Article Text

Abstract
Making the decision as to whether an injury is a result of child abuse or not is stressful for both the family involved and the clinical team. It is not a decision that is taken lightly, and with an increasing expectation by the investigating agencies, lawyers and the public in general, to ensure that it is based on explicit ‘evidence’, clinicians need to be up to date with the latest scientific publications in the field. This article aims to summarise the current evidence in relation to all physical injuries except those pertaining to the central nervous system, which will form a separate article. It will examine the pattern of accidental and abusive bruises, fractures, burns, abdominal injuries and oral injuries focusing on discriminating features and necessary investigations.
Statistics from Altmetric.com
Which children are more likely to sustain physical abuse?
The literature consistently records that the youngest children (predominantly <3 years) are most likely to be physically abused, although it is not restricted to this age group, as those up to late teens are also recorded as being abused.1 2 Children aged <1 year experience the highest rate of abuse (21.9 per 1000 children).3 Sociodemographic characteristics vary from one country to another, with lower socioeconomic status having a greater association with physical abuse in many North American studies,4 and a suggestion of increased prevalence of abuse among immigrant children (these children are eight times more likely to be reported as abused in Sweden2), asylum seekers5 and internationally adopted children.6 This reiterates the need to be aware of all the sociodemographic circumstances of the child. It is difficult to identify whether there is a true association between abuse and specific social factors, as opposed to increased reporting/recognition of abuse in certain groups in society. Certain characteristics in the children themselves may render them more vulnerable to abuse, including disability, and in particular behavioural or learning difficulties,7 8 while practitioners may operate lower thresholds for referral of certain minority groups.3
Which bruises suggest an abusive aetiology?
Bruising remains the commonest abusive injury encountered,9 with the head and neck being the most commonly recorded site.10 However, children will always sustain bruises as a consequence of simple accidents, so distinguishing these two situations is key.10 Contrary to popular belief, boys do not sustain more bruises than girls.11,–,14 It is clear from the literature that the pattern of accidental bruising in young children is strongly influenced by their level of independent mobility, with non-mobile infants least likely to sustain accidental bruises (prevalence <1%).13 Thorough investigation of a baby with an unexplained or inadequately explained bruise is essential, as some may have underlying coagulopathies while others may have been abused.15
Once children start to move around independently, bruising increases incrementally (prevalence: crawling, cruising 17%, or walking >50%). However, even in these children, the bruising tends to be found in specific locations (see figure 1). The commonest site for accidental bruises in mobile children is the knees/shins.14 16 In young children (<6 years), accidental bruising to the head occurs predominantly in a ‘T’ shape across the forehead, nose, upper lip and chin, and in more than a third (37%) bruising is also found on the back of the head.17 It has been clearly shown that accidental bruising occurs on the front of the body and over bony prominences and <6% of accidental bruises to the face are found on the cheeks or periorbital area.11 13 17 In contrast, abusive bruises are found predominantly on the head and neck, where the bruising occurs on the ear, neck and cheeks, all of which are extremely rare sites of accidental bruises (figure 2).9 18 19 Any part of the body may be bruised as a consequence of abuse, but specific areas such as the forearms, upper limb and adjoining area of trunk, or outside thigh may indicate ‘defensive bruising’ where the child has tried to protect themselves from the blows being rained upon them.9 20 Occasionally an abusive bruise may be explicitly linked to its aetiology, if there is a positive or negative imprint of the weapon (eg, studded dog collar, belt buckle)21; however, the tracking of bruising may distort the precise location of the original injury (eg, vertical gluteal cleft bruising when the child was struck horizontally22).

Accidental bruising patterns.
