Article Text

Abstract
The association between hyperlactataemia and poorer outcomes in acutely unwell adults and children is well recognised. Blood lactate testing has become readily available in acute settings and is considered a first-line investigation in international guidelines for the management of sepsis. However, while healthcare professionals do appreciate the value of measuring blood lactate in acute severe illness, its clinical significance and interpretation remain less well understood. In this paper, we present the evidence for the use of lactate as a diagnostic test and prognostic marker in acutely unwell children.
- biochemistry
- physiology
- neonatology
- resuscitation
Statistics from Altmetric.com
Background
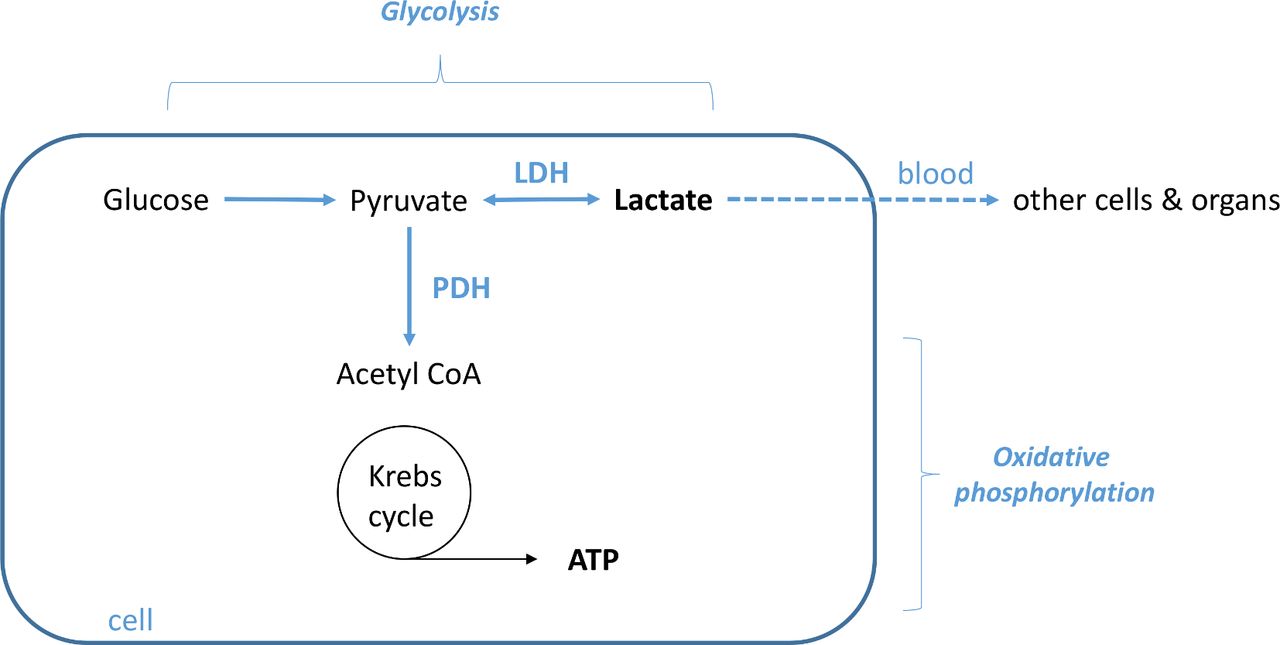
A widely held misconception is that lactate is a toxic waste product of metabolism, driven by hypoxia and/or hypoperfusion.1 It is now well established that increases in blood lactate due to hypoxia are likely the exception rather than the rule.1 At physiological pH, lactic acid (C3H5O3) is almost completely dissociated into lactate anions (La−) and protons (H+). In mitochondria, the process of glycolysis generates pyruvate from glucose. Pyruvate is converted to acetyl coenzyme A (Acetyl-CoA) by pyruvate dehydrogenase and enters the Krebs cycle to produce adenosine triphosphate (energy) (figure 1). The enzyme lactate dehydrogenase converts pyruvate to lactate, and, while the reaction goes both ways, the equilibrium is markedly in favour of lactate. Accelerated glycolysis (eg, in physiological stress) will always lead to an increase in lactate production, and lactate serves as a ‘reservoir’ supplying pyruvate to mitochondria. Lactate is shuttled within and between cells and organs where it is either oxidised to produce energy or converted back into glucose. Glucose can be stored as glycogen or released back into the circulation. Lactate itself is not toxic or harmful; indeed, there is some evidence that hyperlactataemia may be beneficial in some conditions, for example, traumatic brain injury and severe hypoglycaemia, and has a central role as a metabolic fuel.1 2
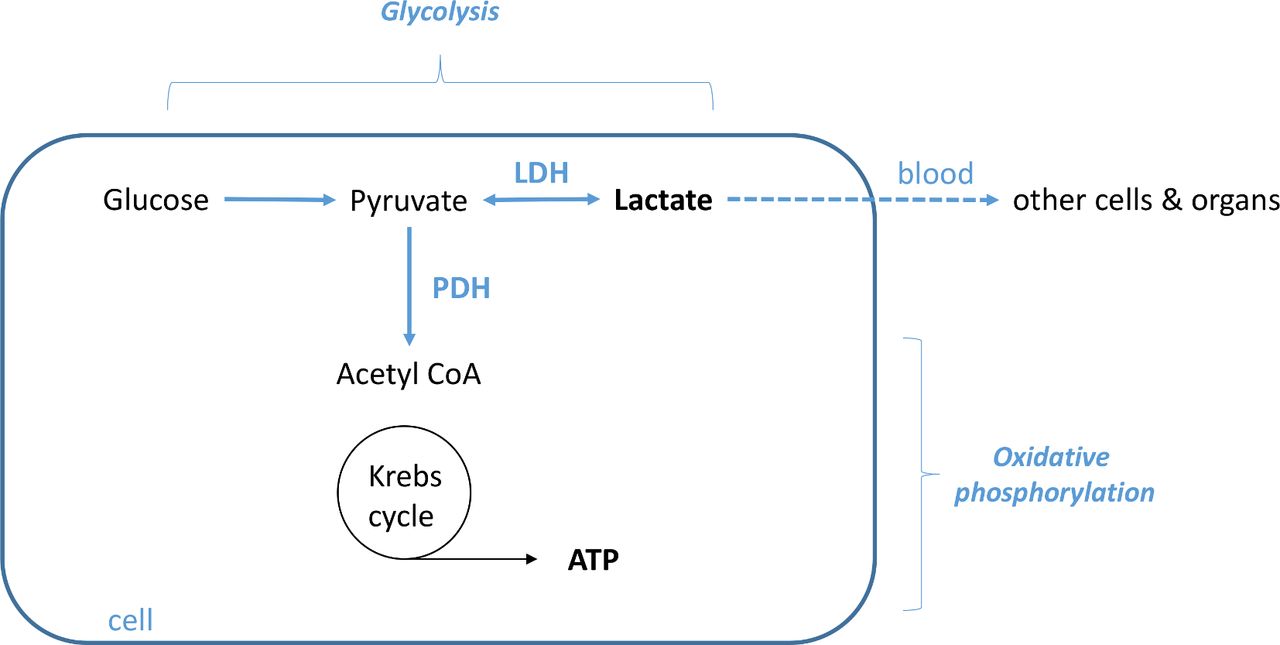
Lactate metabolism. LDH, lactate dehydrogenase; PDH, pyruvate dehydrogenase.
