Article Text

Abstract
Burns are a relatively common injury in children accounting for over 50 000 emergency department attendances each year. An estimated 1 in 10 of these are due to maltreatment. These may present in the form of physical abuse or neglect with a reported ratio of 1:9. A burn associated with maltreatment may be a marker for future abuse or neglect and it is paramount that concerns are identified and addressed at the initial visit. Paediatricians need to be confident to identify safeguarding concerns specific to childhood burns and investigate accordingly. In this review, key variables that may aid in differentiating maltreatment from accidental burns are discussed in a case-based format, utilising up-to-date evidence to support the recommendations. Despite a proportion of burns resulting from physical abuse, the rate of child protection investigations in these patients are significantly lower than for children who present with other forms of physical injuries despite a similar proportion of positive findings. Our objective is to review the available evidence to support the safe assessment and management of children presenting with scalds or contact burns.
- child abuse
- burns
- general paediatrics
- dermatology
Statistics from Altmetric.com
Introduction
While we are aware of the literature regarding physical abuse in the form of bruising and fractures, an area that can potentially be missed is the role child safeguarding plays in childhood burns. A burn is painful and distressing injury, enhancing the possibility of focusing solely on the physiology and failing to appreciate the wider safeguarding concerns.
The aim of this article is to review the literature on this topic.
Case
You are on-call for general paediatrics in a busy district general hospital and are contacted by the emergency department (ED). They have an 11-month-old with a burn and have some safeguarding concerns.
On the long walk down, you do a quick literature search on the safeguarding considerations with childhood burns.
Background
There is good epidemiological data on childhood burns in the UK with approximately 50 000 children attending ED each year with a burn.1 2 It is estimated that 10% of these are a result of maltreatment with the actual reported figure varying with geographical location.3 In the UK estimates of 1%–16% are quoted and the US data estimates between 3% and 26%.4–6 Experts agree that the actual number is much higher.
Maltreatment in the case of burn injuries manifests in the form of neglect or physical abuse with the ratio of neglect to abuse 9:1.7 As clinicians, we are all too aware of the importance of identifying child protection concerns early recognising that child abuse is an on-going process and not a solitary event.
Burns can be viewed as a marker for future maltreatment. The literatures identifies that if a child suffers a burn before the age of three, by their sixth birthday they are seven times more likely to suffer abuse or neglect and twice as likely to be a ‘child in need’ compared with a matched cohort.8
Case
You further discuss the case with the ED team. The injury is reported to have occurred 2 days ago with no clear history. It is a deep partial thickness burn on both arms and legs, estimated at 2%–3% total body surface area (TBSA).
You consider what in the history and examination can help you differentiate accidental burns from maltreatment burns (inflicted and neglect).
History
A vague or changing history, an injury that does not fit with the history provided or a speculative account of an unwitnessed burn are potentially significant points for abusive burns and scalds. The blame of a sibling or a trigger event (family stress, persistently crying infant) also pose a higher risk for abuse.9 As with all paediatric injuries, the reported mechanism must be compatible with the developmental age of the child (figure 1).

Features in history and examination that may be suggestive of maltreatment (neglect or physical abuse) in children with a burn.
Burns are a common cause of ED attendances, particularly in the under 5s. It is also these children who are most vulnerable with regard to abusive thermal injuries with abuse more likely in the younger patient.10
Socially, the presence of risk factors such as domestic violence and abuse, drug and alcohol misuse and severe mental health concerns in the carers, concern regarding level of supervision or the involvement of an active social worker for any reason, increase the potential for concern.11 Likewise, a history of multiple previous attendances for injuries or previous burns may be indicative of neglect or repeated physical abuse and further clarification should be sought.11
A delay in seeking treatment may be an indication of child maltreatment but in burn injuries, the rationale for delay can be more complex. The lack of pain in full thickness burns and the evolution of a burn from a superficial to deeper injury over time may account for some parents or carers delaying seeking medical advice.
There is some evidence to suggest that certain reported mechanisms may be more likely attributed to child maltreatment. One study found abuse was more likely if bathing (4% accidental vs 14% abusive) but less likely if reported to have occurred while cooking (25% accidental vs 4% abusive) or due to a spill (7% vs 1%).10 Pull down injuries, often from hot beverages, are one of the most common causes of accidental scalds in young children. While most are accidental, neglect and lack of supervision must always be considered. The youngest reported age for a pull-down scald was 8 months and a child able to climb into a bath was 16 months, highlighting the need for a detailed history and developmental assessment.12
While the absence of administrating first aid may be considered neglectful, there is no current evidence that supports this as a differentiating factor between abusive and non-abusive thermal injuries. Studies show that parents’ knowledge about appropriate first aid is poor.13 Burns first aid measures are simple but effective at reducing burn severity and should be a Public Health promotion priority.
General examination
It is important to include a development assessment, with an emphasis on correlating the mechanism of injury with the child’s developmental stage. Consideration for child protection principles should be followed. Photographic imaging of injuries should be considered.
Examination of the burn
In this article, we will discuss the most common burns seen in childhood: scalds and contact burns. Remember that other types of burn may also present with child protection concerns.
A meticulous examination of the burn noting the depth, anatomical area involved, TBSA % and pattern is paramount. There are certain characteristics of the burn itself that should evoke concern. Evidence has shown increased likelihood of abuse if a scald has bilateral pattern, TBSA >10% and full thickness depth.9
Scalds—non-inflicted
Scalds are the most common burn injury accounting for 58% of all burns in children.12 Accidental scalds are frequently caused by spillages of hot drinks or hot liquid in food preparation and are found on the head, neck, trunk, face and upper body from the ‘pull down mechanism’ (figure 2). The burn pattern may demonstrate irregular margins, an irregular burn depth and asymmetrical involvement. It is important to consider evidence of neglect in the history when examining burns. Children may present with burns characteristic of accidental scalds due to lack of supervision .

