Article Text

Abstract
A 12-month-old infant was referred with a 6-week history of recurrent admissions with worsening stridor. On each previous admission, the stridor responded well, but transiently, to oral dexamethasone. At this presentation, he required high-dependency unit care with high flow oxygen due to marked increased work of breathing.
He was born at term, previously well, and up to date with immunisations. There was no significant family history. There were no smokers and two cats at home.
He was afebrile with moderate subcostal recession and tracheal tug. On auscultation, breath sounds were normal with transmitted sounds of inspiratory and expiratory stridor. The rest of his examination was normal.
He commenced dexamethasone 0.15 μg/kg three times a day, which was weaned as his clinical status improved.
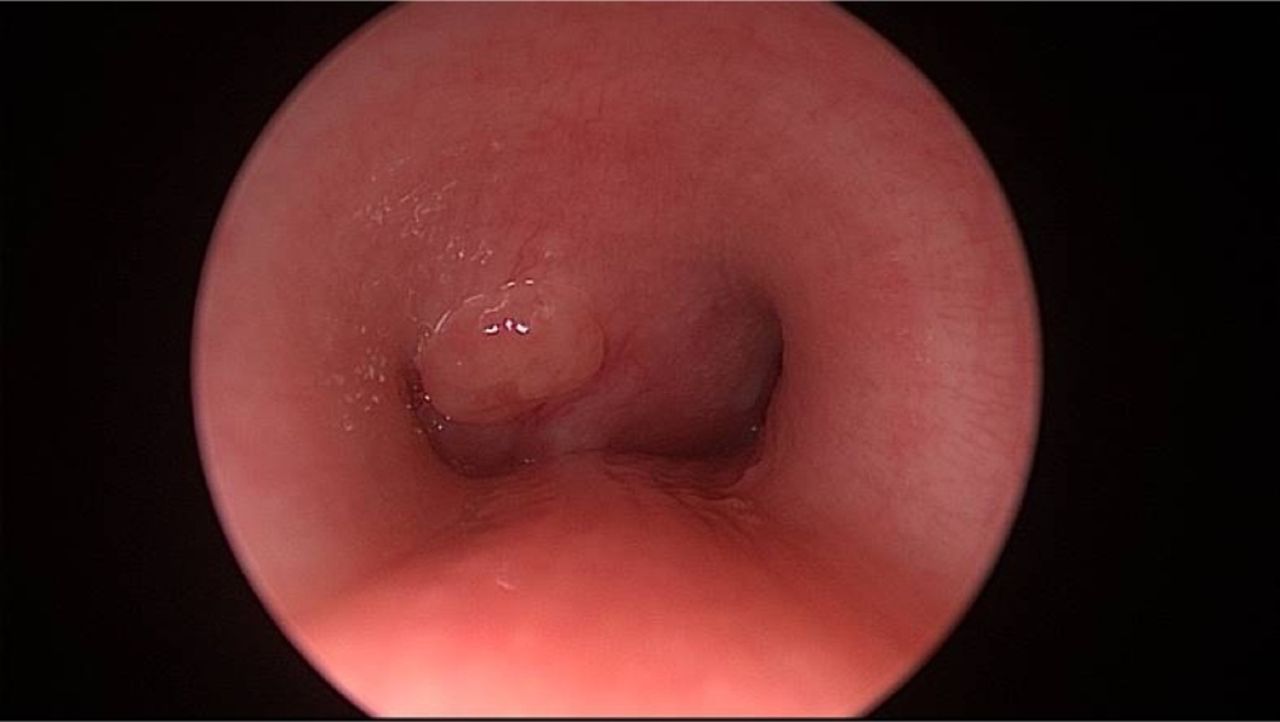
Blood tests showed total white cell count 9 x 10ˆ9/L, CRP <1 mg/L, lactate dehydrogenase level and blood film normal. Chest radiograph showed left lung hyperexpansion and apparent right-sided bronchial narrowing (figure 1). Flexible nasendoscopy was unremarkable. Microlaryngoscopy and bronchoscopy showed external airway compression at the level of the carina (figure 2). CT thorax demonstrated a non-enhancing mediastinal mass extrinsic to the airway, approximately 3cmx2.5cmx1.5cm, compressing the carina and main-stem bronchi (figure 3).

