Article Text

Abstract
Journal club is a long-standing pedagogy within clinical practice and education. While journal clubs throughout the world traditionally follow an established format, new approaches have emerged in recent times, including learner-centred and digital approaches. Key factors to journal club success include an awareness of the learning goals of the target audience, judicious article selection and emphasis on promoting the engagement of participant learners. This article reviews the role that journal club plays in modern clinical education and considers how to optimise its benefit for contemporary learners.
- journal club
- evidence-based medicine
- critical appraisal
- twitter journal club
- learner-centred
Statistics from Altmetric.com
Introduction
History synopsis
Journal clubs (JCs) remain a steadfast pedagogy within contemporary postgraduate clinical education. Since their inception, JCs have shared a common objective to create an environment where people with a shared professional interest can meet periodically to focus on interesting or topical medical research literature. The concept of a JC has been in existence for a lot longer than one may imagine. In the mid-1800s, Sir James Paget set up ‘a kind of club…where we could sit and read the journals’ at St Bartholomew’s Hospital in London.1–3 Sir William Osler led similar clubs during his time at McGill University in Montreal ‘for the purchase and distribution of periodicals to which he could ill afford to subscribe’.4 In 1889, Osler established the first formal ‘journal club’ at Johns Hopkins University in Baltimore.2 These early incarnations of JC may have represented rare opportunities for doctors to collaboratively discuss patient care in an era predating the widely available clinical guidelines, consensus statements, and web-based clinical decision resources that we have today.
Why have a JC?
Core intended goals and learning outcomes of modern-day JCs are outlined in box 1. While several of these may have pertained to JCs of the past, the functions of modern-day JCs have evolved to reflect our rapidly changing sociotechnical clinical landscapes, serving to enhance contemporary clinical education and communication networks.5 6 For example, the multitude of instantaneously available (online or otherwise) clinical information resources means that healthcare professionals no longer depend on JCs to inform best practice. Today, JCs are more often used as a forum for collective critical appraisal of published literature, as a method to enhance evidence-based learning, or as a way of keeping abreast of relevant published research.7 We consider the contemporary JC as a valuable, multidimensional educational intervention for clinicians and clinical educators alike.
Proposed functions of contemporary journal clubs
Teaches critical appraisal of research design, biostatistics, and evidence quality.9 28 29