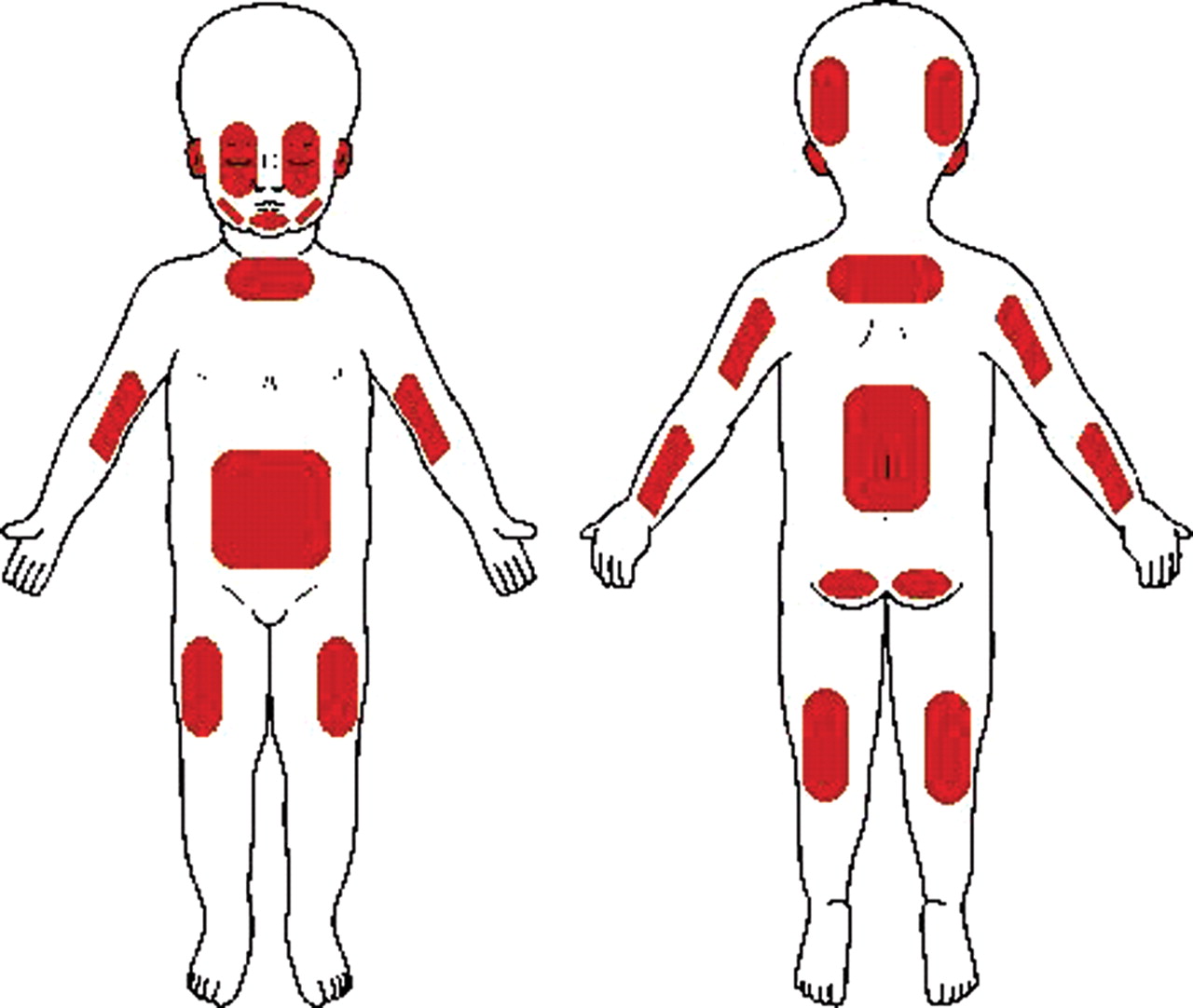
Abusive bruising patterns.
It has recently emerged that the presence of petechiae in association with bruises is a strong predictor of abusive injury with a positive predictive value of 80 (95% CI 64.1 to 90.1), although their absence is of no diagnostic value. Thus it is important to examine carefully for the presence of petechiae with bruising.12 As with all injuries, other differential diagnoses must be carefully considered, including coagulation disorders, Mongolian blue spots23 (which can occur on the back, knee, scalp and feet as well as the lumbosacral area), Henoch–Schonlein purpura, hair braiding,24 etc (box 1).
