Article Text

Abstract
Objective To describe a safeguarding decision pathway for the assessment of osteopenic fractures in non-ambulant children with cerebral palsy.
Method Literature review and consensus practice of a child safeguarding team, including clinicians and social workers.
Conclusion Low-energy fractures of the lower limb in non-ambulant children with cerebral palsy are relatively common and explained by the presence of reduced bone strength, in the absence of any other unexplained injuries or safeguarding concerns.
- child abuse
- endocrinology
- adolescent health
Statistics from Altmetric.com
Case scenario
A 10-year-old boy with bilateral cerebral palsy (CP) with spasticity Gross Motor Function Classification (GMFCS) V and severe cognitive impairment was transferred from respite care to a tertiary children’s hospital for investigation and management of a swollen, tender right lower thigh that was noted after being transferred from bed to wheelchair on the previous evening. X-ray revealed a fracture to the left distal femur.
Prevalence of fractures in non-ambulant children with CP
Non-ambulant children and young people with CP are prone to low-energy fractures from normal care activities such as lifting and transferring.1 Fragility fracture prevalence varies between 3% and 12% in children in children with predominantly Level V Gross Motor Function Classification (GMFCS; see box 1).2–4 Fractures can recur; the mean age to first fracture was 10 years in one study.2
GMFCS levels
Level 1: walks without limitations.
Level 2: walks with limitations.
Level 3: walks using a hand-held mobility device.
Level 4: self-mobility with limitations; may use powered mobility.
Level 5: transported in a manual wheelchair.
These fractures are generally occasioned by lack of a clear history of trauma, as they can occur during normal care activities. In addition, such an incident might not be recognised early due to difficulties in perception of the child’s pain.
You may be asked for advice when safeguarding and position-of-trust concerns arise, particularly if the fracture is found in an institutional care setting such as hospital or hospice, a special school or during respite care.
Safeguarding decision pathway
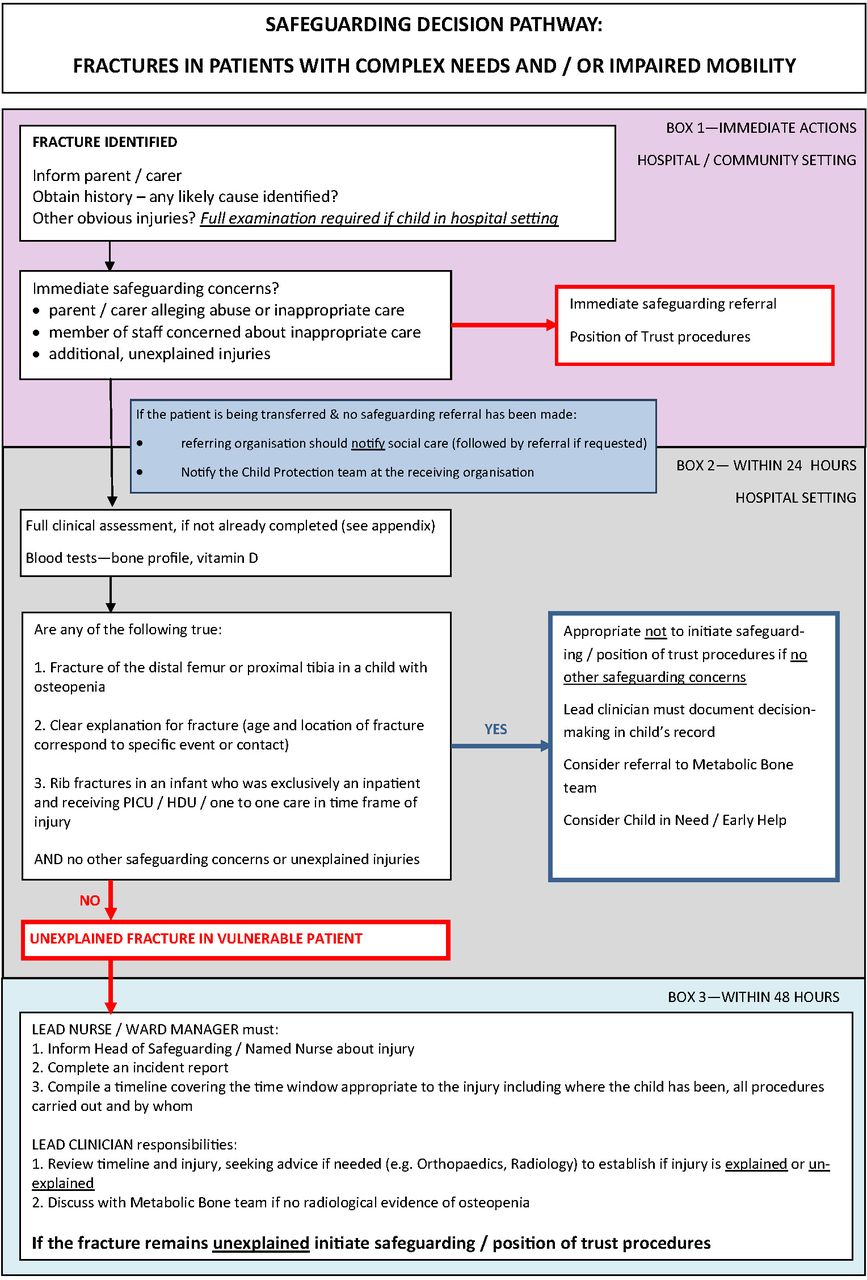
A safeguarding decision pathway (figure 1) was developed through evidence and consensus between clinicians, including a paediatric bone health expert, members of the hospital safeguarding team and a children’s social care lead for position of trust (a legal term in the UK that refers to certain roles and settings where an adult such as a doctor or care worker has regular and direct contact with children). ‘Carer’ is used throughout to include any primary caregiver but is usually the parents.
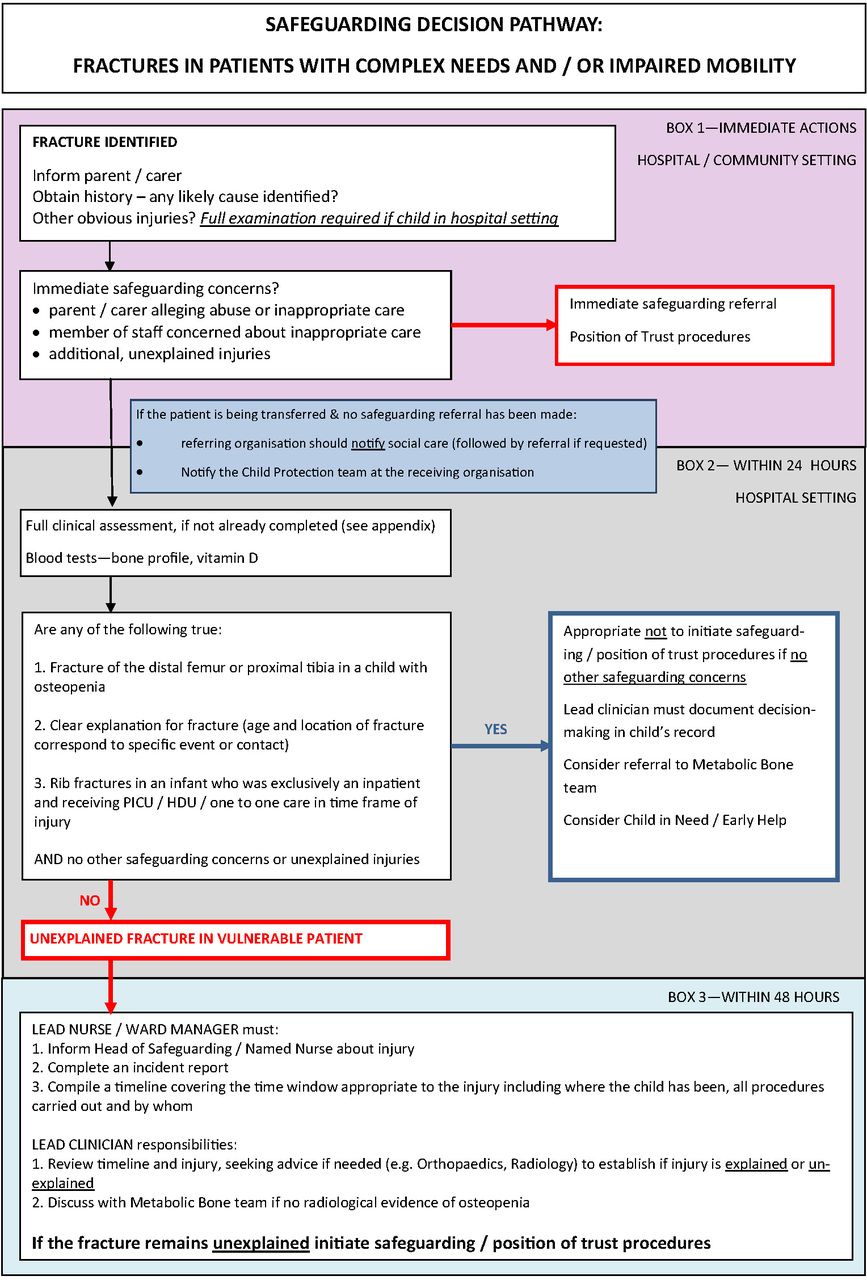
Safeguarding decision pathway.