Promotes evidence-based practice.29 30
Encourages lifelong learning.15
Develops leadership and presentation skills.28
Promotes mentorship and collaborative learning.12
Disseminates new medical developments.12
Broadens professional local and international networks.31 32
Inspires new research studies.
JC format
The classic format
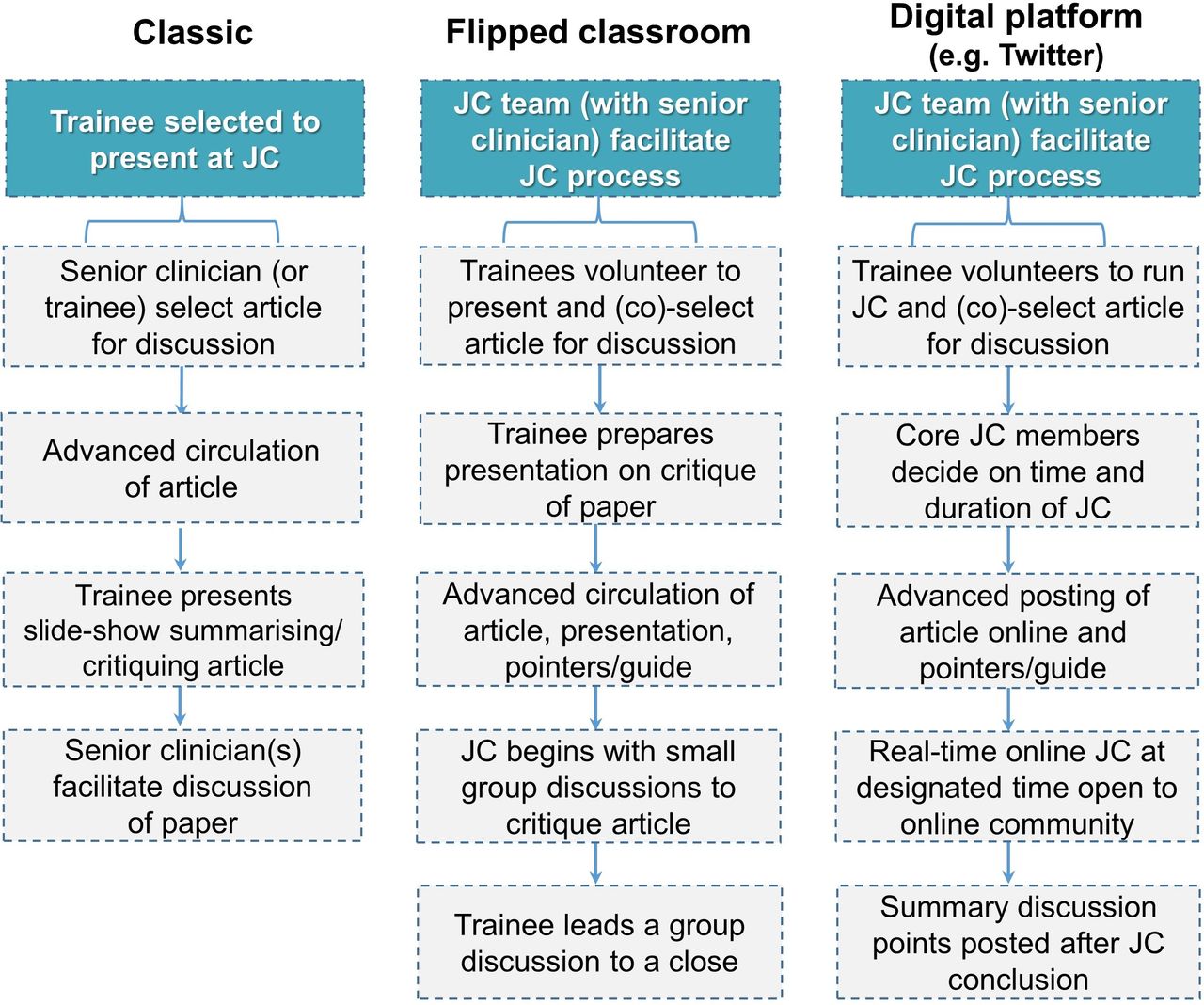
The traditional or classic JC format (figure 1) in its most stereotypical form usually occurs face-to-face. Peer-reviewed journal articles of interest are presented by a junior trainee, followed by discussions often led by the more senior members of the clinical hierarchy in attendance. This, or a similar process, is reproduced in many institutions all over the world. It confers distinct educational benefits, including improved critical thinking skills, increased knowledge of research design and enhanced research awareness.8 9 However, the stereotypical format described may have potential pitfalls (which could be, and indeed are, optimised in some institutions) as applied to a contemporary clinical environment. For example, a JC based around a didactic presentation runs the risk of attendees becoming passive listeners.6 JCs led and facilitated by senior clinicians may result in discussions dominated by those with more experienced viewpoints. Face-to-face meetings that adhere to rigid schedules do not suit healthcare professionals who work different shift patterns or who are geographically isolated.10 11
{kind=link}
Examples of journal club (JC) formats. In practice, elements of the classic format can be incorporated into other formats, resulting in multiple potential hybrid approaches to JC that follow the guiding principles of JC design (box 2) and that address the key issues important to consider when setting up a new JC (box 3).
Modern approaches to a classic format
JC has a lot to offer contemporary learners as a medical pedagogy.8 12 13 Educational researchers view the potential of JC through the lens of educational theories that emphasise social learning, communities of practice and distributed leadership.14 The central premise of the JC format can be built on to reflect the principles of contemporary clinical education approaches, which value collaboration, participation and learner engagement (figure 1; box 2).14 15 Although JC design can be approached in a multitude of ways depending on the educational, institutional or departmental context, we consider more recent complementary approaches below, which may promote deeper learning and a wider reach for participants.
Guiding principles of journal club design
Guarantee both reputational safety and a challenging educational experience.
Foster a safe learning environment, in which all participants can articulate areas of uncertainty, ask ‘low level’ questions, and share personal perspectives without fear of ridicule or censure.
