE asthma guidelines and BTS asthma guidelines.1
Clinical bottom lines
A raised FeNO level is supportive of asthma but not definitive.
FeNO has a high diagnostic accuracy compared with other available diagnostic tests in the primary care setting.
Can the test be used to monitor response to asthma treatment and tailor asthma interventions?
NICE guidelines (NG80) recommend that children with asthma should be reviewed annually. This should include monitoring exacerbations, inhaler adherence/technique and symptom scores. The NRAD was conducted by the Royal College of Physicians in 2013.5 This review identified 195 patients (28 children) whose case met the inclusion criteria and had died from asthma. Of those patients who died, 39% had been prescribed greater than 12 short-acting reliever inhalers in the previous year and 4% over 50.5 In contrast, preventer inhalers were underprescribed.5 This highlights a trend of over-reliance on reliever medication, a lack of monitoring of response to asthma interventions and a lack of assessment of future risk.
Analysis has shown that using symptom scores in isolation can lead to a significant number of children being overtreated. New monitoring strategies for asthmatic children should target poor asthma control to prevent further morbidity or mortality. FeNO offers additional information by quantifying the degree of eosinophilic airway inflammation over time.1 The test can identify patients who are likely to be steroid-responsive and which patients would benefit from adjusting their ICS regimen rather than other treatment options. NICE recommend that FeNO should be used before commencing ICS therapy. A raised FeNO presteroid therapy can be a good predictor of response to treatment.1
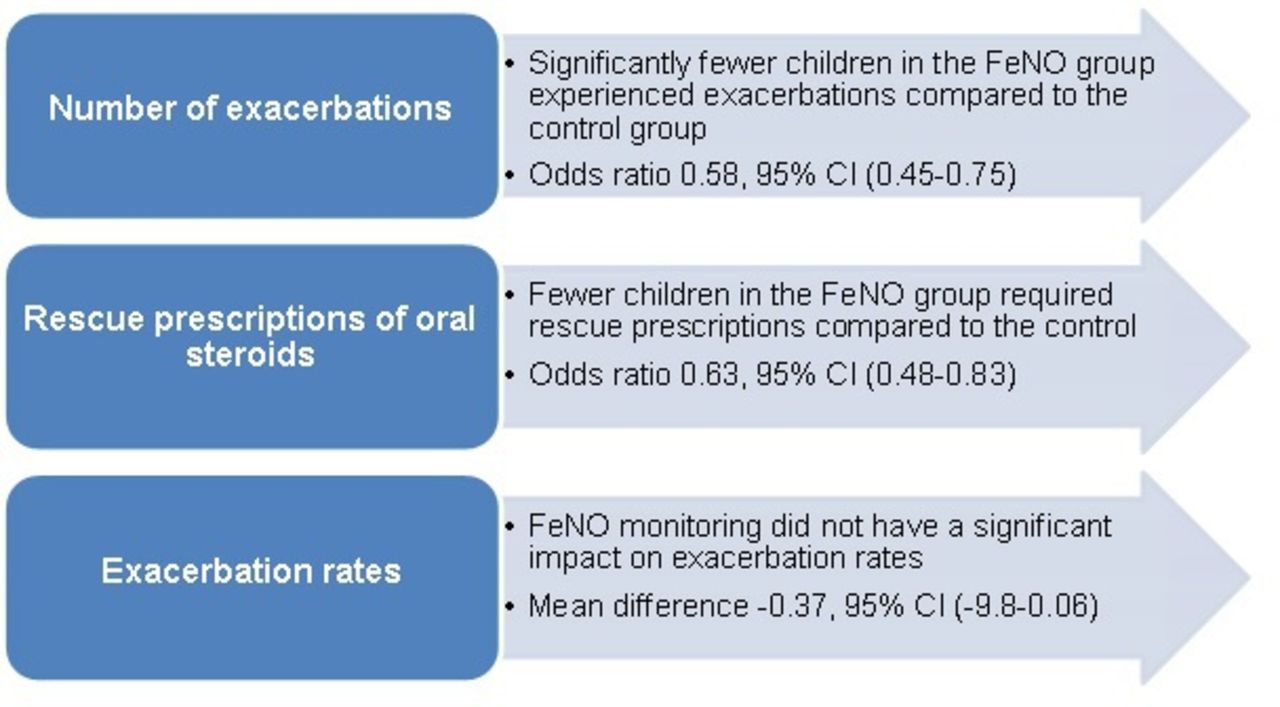
A Cochrane Review (figure 3, 2016) evaluated the efficacy of tailoring asthma interventions according to FeNO levels.11 They included nine RCTs involving 1426 children, placed in either the FeNO monitoring group or the control group. Control group interventions included symptom score, spirometry and peak flow to guide treatment adjustments. All of the review studies were hospital-based, affecting their relevance in primary care.