Immediate actions
Once the fracture has been identified, inform the carers. Liaise with the child’s neurodisability team, if they are not already involved with the admission.
If there are immediate safeguarding concerns, such as a parent alleging inappropriate care by the respite care staff, make a safeguarding and undertake position-of-trust procedures (UK) or equivalent in other countries. If the respite care staff have concerns, they should refer to children’s social care and notify the receiving unit’s safeguarding team (figure 1).
If there are no immediate concerns, undertake a full clinical assessment and investigations.
History
Review the current medical and social history against the background of the child’s condition (box 2), in particular, symptoms, such as pain related to recent trauma or handling.
Points in history taking (not an exhaustive list)
Current presentation, with attention to discernible pain or other symptoms and signs in relation to recent trauma or handling, such as turning or transferring to wheelchair.
Severity of underlying condition – non-ambulant status; degree of spasticity/dystonia/athetosis; seizures; interventions; medication (including anti-epileptic drugs).
Immobilisation (from fractures or operations).
Dietary and feeding history – interventions (such as gastrostomy and any complications); concerns about growth (obtain most recent measurements); feeding difficulty (discomfort during feeds; time taken for a feed; food refusal; retching; reduced tolerance of overnight feeds; dental erosions (associated with ‘silent’ gastro-oesphageal reflux); and admission for episodes of aspiration).
Use of mobility and lifting devices.
Identify key worker, lead paediatrician (if not the same person) and other members of the multidisciplinary team).
Involvement of children’s social care disability team and other support services.
Intervals between respite care.
The majority of carers recognise pain and abnormal movement of the affected limb in their typical developing child with an accidental extremity fracture.5 When fractures are ‘found’, with no history of trauma, or accounts are vague, uncertain or changeable, safeguarding concerns arise.6 Non-ambulant children with CP commonly experience intense, recurrent episodes of pain7 to an extent that it becomes ‘part of them’, making it difficult to appreciate when acute pain is experienced.8 Thus, an external sign such as swelling might well be the first sign of fracture if expressed pain is difficult to perceive.
Pain assessment
Ask carers and therapists if they recognise the child’s behavioural responses to acute pain and whether these have changed recently, in an attempt to narrow down the time window for any trauma. Parents and main carers do become expert in assessing their child’s change in posture or behaviour in response to pain so this should go unheeded.
Case scenario (continued)
Our patient is Level V GMFCS, cognitively impaired and unable to communicate using language.
Chronic pain in this group can be intense but difficult to recognise due to the multiple aetiologies (such as spasticity, dystonia and ‘silent’ gastro-oesophageal reflux) and the complexity of the pain response.7 9 Assessment such as FACES are problematic as the child’s behavioural responses may be atypical (eg, clapping hands and not grimacing).10 Assessment tools with sound psychometric properties, such as Non-Communicating Pain Checklist have been developed but lack clinical utility.11
Where possible, use well-established self-report and carer-report acute pain assessments such as FACES or r-FLACC that measure discernible pain expressed through facial and bodily signs. Although not specifically validated for use in children with CP, they are widely used and might have been used by the parents at home or during recent respite, before transfer.
Case scenario (continued)
The respite carer felt that, in retrospect, he was more unsettled than usual after the swollen left thigh was first noticed; he looked anxious and had had more dystonic episodes than usual.
Risk factors for fractures
Ask about any risk factors for fracture in this group (box 3).
Risk factors for fractures in children with cerebral palsy
Non-ambulatory status (Gross Motor Function Classification V).
Prior fracture(s).
Postoperative or postfracture immobilisation.
Joint contractures.
Vitamin D deficiency.
Gastrostomy feeds.*
Anti-epileptic drugs.*
*May reflect severity of condition rather than individual risk factors.