Balance learner/trainee autonomy against the learning needs of senior faculty.
Allow learner/trainees the autonomy to develop their own learning experiences while also maintaining senior presence to facilitate and inform sessions.
Customise educational design to the needs and requirements of the target group of learners.
Exploit emerging communication technologies in order to enhance the reach, generalisability and effectiveness of the journal club experience.
Learner-centred approach
JCs are more effective if they have a leader, but this leader must be chosen carefully.8 It is a fine balance between selecting an expert facilitator who could potentially dominate the discussion and choosing a junior learner who may not have the requisite understanding of the material to engagingly facilitate the session. However, nominating a mentor to guide juniors in selecting their own article and leading on its discussion facilitates a learner-centred experience that promotes engagement and gives ownership of the process to the learners.9 15 This requires advanced planning, enthusiasm of both supervisors and trainees and possibly a forum for regular, informal discussion between the junior and mentor to ensure that the JC meetings do not become stale.1
‘Flipped classroom’ approach
A flipped classroom approach to JC involves circulating the article for discussion in advance, along with preparatory reading work.6 Ensuring pre-session engagement represents a specific challenge. Video or online interactive tutorials can facilitate this process.16 Distributing an appraisal tool along with the reading material may also help. For example, the Critical Appraisal Skills Programme (CASP) tools are freely available online and can aid JC attendees in the appraisal of randomised controlled trials as well as other relevant study designs (eg, case–control studies, cohort studies, qualitative research, etc).17
When successful, flipped classroom approaches translate to less time spent didactically presenting information and more time for collaborative discussion and questions. Often, this approach involves small group discussions, perhaps after a brief overview of the material at the outset. Small group discussions create an environment that encourages participants who otherwise may have been intimidated to step up and contribute. They also may help less knowledgeable attendees learn from the more experienced members of the group.18 Small group approaches also help to break up the ingrained physical layout of a room; chairs laid out in rows are instead placed in circles and trainees who previously congregated down the back of the room are now dispersed within it. These changes alone may break down hierarchical boundaries that impede learning.
Digital platforms
The advent of digital technology has revolutionised the way healthcare professionals communicate with one another. Online platforms and social media tools now make it possible to traverse national and international boundaries.19 Not surprisingly, a number of virtual JCs have emerged in recent years, starting first with online discussion boards, e-conferences and medical blogs.20 The virtual journal club then shifted to social media platforms, with the first interactive Twitter journal club established in 2011 and an eruption of Twitter journal clubs since that span multiple specialities.5 21 For example, the first paediatric Twitter journal club, @ADC_JC, was established in 2013 by Archives of Disease in Childhood and is still going strong today. Digital JCs are clearly popular and have the potential to spark discussion, disseminate best practice more widely and automatically result in an archived database of previous JC reviews. However, can the online JC learning experience emulate fully the socially constructed learning and knowledge gained from face-to-face interactions?
The most important consideration when developing any contemporary approach to JC is to ensure that its essential elements that have survived for decades are preserved while also harnessing digital connectivity and new educational approaches to our advantage, applicable locally or with wider reach. Some of the potential advantages and drawbacks to digital JC approaches are outlined in table 1.
Journal club on digital platforms
Setting up a journal club
In words of one of the first JC proponents, Sir William Osler: ‘The very first step towards success in any occupation is to become interested in it’. While the various modern approaches to JC have a lot to offer contemporary learners as medical pedagogies, several key considerations must be addressed when setting up a new journal club in order to optimise its delivery and effectiveness (box 3).
Optimising the journal club experience—key considerations
Identify your learners—What are their clinical and academic backgrounds?
Ascertain the objective of your journal club (JC)—What do your learners want to learn? Why?
Selecting an article—What article types or concepts will spark discussion to achieve objective? Critical appraisal curriculum (see table 2)?
Develop JC structure that best suits your learners—A classic, face-to-face JC? A virtual learning experience? Flipped classroom approach? Adapt hybrid model/aspects of each?
Decide the practicalities
How often will your JC meet, and where and when?
Access to resource material (presentations, literature, eg, deposited in Dropbox, accessible computer drive, email). Can information services/librarian assist?
Appraisal tools (why, which, how will it help?).
