Article Text

Abstract
Determining severity of illness and undertaking an adequate risk assessment is a fundamental part of acute paediatric practice. This review highlights physiology, communication, heuristics and external elements as factors which influence decision-making and discusses how incidence of disease and seniority of clinician impact might influence outcomes.
- decision making
- acute paediatrics
- gut feeling
- heuristics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
At the core of the practice of acute paediatrics is an underlying conundrum. The chance of serious disease is low but the consequences of not treating specific illnesses are devastating. In the developed world, despite widespread immunisation, this task is no easier now than it was 10 years ago. While the search for valid biomarkers and validated scoring systems continues at pace, there have been no significant innovations in diagnostic tools to aid the recognition of serious illness in a generation of paediatrics.1
Rosie is an 18 month girl who presents to the Emergency Department with a 3 day history of fever and increasing parental concern that she isn’t eating or drinking enough. Today she has had a couple of vomits and her mother has described her as ‘shaky’. She is clearly coryzal and looks miserable, but not irritable. Temperature is 39.1, she has a pulse of 167 and a respiratory rate of 38. Her central capillary refill time is below 3 s and her peripheral return is 3 s. She feels very hot on the chest but has cold hands and feet.
The diagnostic approach to the child above, while shaped in some part by (inter)-national guidance, is still very much in the hands of the senior decision-makers—clinicians of both paediatric and non-paediatric backgrounds who have experience in the management of ill children. The decision to discharge, observe, investigate and treat, at its core, is based on the application of experience. How are these decision-making processes shaped and how can we refine and improve them to safely reduce admissions and more effectively target those children needing interventions? This article explores the art and science of decision-making in acute paediatrics to help clinicians and educators understand the processes they may be unconsciously using every day so that they too can teach others.
A common problem
Although the probability of diagnosing a life-limiting infection is low,2 the stakes in any acute paediatric assessment are high. High expectations follow the responsibility of decision-making in an acute paediatric consultation. If the clinician makes a diagnosis that later turns out to be wrong, the question will inevitably be asked, ‘At the time why wasn’t it clear that the diagnosis was X?’ Notwithstanding gross negligence there are four factors (physiology, communication, heuristics and external factors) that complicate the process of diagnosis.
The nature of paediatric physiology
Physiological values are complex in paediatrics. They are more than complicated because although there are published ‘normal values’ which will guide the clinician in knowing whether a child is tachycardic or tachypnoeic, these are in fact reference ranges that were initially based on expert opinion.3 Although meta-analysis shows these reference ranges to be at least somewhat valid,4 it is probably safest not to think of them as ‘normal ranges’ at all since much of the data includes children in abnormal circumstances. Indeed, the clinician who relies on these values will by definition be unlikely to have a ‘normal’ child in front of them. What is the normal heart rate of a 10-month-old infant with ear-ache, a temperature of 37.9 and is due a feed? Physiological values have a huge importance in paediatric assessment; however, they must be interpreted in context and often only become useful when a trend is established. This is particularly challenging in a primary care or emergency medicine setting, where it is not desirable to observe every patient. Furthermore while in secondary care it is usual practice to observe a patient following the administration of an antipyretic to reduce distress (not fever), there is no evidence to suggest that response to antipyretics has a predictive value in determining the presence or absence of serious disease.5 It has also been found that temperature–pulse charts perform worse than pulse alone.6 The observation (always post hoc) of the presence of ‘unacknowledged’ tachycardia is often highlighted in serious care reviews. This leads to very defensive medicine when determining management plans in infants with raised heart rates, whereas cohort evidence does not support using heart rate alone as a decision-making aid.7 This results in a dissonance between the decisions that a clinician would like to make based on the child they see in front of them, and the child that is described in the observations charts. Often the challenge is finding physiological objective evidence to support a decision already made, based on the overall judgement of degree of illness.
The variability of communication
Decision-making relies on information, and one of the key components of paediatric practice is the challenge of history taking. Much of what the clinician hears during a paediatric history is inferred or requires interpreting. For example, a parent may report ear pain on the basis of witnessed ear pulling or they may report foot pain on the basis of a limp. The first parent is likely to be right, while in the second case the source of the pain is far less certain. Clinicians must not only learn how symptoms manifest but also how they are commonly reported, which the authors find to be strongly influenced by carer anxiety.