Case scenario (continued)
This 10-year-old has always been non-ambulant. This is his first fracture. He had recently been in a hip spica for immobilisation following surgery for subluxated hips. He has been gastrostomy fed since 2 years of age.
Children in GMFCS levels I–III (able to walk independently or with some assistance or mobility device) have a similar frequency and pattern of fractures to typically developing children. Thus, non-ambulant status is, in itself, a risk factor.12 The non-ambulant child is unable to participate in normal load-bearing activities that contribute to bone growth and density. Insufficient mechanical loading during childhood and adolescence results in inadequate periosteal bone apposition with reduced bone mass accrual, increased bone resorption and associated reductions in bone strength. These factors lead to the development of long, slender bones that have an increased propensity to fracture.1 This risk increases with age. The mean age at first fracture in two retrospective studies was 10 years and 8.6 years, respectively,2 3 as typified in our case.
Previous fracture is a risk factor for subsequent fractures, presumably due to bone loss associated with immobilisation.1 There was no history of fracture in our case but he had recently had immobilisation of the hip, both associated with increase in fracture risk.1
Feeding difficulties and undernutrition are common in children with CP, due to dysphagia, silent aspiration and gastro-oesphageal reflux.13 Gastrostomy feeds are associated with increased weight trajectory14 but not bone growth.15 Gastrostomy feeds and anticonvulsant use,3 particularly sodium valproate,2 have also been found to be risk factors for fracture in non-ambulant children with CP. However, the situation is complex; they may not be risk factors per se but proxy markers for severity of the underlying condition.16 Nevertheless, a full feeding and dietary history should be undertaken, in collaboration with the child’s dietitian and community nurse where possible. Although long-term protein-pump inhibitors are widely used to counter the symptoms of gastro-oesophageal reflux in CP, there is no evidence of increased fracture risk in children.17
Examination
Conduct a full clinical examination following detailed explanation and informed consent. Look particularly for clinical signs of undernutrition, joint stiffness and contractures, and external signs of injury around the fracture site and elsewhere. Inspect the mouth for dental erosions or signs of trauma.