Pull down scald injury.
Scalds—inflicted
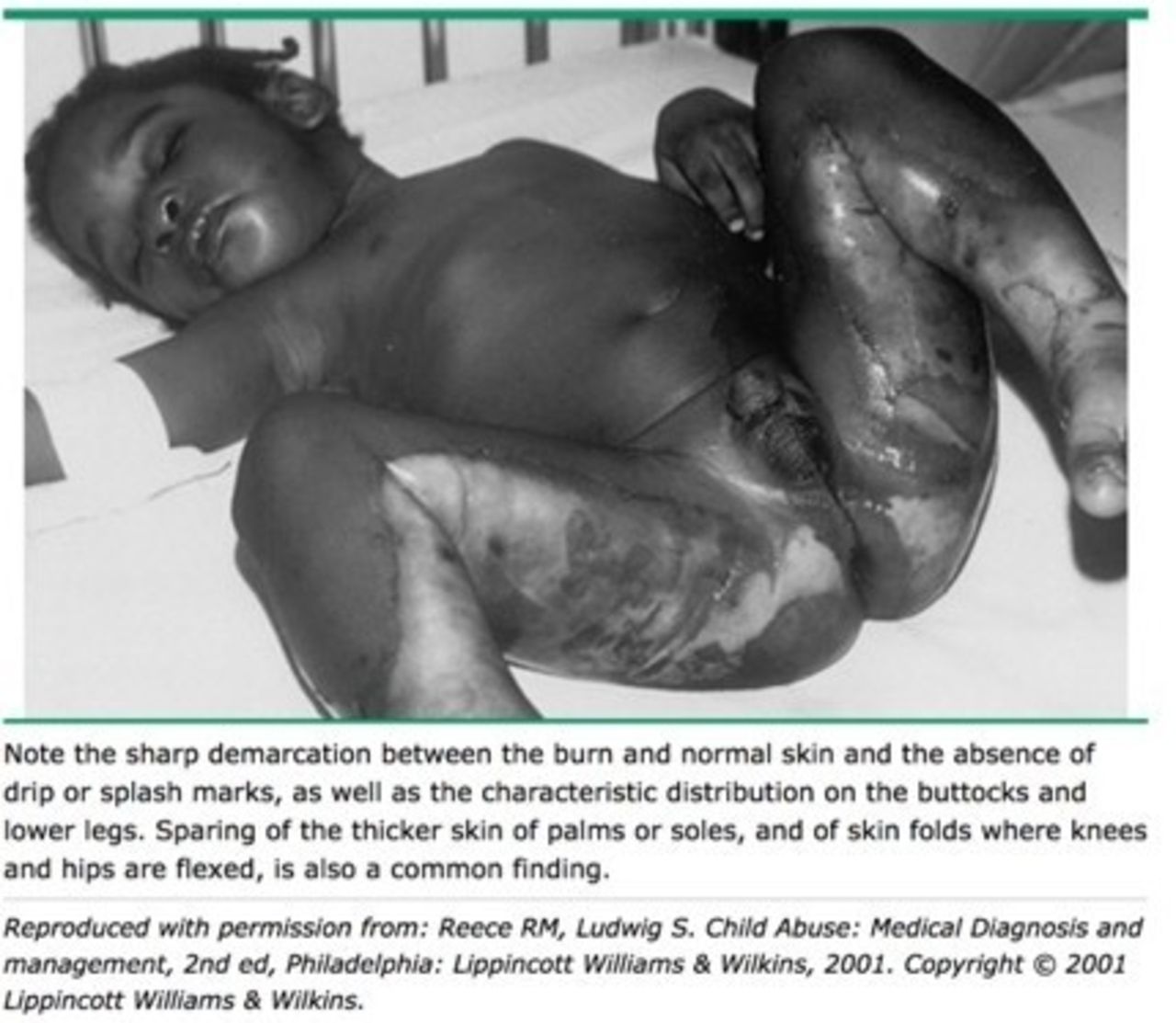
Scalds due to maltreatment have been described to differ by site, depth, symmetry and the presence of sharply delineated borders. Inflicted scalds can be seen on the lower limbs, buttock and perineal regions and may be unilateral or bilateral. The typical pattern seen in forced immersion is a symmetrical burn to both sides of the body with clear margins, circumferential (glove and stocking pattern) and evidence of skin fold or central buttock sparing with uniform burn depth14 (figures 3 and 4).