Another key difference is the complexity of paediatric examination. How exactly does one do a cranial nerve examination on a 4-day-old infant? What does it mean when you palpate a 2-year-old child’s abdomen and they cry? Is this a sign of pain or resentment of strangers? Clinicians must innovate (blowing on a 4-day-old infant’s face gives quite a lot of cranial nerve information), extrapolate (If unable to see in a child’s throat, knowing that they have just eaten a packet of crisps and drunk a carton of fruit juice may be all the information needed) and economise (the child cried as soon as the clinician went near them, therefore other information will have to be relied on when assessing their abdomen) in order to achieve the best possible examination. All these examples demonstrate skills that are difficult to teach, and all must be observed and experienced. Regardless of a clinician’s knowledge (eg, of the cranial nerves), the application of how to interpret and put into context the outcome of that knowledge requires repeated exposure. Learning the decision-making process does require exposure to patients at both undergraduate and postgraduate levels. A developing issue will also be the communication and use of big data in the deployment of artificial intelligence. As diagnostic systems combine, that is, one programme to analyse past presentations, presenting complaint, observations and special tests to generate an overall level of risk, it will be vital that ‘risk’ is applied and explained appropriately. The diagnosis of disease still remains a very human endeavour, but the medical community must be prepared to develop with new approaches and techniques8 and determine how best to have these discussions with families and carers.
The heuristics used by clinicians and how they are affected by cognitive biases
A heuristic (or more precisely a heuristic technique) is ‘any approach to problem solving, learning, or discovery that employs a practical method not guaranteed to be optimal or perfect, but sufficient for the immediate goals’ (https://en.wikipedia.org/wiki/Heuristic). Heuristics are used, often unconsciously, by experienced clinicians to amalgamate the large amount of information they obtain by history taking and examination. Heuristics are a blessing and a curse. It would be impossible to safely see the large number of children needed per shift if a detailed problem-solving approach was adopted involving a dissection of all components of a history with a minutiae examination. At the same time our heuristics create potential biases9 (table 1) which, if not recognised, may well result in serious harm or even death for the patient and a debilitating second victim phenomena for the professionals involved.
A selection9 of cognitive biases originally described by Croskerry
To avoid falling into traps you first need to be aware that the traps exist in the first place. Kahneman and colleagues have popularised the concept of fast and slow thinking: the distinction between instinctive (type 1 thinking) and more reflective, analytical cognition (type 2).10 This model relates to clinicians in day-to-day practice when it comes to achieving a balance between efficiency and effectiveness. Clinicians may employ type 1 (fast) thinking which allows them to make frequent, reflex decisions in order to deal with a large volume of patients in a short period of time. This more intuitive way of thinking is less appropriate when that same clinician is faced with a complex diagnosis or an infrequently encountered clinical scenario. To be successful in these cases, the clinician is likely to need type 2 (slow) thought processes which bring together a number of decision-making facets.
Its application in practice, however, is not a simple case of avoiding snap judgements. In emergency situations, the intuitive recognition of a tension pneumothorax may be life saving. Furthermore, overthinking problems can create clinical dilemmas (and much confusion for parents/carers) with no net benefit. Conversely if we do not have weights or measures to keep our unconscious in check, then it is inevitable that patients will slip through the net. One counter-measure to biases is the application of Bayesian statistics. At any given moment patients have prior probability of disease based on demographics and risk factors. Risk of disease alters following a test result, which can be anything from observation to the latest meningococcal disease biomarker (figure 1).
- Download figure
- Open in new tab
- Download powerpoint
Using Bayesian statistics.
The impact of external factors: parents/carers and/or the clinical environment
Bradley is a 4 year old boy. Yesterday he tried to swing on some monkey bars, slipped and hit is head on the edge of step after a fall of perhaps a 2–3 m. He wasn’t knocked out and despite a bump to his head appeared well in himself an hour later. However in the evening he was noted to be not himself and vomited a couple of times before tea. On arrival in the Emergency Department he has vomited a couple of more times. His parents say he is pale and is definitely not himself. Examination reveals no focal abnormality.
The decision to scan a child’s head is also a good example of differing agendas in the decision-making process (table 2). The National Institute for Health and Care Excellence (NICE) guidelines are designed around a principle of ALARA (radiation exposure should be As Low As Reasonably Achievable) which means that the purpose of a scan should really be to detect treatable injury. While a clinician may be comfortable with this principle, since it protects children from harmful radiation, parents may prefer certainty and push for a head scan even when the chances of harm from the scan are greater than the likelihood of treatable brain injury.