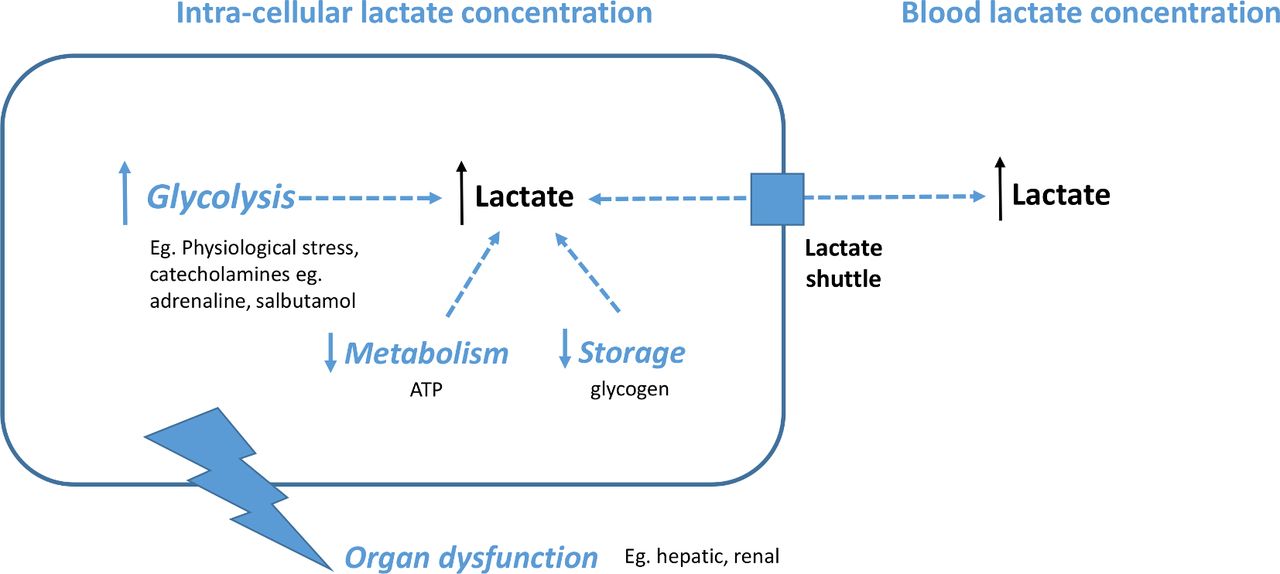
As for any metabolite, blood lactate concentration depends on the ratio between production and consumption.2 When elevated beyond baseline (0.3–1.8 mmol/L), it is most often a sign of altered energy homeostasis, but this may be a physiologically appropriate adaptive response (figure 2).
{kind=link}
{kind=link}
Elevated blood lactate concentration may be due to increased production, decreased consumption or changes in the balance of transport in and out of cells.
The term ‘lactate clearance’ is often employed to refer to a fall in blood lactate level; however, this is misleading since changes in lactate levels depend both on lactate production and metabolism.2
That hyperlactataemia is associated with hypoxia, ischaemia and acidosis confounds its clinical interpretation, and a normal level should not offer reassurance in the face of other clinical concerns.1 2
The assessment of hyperlactataemia in the context of inborn errors of metabolism is beyond the scope of this article; suggested resources are provided in box 1.
Inborn errors of metabolism—online resources
Vademecum Metabolicum (Assessment and Treatment of Inborn Errors of Metabolism): http://www.vademetab.org/
British Inherited Metabolic Diseases Group (BIMDG) Emergency Guidelines: http://www.bimdg.org.uk/guidelines/
Technological background
Sampling
A venous blood lactate concentration of <2 mmol/L is predictive of a (gold standard) arterial blood lactate of <2 mmol/L, but above this level an arterial sample is most reliable.3 Capillary blood lactate measured on heel-prick samples has been shown to correlate with arterial blood lactate in both preterm and term neonates.4 Though capillary blood gases are used extensively in paediatrics, there is insufficient evidence showing a correlation between capillary and either venous or arterial blood samples in children, and in adults, capillary lactate in acute illness has been shown to correlate poorly with venous lactate.5
Analysing
Blood lactate can be measured by point-of-care-testing (POCT) devices (using whole blood) or in the laboratory (on plasma). POCT requires smaller samples, can be performed on user-friendly instruments by staff without laboratory training, provides a rapid turnaround time for results and facilitates increased frequency of testing.6 Although there is generally a strong correlation between methods across the range of lactate values, at higher lactate concentrations POCT may be less reliable.7
Clinical cases
In children with suspected sepsis does a raised blood lactate at presentation predict mortality?
