Article Text

Statistics from Altmetric.com
The 2020 British Society for Paediatric Endocrinology and Diabetes (BSPED) guideline differs from the previous iteration and the more conservative National Institute of Health and Care Excellence 2016 guideline for diabetic ketoacidosis in children and young people (2015). It recommends a more liberal approach to initial fluid resuscitation and a reduced enthusiasm for using inotropes. This contrasts with shock resuscitation guidance elsewhere. In septic shock acute fluid resuscitation is now recommended to be more selective and conservative, and the early use of vasoactive drugs is supported.1
So why did BSPED make a new recommendation for diabetic ketoacidosis (DKA)? Recent correspondence2 suggests that it arose from: (A) expert interpretation of physiological data suggesting hypoperfusion as the precursor to cerebral oedema; (B) the Pediatric Emergency Care Applied Research Network (PECARN) fluid in DKA randomised controlled trial3 and (C) regional audit data. Such evidence is not compelling.
Physiological and imaging data suggest cerebral hypoperfusion may not be present at baseline. In 1948, Kety et al 4 measured cerebral blood flow (CBF) in adults with DKA: none had CBF below the normal range and several were hyperaemic. Glaser et al 5 interpreted MRI scans of patients in DKA as suggesting increased CBF. Some of this excess may have resulted from treatment. If concern about hypoperfusion is key, it is not clear why increasing perfusion with inotropes rather than fluid is discounted. Inotropes have the advantage of not reducing osmolarity, and rapid falls in osmolarity probably contribute to cerebral oedema. The PECARN study3 was prompted by concerns about this mechanism. It compared high and lower volume and tonicity fluid regimens in children with DKA. There was no difference in the primary outcome of significant neurological deterioration. Children at high risk of cerebral oedema at baseline were excluded, and clinically evident brain injury was so rare: 12 episodes (0.9%) that the study was not powered to inform on relative risk. Last, use of unpublished audit data in the development of guidelines is unconventional. Most guidelines state the methodologies in advance and specifically avoid the use of non-peer-reviewed data as a potential source of bias.
Perhaps something more fundamental needs to be considered when discussing intravenous fluid resuscitation. This is a very difficult area to study. There is no high-performing, or universally accepted, definition of shock in children; hypotension definitions are problematic, and the severity of shock does not always relate to the probability of a poor outcome; positive acute physiological responses (improvements in heart rate and perfusion) correlate poorly with outcomes, the risks and benefits of fluid resuscitation are highly sensitive to the cause of shock (eg, myocarditis less benefit than hypovolaemia), the timing (early resuscitation more benefit than late resuscitation) and the healthcare system in which the resuscitation is being provided (greater risk when no access to positive pressure ventilation, lower risk on an intensive care unit).1 Defining shock is especially problematic in DKA. Acidosis and hypocarbia cause a range of clinical features independent of tissue oxygen delivery, for example, tachycardia, tachypnoea and reduced skin perfusion,6 7 and adaptive metabolism (eg, raised serum lactate8) that can easily be misinterpreted as signs of shock.
The degree of physiological disturbance with severe acidosis, tachypnoea and poor perfusion would be associated with very poor prognosis if it resulted from septic shock or other systemic insults. DKA is different. How different can be illustrated with the physiologically based scoring system the Paediatric Index of Mortality 3. The values of a base excess −30 mmol/L, with an arterial partial pressure for oxygen (PaO2) of 10 kPa in 25% oxygen and a systolic blood pressure of 100 mm Hg estimates a risk of mortality of 9.7% without DKA but only 1.2% with DKA.9 This estimate fits with the reported mortality of DKA (0.5%–2%).