Differences between clinician and parent/carer and child or young person (CYP) agendas
Differing agendas can potentially create a dangerous understanding gap in a paediatric consultation.11 12 Take the example of one of the most common presentations in child health: the febrile child. A doctor sees a 2-year-old child with a history of cough and fever. Working through the above agendas, they establish that the child is well hydrated, that they have all the signs of a viral upper respiratory tract infection and no signs of pneumonia, sepsis or meningitis. Thus the clinician’s agendas are fulfilled. However, in terms of the parent’s agendas, the clinician is unable to treat the cough and is unable to give a specific time frame for when the symptoms will resolve. However, it is the third parental agenda listed above which provides the greatest paradox since it is completely at odds with good safety-netting. To safely discharge the patient, the clinician must in fact warn the parent of the possibility that secondary infection is possible and therefore when to seek a further assessment.
The impact of incidence of disease
One of the most consistent challenges in paediatrics is the overall low probability of significant pathology. The clinician faces a decision between a path of reassurance and avoidance of overtreatment/overinvestigation, or a path of investigation or possibly empirical treatment. The likelihood that investigations or treatments will be of value is greatly reduced when the probability of significant pathology is very low (palpable but otherwise uncomplicated cervical lymph nodes in children). There are few examples in paediatrics where a particular presentation has such a high chance of finding something significant that investigation is always needed (as in Henoch-Schonlein purpura where urine dipstick is always needed).
Nor is the probability factor that influences the decision-making a constant. Vaccination rates have, for example, altered the probability that a petechial rash might be due to meningococcal infection. Often, guidelines lag behind such shifting sands, partly due to a lack of published data to confirm that things have changed and partly due to the inevitable delay from publication of new evidence to inclusion in the guidelines.
Decision tools in paediatrics are rarely as sensitive and specific as we need them to be. The NICE febrile child guideline, perhaps the most used decision tools in paediatrics in the UK, has a poor sensitivity and specificity.13 By contrast, the head injury imaging guidelines are a rare example of a decision tool which has achieved specificity without sacrificing sensitivity.
When approaching a clinical scenario, doctors tend to use a combination of Bayesian probability (making and assessment of the likelihood of a particular diagnosis) and hypothetico-deductive technique (formulating a hypothesis which can be tested). Both are problematic, especially in paediatrics. Take the diagnosis of asthma in the under-5-year age group—a hotly debated subject.
Ahmed is a three year old boy. He has had several episodes of wheeze requiring inhalers, which started when he was two years old. Initially these were all triggered by respiratory tract infections, however the two most recent episodes had no apparent trigger. Following the second episode, the doctor considers the pros and cons of giving a steroid inhaler and the parent asks if Ahmed has asthma.
Atopic asthma is rare in the under-5-year-old age group, however, there are children who have recurrent episodes of wheeze which are not exclusively exacerbated by respiratory tract infections. A clinician would rightly consider (Bayesian probability) the fact that the most common reason by far for a 3-year-old child to have recurrent episodes of wheeze is viral-induced wheeze. Improbability is not impossibility, however, and because the incidence of a disease at different ages tends to map to a curve, there is always an outlying possibility of an early presentation. Even considering risk factors is of little help here. In fact, the latest British Thoracic Society-Scottish Intercollegiate Guidelines Network guidance for the diagnosis of asthma has de-emphasised family history of atopy due to the fact that this is a poor indicator of a diagnosis. So, if probability does not give the answer, what about a test to confirm or refute the hypothesis (hypothetic-deductive technique)? Unfortunately, there is no perfect test for asthma, and this is especially true the younger the patient. For this reason, many treat the introduction of a steroid inhaler as the test itself, leaving them at risk of confirmation bias if the episodes self-resolve.
The combination of rare versus common diagnosis, with no good test to distinguish between them, is a recurring theme in paediatrics. Essentially, every benign diagnosis has an evil twin, and it is often very difficult to tell them apart. This is just as true for the question that is asked in primary and secondary care every day around the world—does this child have an uncomplicated viral illness or do they have early sepsis? The odds are always going to favour viral illness but the cost of being wrong is the potential loss of a child’s life. The inability to prove a negative is one of the biggest challenges of decision-making in paediatrics.
