Article Text

Abstract
Two previously well Caucasian teenage girls with no significant travel or family history were admitted with sinusitis refractory to treatment with antibiotics. Both had progressive symptoms despite broad-spectrum antibiotics and developed involvement of other systems, ultimately requiring admission to the paediatric intensive care unit (PICU). They were subsequently diagnosed with the same condition and made an excellent recovery.
The first girl, 14 years old, originally presented to her general practitioner with a sore throat, nasal congestion, and fever. Despite multiple courses of antibiotics over the following month she presented again multiple times with progressive symptoms including epistaxis, widespread myalgia and arthralgia, difficulty in breathing, haemoptysis, fatigue, and weight loss. Examination on admission found minimal discharge from her right tympanic membrane, ulcerated inferior turbinates with dried blood and yellow mucus in both nasal cavities, swollen tonsils without exudate, and an isolated aphthous ulcer on the tip of her tongue. She had small bilateral cervical lymph nodes. Examination of the cardiovascular system was unremarkable but on respiratory examination there was reduced air entry on the right side. Her abdomen was generally tender but soft with no organomegaly. A week into her admission she developed an oxygen requirement and increased work of breathing requiring intubation and ventilation.
The second girl, 13 years old, presented to her local hospital with a 1-day history of epistaxis, right ear pain, and pain and swelling to the right periorbital tissues. Again, despite multiple courses of antibiotics, she had persistent symptoms and subsequently developed fever, fatigue, haemoptysis, and had a syncopal episode. She was admitted to her local district general hospital and, despite initial treatment, deteriorated over the following 2 weeks with persistent fever, new oxygen requirement, deteriorating renal function, and anaemia. She was transferred to a tertiary centre for respiratory support which escalated from Optiflow, through continuous then biphasic positive airway pressure, intubation and ventilation, and ultimately VV-ECMO.
The investigations for both patients prior to admission to PICU at our centre are shown in table 1.
Questions
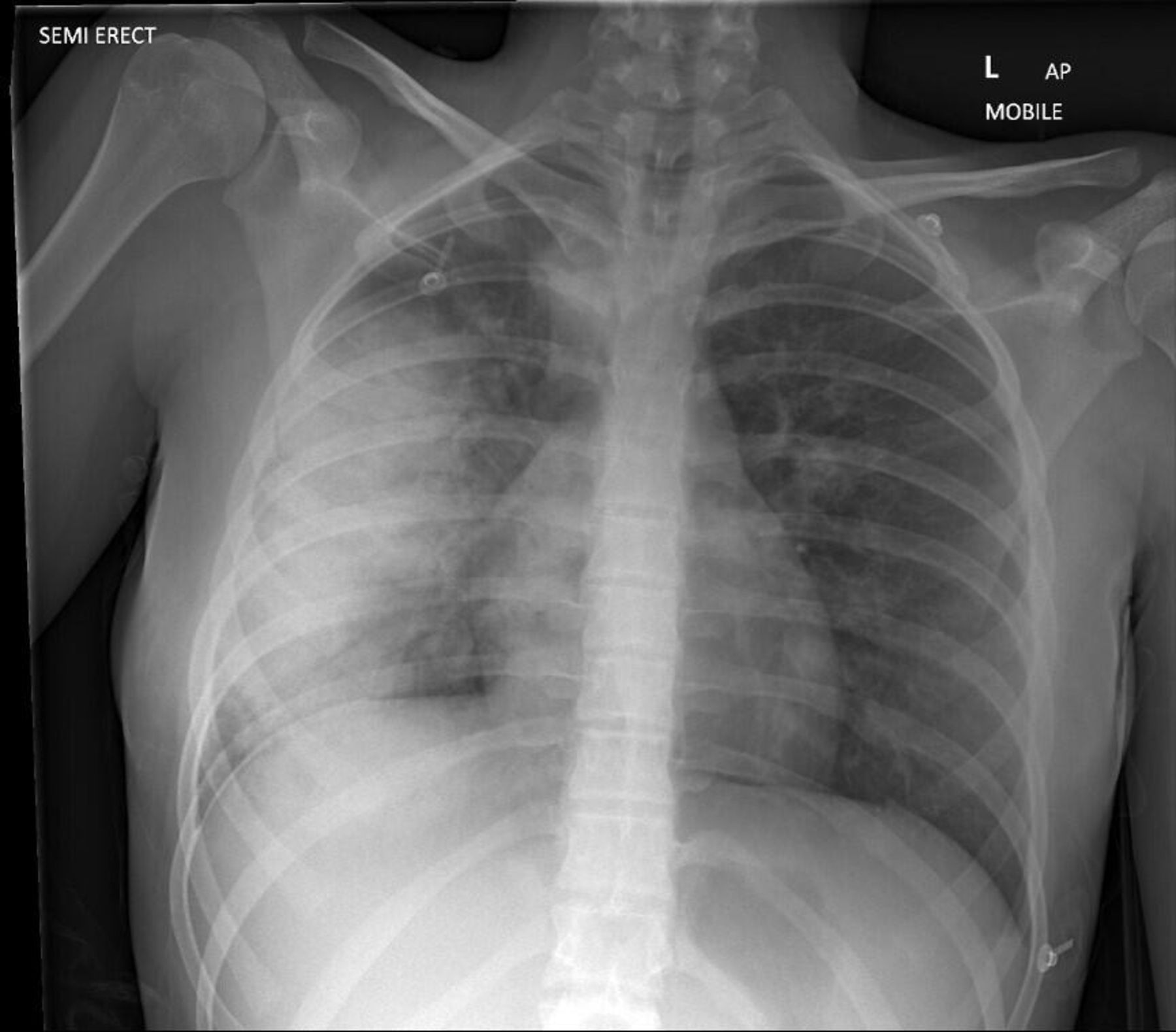
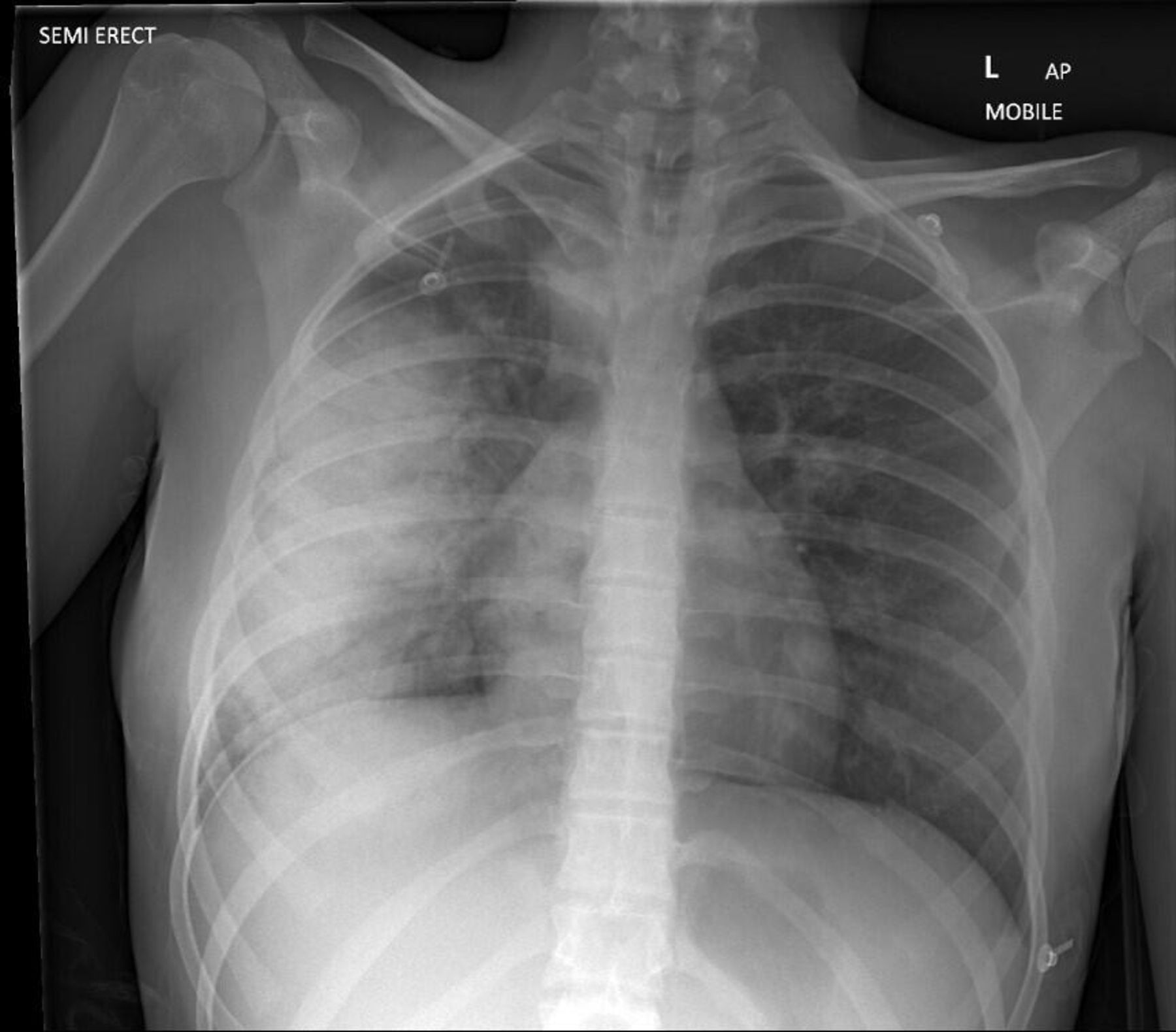
Describe findings in figures 1 and 2.
Which causes of sinusitis could explain the presentation of both cases?
Acute sinusitis following viral upper respiratory tract infection.
Bacterial infection.
Allergic sinusitis secondary to mould.
Underlying diagnosis of cystic fibrosis.
Sarcoidosis.
Tuberculosis.
Granulomatosis with polyangiitis.
Samter’s triad.
Ciliary dysfunction.
Immunodeficiency.
What investigations should be performed in a child presenting with symptoms of sinusitis?

{kind=link}
{kind=link}
QuestionsAnswers can be found on page XX.
- rheumatology
- nephrology
Statistics from Altmetric.com
Footnotes
Contributors This article was designed and written by JRB, with support and revisions from KS and VS, the senior author. Radiology images and interpretation were provided by RS. All authors have contributed to critical review of the manuscript, have approved the final version for publication and are accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.