Case scenario (continued)
Our patient looked thin but he was not pale and there was no clinical evidence of rickets. His teeth were normal. He had severe spasticity with lower limb joint contractures, particularly around the knees. His left leg was in traction and he did not appear to be in pain (Face 1 on Nursing FACES scale).
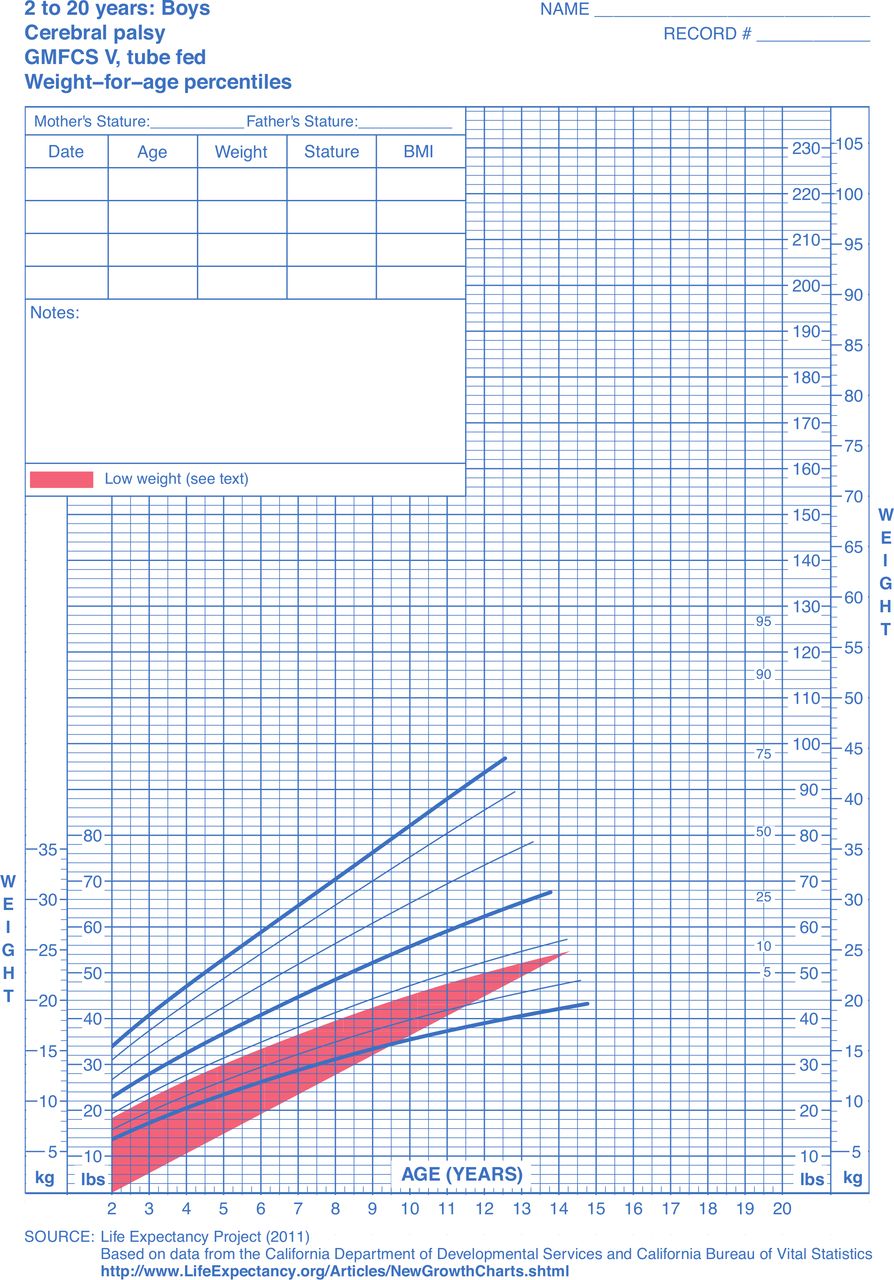
His weight (23.0 kg) was between the 0.4th and second centiles on standard weight charts but on the 25th centile on a specific weight-for-age chart for a male with GMFCS V CP. It was not possible to measure his recumbent length.
Anthropometric assessment
Even with careful clinical and nutritional monitoring, children with CP GMFCS V grow slowly for intrinsic reasons rather than poor intake.18 Specific growth charts for children and adolescents with CP were developed in the USA19 and validated against morbidity and mortality. These have also been validated for use on UK children.20 They are readily available (figure 2) and should be used to avoid potentially erroneous conclusions about the possibility of undernutrition and neglect, as there is a two-intercentile difference between his weight on the respective charts.
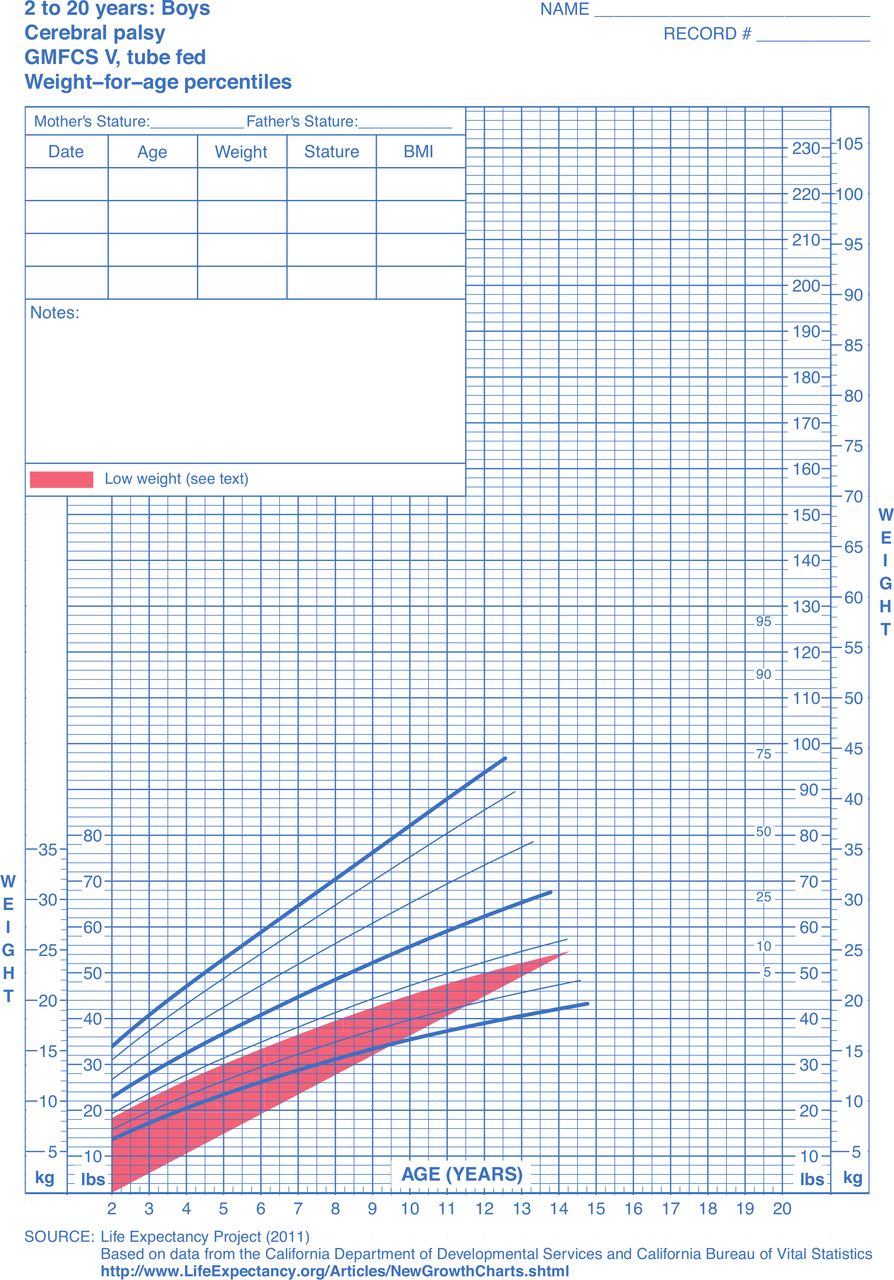
Weight-for-age charts for cerebral palsy GMFCS V – tube-fed males aged 2–20 years. GMFCS, Gross Motor Function Classification.
Recumbent length could not be measured due to inability to stand and joint contractures. Segmental measures such as upper arm length and tibial length can be undertaken in such situations and equated with linear growth using tables or charts.21 These measurements are challenging in a busy clinical environment but worth undertaking wherever possible.
Bruising
Case scenario (continued)
Our patient had three diffuse, ill-defined bruises in mid-lower back and one large, faded, linear bruise on the abdomen, just above the left iliac crest. There were no other bruises.
Take a full medication history and ask about any past or family history of excessive bleeding with haemostatic challenge. Check coagulation profile.