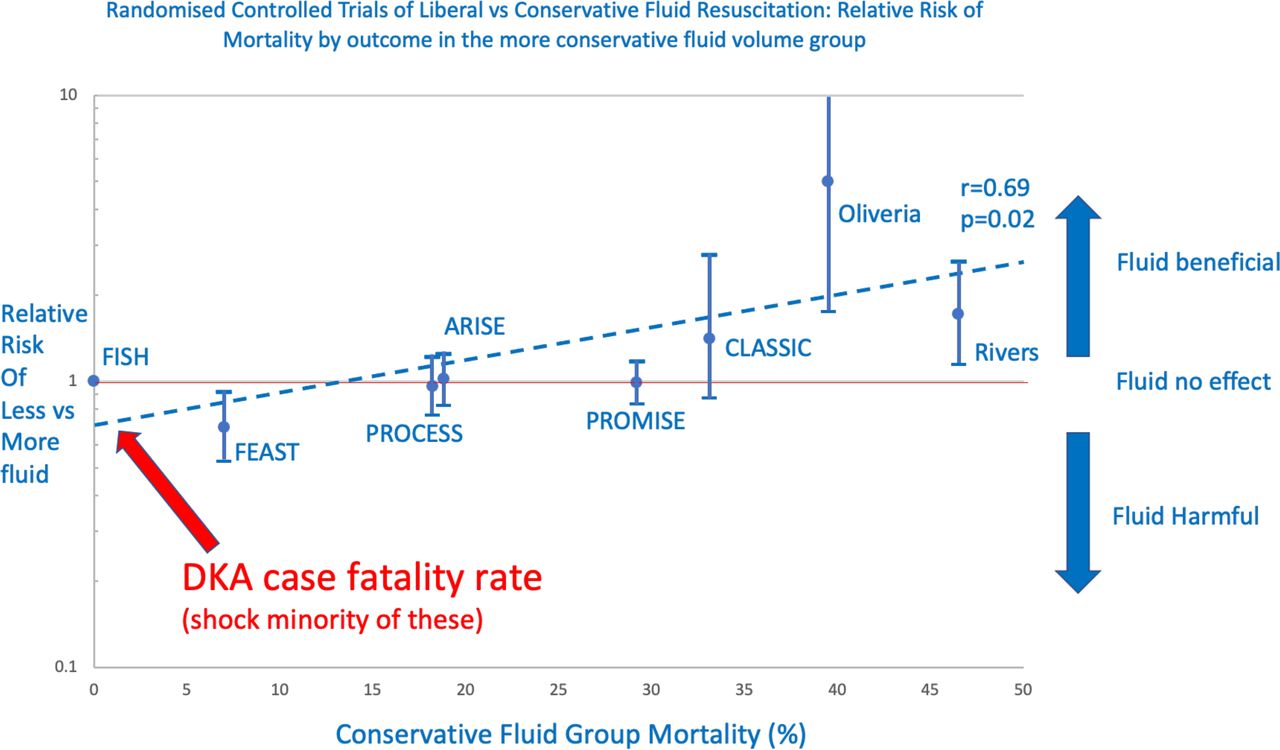
‘What is the risk of death from shock?’ should be the key question when balancing the risks and benefits of fluid resuscitation. Trial evidence illustrates this point (figure 1). ‘Early-goal directed therapy’ (EGDT) describes an approach of increased monitoring for subclinical shock. EGDT results in more aggressive fluid resuscitation and dramatically improved outcome in randomised trials in adults and children. However, this effect is only seen when the control group mortality is very high (39%–49%).10 11 When similar trials were repeated in lower risk populations (control group mortality 18%–22%), they offered no net benefit.12–14 Indeed, the only large high-quality trial of fluid resuscitation in children observed that fluid increased mortality in acute infective illness. Maitland’s Fluid Expansion as Supportive Therapy study had a ‘no fluid bolus group’ mortality of 7% and fluid resuscitation increased this to >10%.15 So, the ‘space’ for fluid resuscitation to improve outcomes was relatively limited, and the potential for harm was high. Of relevance to the management of fluids in DKA is that it carries a low risk of mortality—only a tiny subset of whom die from shock—on the continuum shown in the exploratory plot (figure 1). Therefore, potential opportunities for aggressive fluid resuscitation to improve outcomes are limited, and the potential for harm appears high. An aim for future guidelines might be a more approach stratified for the specific risks of cerebral oedema versus shock in an individual case.
{kind=link}
Randomised controlled trials of liberal versus conservative fluids resuscitation: relative risk of mortality in the more liberal group is shown against the mortality in the more conservative fluid group. There is a strong (r=0.69) correlation between the log of the relative risk and the conservative group mortality with the equation y=0.69e0.026x that is unlikely to be due to chance (p=0.02). In other words, fluid resuscitation is effective in shock with a high mortality risk but harmful in low-risk populations.10 11 13–16 DKA is a very low-risk population.
What we don’t yet know about the BSPED guidelines is: why they choose to recommend more aggressive resuscitation in a low-risk situation? Fluids carry a potentially important risk of harm even in the absence of the predominant additional risk of cerebral oedema. The general principle should be that we do not intervene without evidence. We don’t yet know where the balance of risks and benefits sits for early volume expansion in DKA. But any change requires a justification than can be considered by the potential users of the guideline.
Ethics statements
References
Footnotes
Twitter @pus27
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Guideline review
- Viewpoint
- Guideline review