Hyperlactataemia is correlated with increased mortality in studies of children and adults with sepsis; however, its definition (from 2 to 5 mmol/L) and sampling timeframe (eg, initial lactate, peak lactate and/or duration of hyperlactataemia) varies.8
Evidence for the accuracy of initial blood lactate in predicting mortality in children with sepsis is provided by several cohort studies; however, there is significant variation in patient populations and lactate thresholds (table 1). These studies demonstrate a large variation in mortality rates (from 1.9% in presentations to a USA emergency department (ED) to 63.5% for undifferentiated paediatric intensive care unit (PICU) admissions in India), clearly representing significantly different populations.9–13
Diagnostic accuracy of initial blood lactate in predicting mortality in children with sepsis/suspected sepsis*
In a large observational cohort study of 1299 children with suspected sepsis presenting to a US ED,9 those with initial lactate >4 mmol/L had higher 30-day mortality (4.8% vs 1.7%). However, it is important to note that, in this patient group with a low mortality overall (1.9%), 80% (20/25) of all deaths were in children with initial lactate <4 mmol/L and >95% patients with lactate >4 mmol/L survived, yielding a sensitivity of only 20%. In a large study of children admitted to PICUs in Australia and New Zealand with sepsis and/or septic shock (n=1697), mortality was independently correlated with lactate on presentation to ICU, with the highest mortality in children with hypotension requiring vasopressors and lactate >2 mmol/L (32% vs 7.7% in the hypotensive non-vasopressor group with lactate <2 mmol/L).14
The recently published Surviving Sepsis Campaign (SSC) International Guidelines for the management of septic shock and sepsis-associated organ dysfunction in children, states: “we were unable to issue a recommendation about using blood lactate values to stratify children with suspected septic shock or other sepsis-associated organ dysfunction” and that levels should “be interpreted as part of a more comprehensive assessment of clinical status and perfusion”8 (see online supplementary infographic: decision-tree).
Supplemental material
In children with suspected sepsis, does lowering lactate levels improve outcomes?
In adults with septic shock, there is some evidence that lactate-guided resuscitation reduces mortality though these findings remain under debate.1
In children, evidence for lactate as a therapeutic target is limited to observational studies10–12 15 table 2.
Association between persistent hyperlactataemia and mortality*
In a cohort of 77 children presenting to a USA ED with suspected sepsis, those whose lactate normalised within 2 to 4 hours of presentation had decreased risk of organ dysfunction at 48 hours (RR 0.46, 0.29–0.73).16
In a study of Ugandan children admitted to hospital with pneumonia with lactate >2.5 mmol/L, mortality was increased in those whose levels remained >40% baseline by 8 hours (32% vs 11%, p=0.046).10
Persistent hyperlactataemia may be more predictive of mortality than raised admission lactate. In a study of 700 medical PICU admissions,17 persistent hyperlactataemia (>2 mmol/L) at 24 hours was associated with 93% mortality versus 30% in children whose lactate levels normalised (sensitivity 78%, specificity 89%, LR+ 7, LR− 0.25); this compared with 64% mortality in children with admission hyperlactataemia versus 6% in children without. Two studies address persistent hyperlactataemia at 24 hours in children with septic shock admitted to PICUs in India: Choudhary et al (n=148) observed that lactate levels falling <10% were associated with 83.1% (74/89) mortality versus 33.9% (20/59) in children whose lactate normalised more rapidly12; Nazir et al reported that children whose lactate failed to fall by >20% at 24 hours had 100% (28/28) 60-day mortality versus 8.3% (7/84) in those whose lactate reduced by >20%.15 This association was evident even at 6 hours: mortality 83.3% versus 17.05% (sensitivity 94.8%, specificity 57.1%, LR+ 2.21, LR− 0.091).