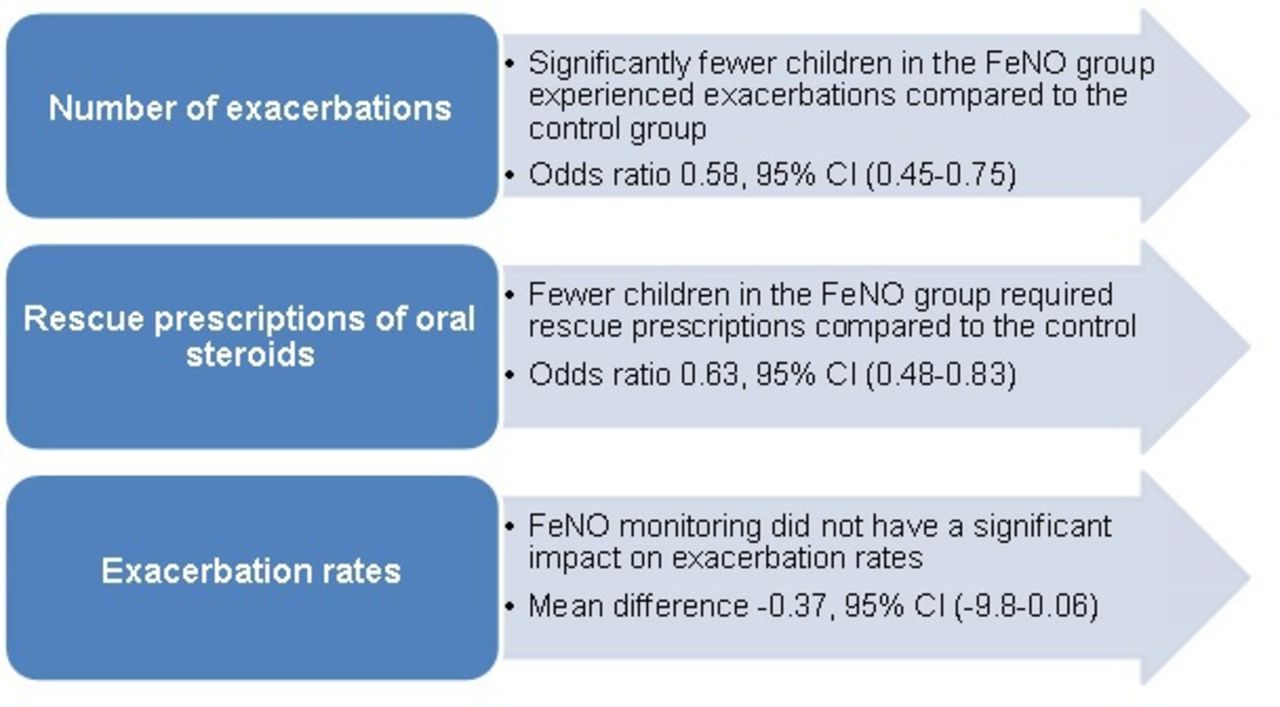
Petsky and Chang: exhaled nitric oxide levels to guide treatment for children with asthma. (Cochrane review): key results summary.11 FeNO, fractional exhaled nitric oxide.
Overall, the review concluded that using FeNO to tailor asthma therapy cannot be universally advocated. However, the review used the number of patients who had exacerbations during follow-up as the primary end-point and did not adjust for multiple exacerbations during the study period.1 The National Institute for Health considers asthma exacerbation rates as the most valuable outcome for assessing asthma exacerbations.12 Reanalysing the review data using asthma exacerbation rates as the end-point demonstrated that the exacerbation rate was significantly lower in patients receiving FeNO-based asthma management.13
Price et al performed an observational study (2013) analysing clinical data to identify patterns of FeNO in UK primary care and its effects on physician/patient behaviour. This aimed to inform algorithms for the use of FeNO in practice (figure 4).14 A total of 678 patients aged 4–80 years were included, involved in routine FeNO measuring. Using published evidence and the study results, the authors developed a clinical algorithm using FeNO for monitoring patients with asthma.