Bruising in these locations in a typically developing child, in the absence of a plausible explanation, raise concerns about possible inflicted injury.22 However, two studies23 24 have demonstrated that everyday bruising in children with neurodisability is different in location to that of typical children, occurring on the thighs, feet, hands, arms, abdomen and pelvis and back (lumbar region). Like typical children, they do not bruise over the ears, neck, chin, anterior chest, buttocks or genitalia, locations associated with inflicted bruising.25 The location of bruising, particularly in on-ambulant children, is predominantly related to equipment, transfers and wheelchair use.23
Investigations
Radiology
Case scenario (continued)
Plain film radiography of the left leg revealed an undisplaced fracture of the distal femur metadiaphysis. There was significant soft tissue swelling on the initial film and in a later film, shown in figure 3 , evidence of periosteal new bone formation tracking along the femoral shaft. Osteopenia was also evident.

{kind=link}
{kind=link}
{kind=link}
X-ray showing a healing fracture of the distal femur and osteopaenia.
Fractures in typically developing children occur mainly in the upper extremities.5 However, fractures in non-ambulant children with CP occur predominantly in the lower limbs, with a very high predilection for the distal femur and proximal tibia.1 Our patient had lower limb joint contractures, particularly around the knees. The immobilisation consequent on the stiff, flexed knees in such children contributes to the distal femoral location of fractures.16 Vertebral fractures have also been reported in non-ambulant children with CP.25
Studies have shown a strong inverse correlation between bone mineral density (BMD) of the distal femur and history of fracture.26 27 The X-rays show slender and ‘gracile’ long bones with a ‘washed out appearance’ of osteopenia,1 as shown in figure 3.
Discuss the estimated radiological time window for the fracture with a paediatric radiologist.
Although there is published guidance, the radiological timing of fractures in typically developing children is subjective and remains the province of experienced paediatric radiologists. Data on rates of bone healing in children with reduced BMD is lacking. Thus, dating fractures in the presence of osteopenia is even more challenging. The presence of the initial soft tissue swelling at the fracture site and later periosteal new bone formation may enable a paediatric radiologist to date the fracture within the time period that our patient first became symptomatic.