Senior decision-makers and the use of gut feeling
Since diagnosis in acute paediatrics cannot rely on tests or decision tools,14 15 many guidelines point the way to a ‘senior decision-maker’. This term remains ill-defined but is a crucial aspect of the process which allows children to receive a safe and accurate clinical assessment. Clinicians with the necessary experience in assessing children do not tend to rely on guidelines or tests to make decisions (though will use these where appropriate).16
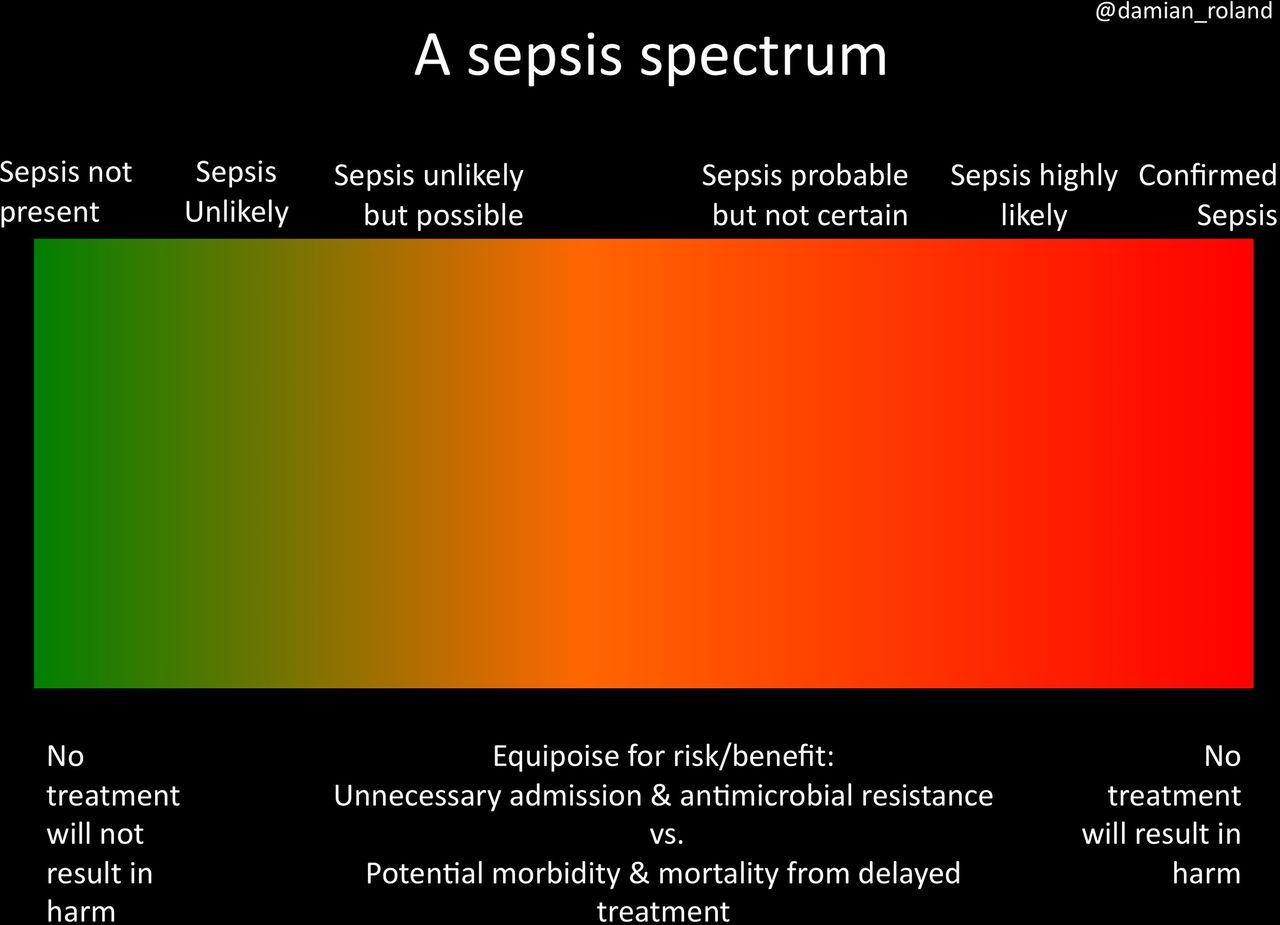
Sitting alongside a number of well-described educational and mathematical diagnostic approaches such as the hypothetico-deductive technique and Bayesian probabilities is the innate sense that a diagnosis or management pathway is the correct thing to do. This utilisation of gestalt and gut feeling is a core practice of senior decision-makers. The terms are used interchangeably but this is not linguistically correct. Gestaltic philosophy describes the way the conscious mind comes together to perceive things, with gestalt defined as ‘an organized whole that is perceived as more (or other dependant on some translations) than the sum of its parts’. Over time this has come to describe the way that a clinician may take a number of different facets of information and bring them together to make a decision. This decision may be contrary to some of the individual pieces of information, that is, the senior decision-maker choosing not to emergently treat the tachycardic, tachypnoeic and febrile child with antibiotics as the presence of coryza with a miserable, not irritable, nature indicating the overall disease process is likely to be viral in origin. Gut feeling has been defined as an intuitive feeling that something was wrong even if the clinician was unsure why.17 Research varies on the impact of gut feeling in clinical practice but it may be as good or better at identifying ill children than individual features such as cyanosis.18 Our inability as a medical community to encapsulate the concept of gut feeling so that training can be improved either implies it is true tacit knowledge (something that is functional but is difficult to describe) or that more intensive research, likely to need the involvement of cognitive psychologists, is required.19 20 This is an important avenue of research as currently there are no standards in exploring the use of gestalt and gut feeling by clinicians in training21 and some conditions are very dependent on the adequacy of gut feeling as a decision-making aid. This is very true for sepsis in the acute care setting. When the diagnosis has been made, the management pathway is clear but it is the diagnosis (often only definitely made when the management pathway has been used), or the consideration of the diagnosis, that is important to prevent morbidity and mortality. While screening tools aid those with inexperience, the deployment of antibiotics in all children meeting red flag criteria is neither sustainable nor in keeping with antimicrobial guardianship. Paediatrics contains many ‘spectrum’ diseases (figure 2), and in the absence of sensitive biomarkers it is likely that gestalt and gut feeling will be used for some time to come. This spectrum evolves over time so that a child may present on the left side and be appropriately