It is important to note that, since these studies are observational and not interventional, there is currently insufficient evidence to support the use of lactate as a therapeutic target in paediatric sepsis. However, there is an association between persistent hyperlactataemia and mortality and morbidity, so failure of lactate levels to normalise is likely to be a valuable indicator of disease severity.
SSC guidelines suggest—as a weak recommendation, with very low quality of evidence—“using trends in blood lactate levels, in addition to clinical assessment, to guide resuscitation” and note that “a persistent elevation in blood lactate may indicate incomplete haemodynamic resuscitation and should prompt efforts, as needed, to further promote hemodynamic stability”.8
In neonates in neonatal intensive care, do lactate levels on day 1 of life predict morbidity and/or mortality?
Hyperlactataemia in the neonatal period may represent an acute insult or underlying disease such as inborn error of metabolism.
In suspected neonatal hypoxic ischaemic encephalopathy (HIE), there is an association with hyperlactataemia as a marker of secondary energy failure. In a retrospective study of 61 term neonates, a plasma lactate >7.5 mmol/L within 1 hour of life was associated with moderate or severe HIE—sensitivity 94% (PPV 55%) and specificity 67% (NPV 97%).18
A study of admission and peak lactate in the first 12 hours of life in low birthweight and preterm neonates (n=381) reported an association between hyperlactataemia and in-hospital mortality, which was also independently associated with abnormal cranial ultrasound scans, bronchopulmonary dysplasia and retinopathy of prematurity.19
In neonates requiring extracorporeal membrane oxygenation (mainly for respiratory pathology such as meconium aspiration, congenital diaphragmatic hernia and persistent pulmonary hypertension), a prospective study (n=74) found admission, 12 hours and peak lactate levels were significantly higher in non-survivors, but only peak levels (>15 mmol/L) were associated with poorer neurodevelopmental outcome at 2 years.20
In neonates with suspected necrotising enterocolitis (NEC), is lactate useful as a diagnostic or prognostic marker?
A small retrospective study (n=24) evaluated the prognostic value of perioperative measurement of blood lactate levels for neonates undergoing surgery for NEC; those with lactate >1.6 mmol/L were more likely to develop complications such as strictures and death.21 Serial changes in lactate are better predictors of progression in confirmed NEC. A cohort study (n=37) comparing lactate level changes from baseline over 48 hours in preterm neonates with medical and surgical management of NEC showed that a rise from baseline at 72 hours was associated with progression to surgical intervention or mortality (area under the curve (AUC) 0.82, p=0.047), though in this group, a rise in C reactive protein showed a stronger association (AUC 0.93, p=0.001).22
Despite a widely held belief by clinicians that an increased lactate level is associated with an increased likelihood of NEC,23 there is currently insufficient evidence to support the use of lactate as a diagnostic marker for the disease.
Clinical bottom line
Lactate is an important molecule with complex biological functions—it is not a simple marker of hypoxia or a waste product of metabolism.
Elevated lactate levels indicate a metabolic imbalance between production, consumption and cellular transport.
A normal lactate at presentation does not rule out severe sepsis or septic shock and should not be considered reassuring in the presence of adverse clinical signs.
In sepsis, a high blood lactate at presentation should prompt careful monitoring, as persistent hyperlactataemia is associated with organ dysfunction and mortality.
Elevated lactate does not assist in the diagnosis of necrotising enterocolitis (NEC), but in neonates with confirmed NEC, hyperlactataemia is associated with poorer outcomes.
Acknowledgments
Drs A Arumburo, H F Scott and NP Boeddha for providing clarifying information.
References
Footnotes
Twitter @MDMarikar, @docpbabu, @finegoulden
Contributors DM and PB: initial manuscript draft. MF-G, DM and PB: manuscript revisions. PB and MF-G produced the figures and DM the infographic. DM produced statistical summary tables. This is an update of an article originally published in ADCE&P by MF-G in 2014.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.