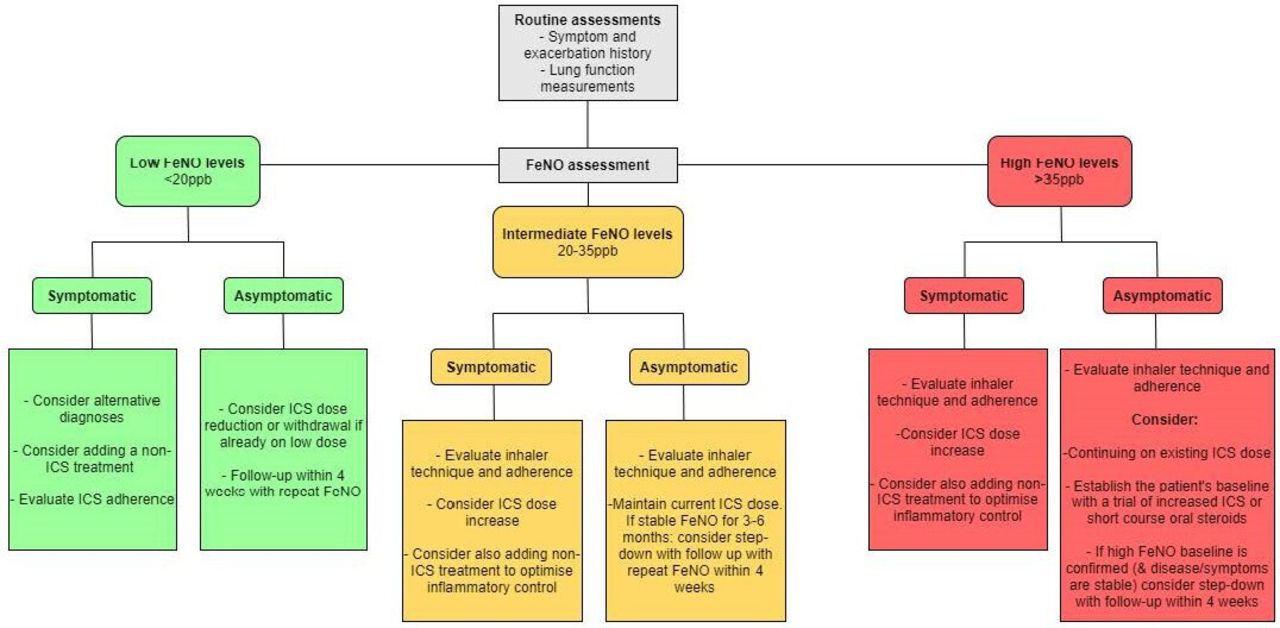
Algorithm for the management of asthma based on FeNO levels (adapted from Price et al): FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroid.
Clinical bottom line
NICE do not currently recommend the routine use of FeNO to monitor asthma control as there is a lack of sufficiently powered studies demonstrating benefit. However, FeNO can support management in symptomatic children despite using ICS and in specialist asthma clinics.1 Further research is needed into the role of FeNO in asthma monitoring.
In children with asthma, is FeNO more reliable than clinical history, spirometry or peak flow in predicting future asthma exacerbations? Can the test be used to measure ICS adherence?
Research has shown that the majority of patients with asthma with treatment failure have an associated lack of ICS adherence. Furthermore, studies have shown that in children referred to tertiary care with ’severe asthma', adherence with prescription collection was below 80% in over half of the cohort.15 This can lead to increased unplanned healthcare attendances (UHAs), the provision of oral corticosteroids, and in some cases, death. Furthermore, exacerbations can reduce lung function and increase time off school/work.1
International guidelines recommend that non-adherence should be considered in all patients with severe asthma that is difficult to control before considering treatment escalation.16 However, detecting this non-adherence can be difficult, with self-reported and parental-reported adherence often overestimated.17
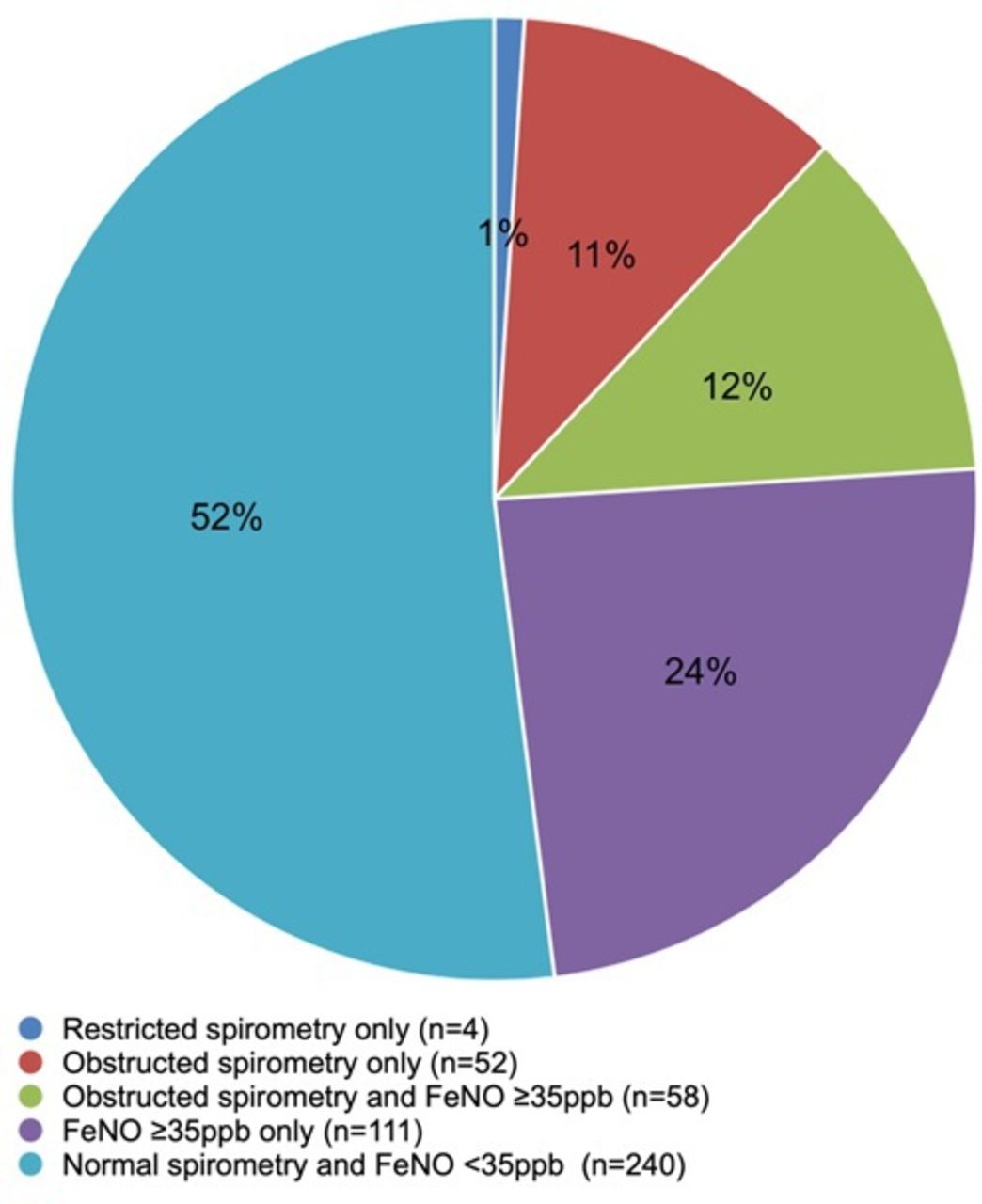
Lo et al conducted a UK prospective observational cohort study.17 Using spirometry, FeNO and asthma control test (ACT) scores, they assessed the prevalence of abnormal spirometry and FeNO in 614 children with asthma across 10 general practice settings. They then explored the inter-relationship of this with asthma control and measured the number of UHAs. They found that almost 50% of the cohort reported good asthma control based on their ACT score but had at