discharged only to return 24 hours later on the right hand. Decisions taken may have been entirely appropriate with the given information.22 The ability to develop clinical intuition is a process which is developed over repeated clinical contacts, often refined by trial and error. The point at which one becomes intuitive in assessing childhood illness is likely to depend on several factors. While the number of patient contacts is likely to be the greatest of these, good feedback processes and the ability to learn from error is certainly a major factor in developing a sixth sense for when a child has a serious illness or injury. Education and supervision therefore remain a core component of improving medical care, and we recommend that those involved in decision-making in paediatrics make full use of any resource that involves the passing on of expertise as a way of accessing the tacit knowledge developed by others. Educators can use the strategies in box 1 to improve learner’s decision-making.
{kind=link}
A sepsis spectrum.
Strategies for clinical educators to improve learners’ decision-making (via Roland, Have we forgotten to teach how to think)21
Provide adequate and appropriate clinical exposure
Don’t assume teaching about cognitive biases will enable learners to avoid making them
Trainers must consider discussing why decisions were made, not just what decision was made
There exists a great deal of tacit knowledge among those clinicians who assess children. Because this knowledge sits outside the evidence base, it is not easily included in guidelines or decision-making tools. It should be possible to extract this knowledge in a valid way through the use of tools such as the Delphi method. Doing so may reveal the key elements of decision-making that only develop through the experience that comes from repeated patient contacts. This is a largely untapped resource which has until now almost exclusively relied on clinician to clinician discussions and may well explain the popularity of social media as a platform to have these grey-area debates.23 While face-to-face discussions will always be a valuable resource, they are a scarce commodity for many at the point of decision-making. The publication of large-scale consensus opinion would go a long way to the development of this important but complex element of the decision-making process.
Conclusion
Decision-making in paediatrics is influenced by a number of factors, some dependent on child and some on the clinician. Recognising cognitive biases, providing access to senior decision-makers and further understanding the role of intuition in clinical practice, are all important in improving outcomes for children in acute paediatrics. Clinicians should use published evidence, guidelines, decision-making tools and available expertise wherever possible to improve their understanding of how to make the best decision in any given clinical scenario. One of the most significant factors in decision-making, the development and application of tacit knowledge, is poorly understood and is a potential area for research which may greatly influence the improvement of decision-making in paediatrics.
References
Footnotes
Twitter @damian_roland
Contributors Both authors contributed equally to the article.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.