Immersion burn

Stocking immersion
The absence or presence of splash marks is no longer considered pathognomonic of child maltreatment. Children being held in water may struggle to get away from the scalding liquid (and so will have splash marks) and children who jump into a bath with hot water may ‘freeze’ giving themselves a symmetrical, unsplashed burn distribution.15 This highlights the importance of collating history, examination and further social and family information of this case and seeking expert advice where child protection concerns arise.
Contact burns
It can be difficult to differentiate between contact burns caused by maltreatment and those not. All contact burns are often clearly demarcated in the shape of the causative agent.
Children suffer accidental contact burns from irons, hair straighteners, oven doors or hobs. Accidental contact burns are predominantly caused by children touching hot objects and therefore seen on the fingers or palm of the hand12 (figure 5).

Brand burn.
The most common reported cause of inflicted contact burns are from cigarettes, irons, hair dryers or domestic heaters.12 Burns may also occur from atypical instruments such as a hot spatula.14 Burns in inflicted contact burns can be found on the limbs, back or trunk and areas where the child themselves cannot reach. Burns are often multiple and may co-exist with other injuries suspicious of abuse9 (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contact burn pattern suggesting abuse.
Case
You have completed your history and examination. You do have some concerns that this case may be an inflicted injury and wonder what investigations, if any, you need to perform.
Investigations
It is important to remember that burns in cases of suspected child abuse are a sign of physical abuse or neglect. We would recommend that you adhere to your local safeguarding guidelines and consider referral to social services and for a child protection medical. The Royal College of Paediatrics and Child Health (RCPCH) companion recommends that in children <2 years where physical abuse is suspected, investigations to exclude occult injury is required (eg, skeletal survey in those <2 years and cranial CT when <1 year of age).16 In children >2 years, further investigation should be decided on a case-by-case basis.
Despite these recommendations by the RCPCH, the rate of investigations in children with burns is lower than when children present with bruises and other physical injuries9 (table 1). This is despite a comparable proportion of positive findings.
Comparing percentage of diagnostic investigations performed (bold) and percentage of positive results (in brackets) for children with burns versus* other, whom were referred to a Child Abuse Paediatricians.9
Other considerations
A home visit may collaborate facts and allow the collection of further evidence. This should occur in a detailed and forensic manner. A number of conditions have been mistaken for inflicted burns.11 It is important to include the multidisciplinary team in suspected cases of abuse. A formal review by a burns surgeon for their specialist input would be advisable, specifically commenting on the depth of injury, the degree of healing and their interpretation of the case.
Clinical prediction tool (CPT)
The BuRN Tool is a CPT developed to aid clinicians in identifying child safeguarding concerns in children with burns.17 The tool is currently undergoing an implementation evaluation and pending these results, it may play a significant future role in the assessments of burns injuries.
Conclusions
Burns in childhood are a frequent presentation to EDs, with a significant proportion attributed to maltreatment. The recognition and initiation of child protection proceedings in these instances are imperative in preventing future harm to the patient. We recommend a detailed history, examination and a broader consideration of the social and historical background, appreciating that it is not one feature in isolation but an amalgamation of key variables that allows the clinician to appreciate the bigger picture.
References
Footnotes
Contributors SM conceived this review. SM, RB and ZR were all co-authors on this paper. AMK reviewed the final draft and helped develop this review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SM and AK are undertaking research in the BuRN-Tool.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.