least one objective test abnormality, with 12% having both abnormal spirometry and FeNO.18 This suggests that symptom-based evaluation of asthma severity and control may lead to under-recognition and suboptimal control. Abnormal pulmonary function and FeNO levels are common in children presenting to primary care for an asthma review. Figure 5 further demonstrates the results of this study.17

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A diagram demonstrating the percentage of children with normal compared to abnormal objective tests. Adapted from the study performed by Lo et al.17
In total, 25% of the cohort had a raised FeNO level without abnormal spirometry. Furthermore, at follow-up 6-month postreview, the mean number of UHAs fell from 0.31/child in the 6 months preceding the review to 0.2/child (p=0.0004). There was also an increase in median ACT score from 20 to 22 (p=0.032).17 This demonstrates the benefits of FeNO monitoring and regular asthma reviews in reducing morbidity and mortality, and identifying those with poor adherence. This is further supported by the study published by Heaney et al in the adult cohort that found that FeNO suppression testing was an effective method of identifying non-adherence to ICS in patients with poorly controlled asthma.18
An observational UK study of 93 children aged 5–17 years assessed ICS adherence using electronic-monitoring.19 This was compared with self-reported adherence, FeNO and spirometry. They showed that suboptimal adherence (<80%) was found in 58% of children. There was no significant difference observed between the varying adherence groups and the measured parameters at the start of monitoring (such as FeNO, FEV1). Over the monitoring period, a significant but weak correlation was found in changes in asthma control between adherence and FeNO (r=0.46; p<0.001) whereas no correlation was found with the other monitoring groups.19
Clinical bottom lines
Consistent evidence has not validated whether FeNO can be used to monitor adherence. Therefore, this is not routinely advocated by NICE.