Decide how to promote JC engagement—What will your learners best respond to?
Free food? Mandatory attendance? Continuing medical education points/portfolio requirements?
A learning experience facilitated and led by trainees?
Seniors willing to provide feedback (eg, presentation skills, JC delivery and evolution)?
Develop JC resource, for example, available material from previous good JCs and good quality material related to critical appraisal education/techniques (eg, websites, articles, books, prior presentations).
For digital platform JCs (eg, Twitter) consider:
Clinical Journal club material
Consider who your learners are
Creating a JC from scratch represents an opportunity to design a JC that best suits its learners. A key starting point is carefully considering the individual and collective needs of the attendees, taking into account their career goals and varying clinical and academic experience and mapping learning outcomes accordingly.22 Hospital-based JCs often focus on developing critical appraisal skills, enhancing evidence-based practice and understanding the hierarchy of evidence. Therefore, many JCs in turn reflect ‘Evidence-Based Medicine’ curricula.23 In choosing articles, generally those published in high impact journals that are recent, paradigm changing and have the potential to influence clinical practice make for the bulk of good JC discussion material.
Just as every clinical question, research question or discovery cannot be answered by studies outlined in the typical ‘Evidence Pyramid’ and critical appraisal thereof, JC material may vary depending on context or even week. JCs still help to keep teams and individuals up to speed with topical and important research themes and, for example, material may also include case descriptions, qualitative research, clinical practice guidelines and review articles of major importance (table 2).24 Attendees involved in academia and scientific research may also be interested in translational research approaches. Occasional reviews of recent conferences or discussions around the evidence base for alternative or even controversial approaches in medicine may also appeal to attendees. While attendees ‘rotating through’ general paediatrics and its subspecialties may find these former approaches most relevant, medical JCs also represent an excellent opportunity for interprofessional education and learning, and so can be attended by and tailored towards multidisciplinary professionals.25
Encouraging attendance and engagement
The first step in creating a sustainable, effective JC that engages a learner group is to identify a core team to assist with the design process. This team should consist of genuinely enthusiastic, engaged junior learners and senior clinicians who are willing to act as facilitators of the JC process.8 14 This team can then consider the key ingredients relevant to the learning contexts of their JC group.
The optimal size of journal club has yet to be determined, though at least eight attendees has been suggested for JCs at departmental level. The optimal execution of larger (eg, hospital-wide critical appraisal rounds) may differ, for example, more or less formal boundaries, participant and attendee roles, depending on group size.22 26 Provision of food has been debated and has been associated with increased attendance.8 Mandatory attendance has also been suggested to promote attendance, as has using JC to fulfil continuing medical education or ‘e-portfolio’ requirements. However, being physically present does not equal engagement,8 27 and while these incentives are useful to consider, the emphasis should be placed on actively engaging the target audience so that they realise there is something of value to be learnt during the sessions.
Conclusion
JCs remain a potentially powerful pedagogy within postgraduate clinical education in an era of abundant and instantly available clinical information resources. A JC based on several guiding principles will help ensure that learners engage with and attend JC for the sake of learning. Key to JC success include:
Considering who the learners are and what they wish to learn.
Ensuring that learning is social, collaborative, and not hampered by hierarchical boundaries.
Combining key elements of the classic JC format with new educational approaches to suit the needs of contemporary learners.
Harnessing the advantages of digital connectivity.
What this study adds
What is already known on this topic
Journal club is a long-established pedagogy within clinical education.
What this article adds
New approaches and formats to group learning have emerged in recent years in response to the changing educational and workplace environments and cultures. Modern technology has allowed journal club to be adapted to continue to play an important role in contemporary clinical education for today’s learners.
References
Footnotes
SMM-B and MO are joint first authors.
Contributors SMB and MOR acquired, analysed and interpreted data for this study (literature review), drafted the article, co-wrote the article and wrote and revised subsequent drafts of the article. PC contributed to the content of the article, critically reviewed the article for important intellectual content and edited the article. NA conceptualised the study, supervised the study, contributed to the article, critically reviewed the article for important intellectual content and edited the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Hospital ethics approval was not requested due to study design.
Provenance and peer review Not commissioned; externally peer reviewed.