Chest radiograph showing left lung hyperexpansion and apparent right-sided bronchial narrowing (arrow).
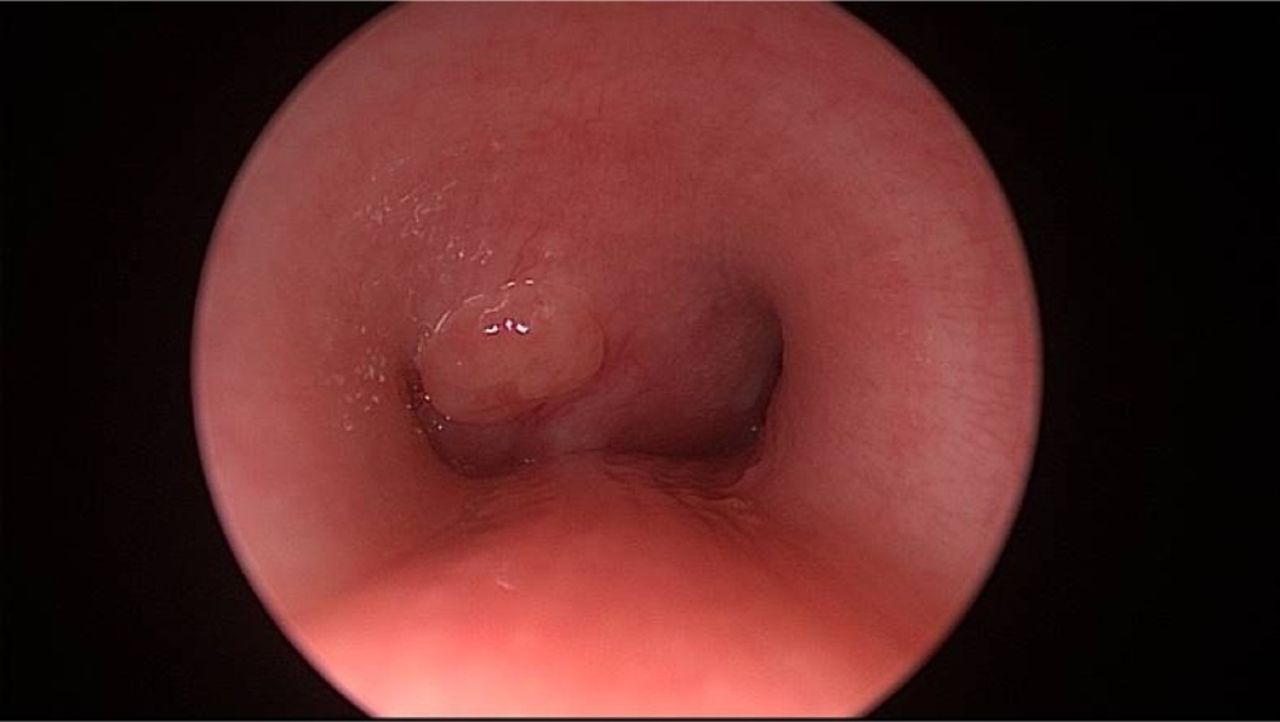
Rigid bronchoscopy image showing external airway compression at the level of the carina. Incidental finding of small mucosal lesion—felt to be making no contribution to critical airway narrowing.

{kind=link}
{kind=link}
{kind=link}
Contrast axial CT image with lung windowing which shows a large subcarinal soft tissue density mass (arrow) flattening and splaying both proximal bronchi into a crescentic appearance. Reflux of contrast to the azygos vein is seen at the right lateral aspect.
Question 1 Please list four differentials for this child's mediastinal mass.
Question 2 Which of these approaches would be suitable at this stage?
CT-guided biopsy
Bronchoscopic biopsy
Excision biopsy
Watch and wait and monitor response to steroids
Question 3 What is first line treatment for Mycobacterium avium complex lymphadenitis?
Complete excision
Clarithromycin and complete excision
Clarithromycin, rifampicin, ethambutol and complete excision
Isoniazid, rifampicin, pyrazinamide and ethambutol and complete excision
Answers can be found on page 2.
- general paediatrics
- imaging
- infectious diseases
- respiratory
- ENT