Other investigations
BMD may be reduced by up to 40% before it becomes evident on plain films.28 Measurement of BMD by dual-energy X-ray absorptiometry is very difficult in children with severe CP due to multiple contractures, scoliosis and pelvic obliquity. Assessment of BMD at the lateral distal femur is recommended in the latest paediatric position statement from the International Society of Clinical Densitometry.29 However, reference data for this site is only available for the Hologic Discovery scanner. Furthermore, this technique does not provide information about diaphyseal bone geometry that contributes to reduced bone strength in these children. If osteopaenia at the fracture site is not evident on plain film, discuss with a paediatric endocrinologist with expertise in bone health on the value of undertaking an assessment of BMD at the lateral distal femur.
Bloods for bone profile and vitamin D
The patient’s serum calcium, phosphate and magnesium were normal. The serum alkaline phosphatase was elevated in keeping with increased bone turnover. Some children on long-term sodium valproate develop a Fanconi-like tubulopathy with a low plasma phosphate.30
His serum vitamin D level was normal. Reduced vitamin D levels are associated with reduced BMD in CP patients and is therefore a risk factor for fractures in this group1 (box 1).
Safeguarding
Although the evidence for an association between disability and child maltreatment is weak,31 children with communication difficulties are more at risk.32 Thus, health professionals must be alert to this possibility when a child with severe, non-ambulant CP presents with a fracture.33 Our patient became symptomatic while in respite care, creating additional concern in terms of -positionof- trust.
Case scenario: safeguarding
Our patient had a fracture of the distal femur associated with osteopenia and three additional risk factors for an immobility fracture (box 1). The location of his bruising was normal for a child with non-ambulant CP. Although it was difficult to pinpoint the precise incident due to difficulties with pain perception, there was a change in his behaviour when the sign of fracture was first noticed, and this was within the radiological window of the fracture. There were no other safeguarding concerns.
On the basis of the evidence presented here, safeguarding and position-of-trust procedures are not indicated (figure 1), and the clinical team can move to consideration of fracture prevention by involving the metabolic bone team. (This is well reviewed by Fehlings and coworkers34 and will not be discussed here).
If the fracture remains unexplained, particularly in a vulnerable child, initiate safeguarding and position-of-trust procedures and take the actions outlined in box 1. Special school staff may also be the first to raise concern about a child with a possible immobility fracture, and therefore find themselves unwittingly involved in position-of-trust procedures. This decision pathway also applies to this scenario.
Other neurodisabilities
The decision pathway described for children with CP is also applicable to children with other forms of neurodisability, such as Duchenne muscular dystrophy (DMD), spinal muscular atrophy, spinal bifida and acquired brain injury, when found to have immobility fractures. Children with DMD are prone to fractures as a consequence of prolonged corticosteroids and progressive loss of mobility.35 36 In ambulant children, these are predominantly symptomatic, occurring after a minor fall, and involve both upper and lower extremities.37 In non-ambulant DMD children and adolescents, the fractures are predominantly extremity, although those using assisted walking devices (GMFCS IV) can sustain predominantly thoracic compression vertebral fractures even without long-term steroid exposure.26 This is also the case for children with myelomeningocele, spinal muscular atrophy and other inherited or acquired conditions associated with a motor deficit with GMFCS IV and V).26
Conclusion
Immobility fractures are relatively common, particularly in non-ambulant children with CP and also in other neurodisability conditions. However, they often occur in situations where safeguarding and position-of-trust concerns might arise. An evidence-based safeguarding decision pathway is described to guide health professions, particularly the lead clinician, in coming to a quick and reasonable decision that benefits both patient, carers and staff.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to thank members of the Safeguarding Team at Birmingham Women's and Children’s Hospital and Birmingham Children’s Trust for developing this safeguarding decision pathway.
References
Footnotes
Contributors All authors contributed to the conception and design of the manuscript following its commission. GD wrote the initial drafts and revisions, following input from the other authors. HM designed the Safeguarding Decision Pathway. NS provided expertise on aspects of osteopaenia and fracture risk and AO provided input on aspects of fracture morphology and fracture dating. All authors contributed to draft revision and agreed the final manuscript. GD assumes full accountability for all aspects of this commissioned work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.