Despite this, FeNO is potentially a valuable biomarker when used alongside adherence monitoring in order to influence management decisions in patients who are symptomatic despite using ICS.1
Limitations
Studies have shown that a positive FeNO test is supportive of an asthma diagnosis. However, this is not conclusive since there are many confounding factors which can influence results.2 This is summarised in table 4.
Factors affecting measured FeNO levels1
A cross-sectional analysis of 276 children was conducted in Finland.20 They completed a questionnaire and underwent medical assessment, including FeNO. A total of 114 healthy, non-atopic, school-aged children were included. Patients with a history of atopy, infection, abnormal lung function and smoking were analysed separately. They found that FeNO was significantly associated with age (p<0.0001) and height (p<0.0001), but not with gender (p=0.42).20 Research has shown that height is the best determinant of FeNO in healthy children. On average, an increase in height range of 120–180 cm leads to an increase in FeNO from 7 to 14 ppb.20 This highlights the importance of interpreting FeNO results in their clinical context and considering proposed models when analysing data.
Furthermore, increased FeNO levels are affected by atopy (OR 9.0, 95% CI, p<0.0001), allergic rhinitis and atopic dermatitis independent of the child having asthma.20 Therefore, FeNO levels should not be interpreted without knowing the child’s atopic status.
Clinical outcome
Jamie’s FeNO was 55 ppb. This result enabled an honest conversation about ICS use. Jamie noted that he had recently lost his steroid inhaler but was keen to return to playing football. He restarted his ICS and was considered for a combined ICS/long-acting reliever such as Symbicort SMART and once daily Relvar to help with adherence. Given his previous life-threatening exacerbation, he was referred to the tertiary multidisciplinary team respiratory clinic. In the meantime, a home visit by the respiratory nurse identified significant damp and mould. Two months later, his FeNO had improved to 14, with improved symptom control. The council had remediated the problems with the damp and mould. He was also back playing football.
Conclusion
There is currently a lack of evidence demonstrating a statistically significant benefit associated with FeNO measurement in order to support its routine use in asthma monitoring in primary care. Studies indicate that FeNO monitoring is associated with a reduction in asthma exacerbations owing to the appropriate targeting of increased ICS dose. Furthermore, FeNO has the potential to be cost-effective due to the associated reduced costs of hospitalisation and adverse complications. Further data are needed to define the optimal decision thresholds and the specific role of FeNO in asthma monitoring. The test is associated with low cost, ease of use and reproducibility.
Test your knowledge
Which of these FeNO levels is raised, in a new patient with suspected asthma?
12 ppb
20 ppb
40 ppb
60 ppb
100 ppb
FeNO is likely to be falsely raised in which of these groups?
Children with rhinovirus
Children who smoke tobacco
Children with allergic rhinitis
Children who vape
Which of these test results for asthma are clinically significant?
Bronchodilator reversibility (BDR) test: improvement in FEV1 of 15%
FeNO 50 ppb
Spirometry: FEV1/FVC ratio 75%
Peak flow variability 25%
You review an 8-year-old boy who is taking a fluticasone 50 mcg inhaler for asthma (two puffs two times a day) and salbutamol (two puffs two times a day and as needed). He produced a FeNO of 12 ppb and reports being well. Would you consider:
Reducing his inhaled steroid dose (to one puff two times a day)
Increasing his steroid dose (to three puffs two times a day)
Switching him to beclomethasone (two puffs two times a day)
Retesting FeNO if his symptom control changes
What is the estimated cost of FeNO per patient (in an outpatients setting)?
50p
£10
£50
£100
Answers to the quiz are at the end of the references.
Answers to the multiple choice questions
C, D, E
A, C
A, B, D
A, C, D
B
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RH and MPT were involved in the literature review, writing and editing of the paper. SW and MV were involved in the review and editing of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.