Box 1 Evaluating bruises
Assessing a bruise of possible abusive aetiology
▶ Document location, number, size (two maximum diameters), petechiae if present and history of cause (if any given)
▶ Photograph relevant bruises, including a right angled measuring device, and colour scale in the photo
▶ Full blood count, coagulation studies, von Willebrand Factor, PF A 100
▶ Family/personal history of bleeding disorder? Discuss with haematologists
▶ Age <2 years? Consider other occult injury (fractures, retinal haemorrhage, intracranial abnormality)
It has long been the practice of clinicians to offer a likely age for bruises found, and this is relied on heavily by the investigating team of social workers and police. Some authors still give explicit timetables for the appearance of different colours (red, blue, yellow, green) in bruises25; however, it has been clearly established that there is no scientific basis for such a timeline,26 and as such a personal estimation may be extremely misleading. It is clear that not only do different colours appear in the same bruise at the same time, but each of us perceives colour differently, and we may not even agree with our own assessment of colour between the assessment of the live child and subsequent review of a photograph.27,–,29 New techniques are being explored which may offer a method of dating bruises, including reflectance spectroscopy, chromophore concentrations, etc, but these are not yet in clinical practice.30 31
Could this mark be a bite?
Abusive bites are particularly important injuries to identify in children, as they are the only physical injury which offers the potential for a forensic identification of the perpetrator.32 This may include reconstruction of the dentition of the perpetrator of the bite, with or without additional DNA evidence. However, this relies on the initial examining doctor recognising that the injury could be a bite. Children are frequently bitten, predominantly by animals or other children. Dog bites are typically narrow, and they produce a tearing injury. Any adult bite on a child sufficient to leave a mark is deemed abusive. An adult bite classically results in a 2–5 cm oval or circular mark, made by two opposing concave arcs, with or without associated ecchymosis and/or petechiae. However, the bite may be incomplete, located over a curved surface or be a dragging injury, distorting this shape. Traditionally, the method of distinguishing between an adult (and thus abusive) bite or a child bite, relies on measuring the intercanine distance within the bite, which in human adult bites are deemed to be 3.0–4.5 cm; 2.5–3.0 cm in a child or small adult; and <2.5 cm in a child. However, it is important to bear in mind that there can be considerable racial, sexual or individual variations and that adult dentition is reached by 12 years. In addition, if the adult has distorted dental anatomy, their intercanine distance may be reduced. Likewise, another important facet to bites, is that a child who is being attacked may also bite their attacker, which may help in their identification.33 The full analysis of a bite therefore is a specialised field, as consideration must also be given to a differential diagnosis such as skin conditions—for example, ringworm (box 2).
Box 2 Evaluating possible bites
If you suspect that an injury may be a bite then you must do the following:
▶ Obtain clinical photographs of the bite, in each plane if it is on a curved surface
▶ A right angled measuring device must be included in the photograph, consider serial (daily) photographs if there is going to be a delay before forensic dental assessment
▶ Contact a forensic dentist immediately via the British Association of Forensic Odontologists (http://www.bafo.org.uk)
Which fractures may be the result of abuse?
Fractures are a common injury in childhood, with between a third and two-thirds of boys and 40% of girls sustaining a fracture by their 15th birthday.34 35 Many are related to falls, motor vehicle collisions, playground or sporting activities,34 and most frequently involve the upper limb.35 Distinguishing the inflicted from the accidental fracture is challenging, but this is an injury where the age of the child seems to be a key factor. A large-scale case–control UK study has shown36 that 85% of accidental fractures occur in children >5 years, while 80% of abusive fractures occur in children <18 months. This pattern is borne out in US data too, where it is noted that while the incidence of abusive fractures is 15.3/100 000 children aged 0–35 months, the incidence in those <12 months is 36.1/100 000 dropping to 4.8/100 000 for those aged 12–35 months, respectively.37 Determining how many abused children have fractures (occult or overt) is more difficult, as not all children being assessed for possible abuse undergo standardised investigations to detect fractures. Overall, it is estimated that a third of abused children have fractures,38 39 many of which are occult.40 One finding that is clear across all studies, is that multiple fractures have a strong association with abuse.36 37 The biomechanics of fractures is a complex subject (well reviewed by Pierce and Bertocci41), but it is becoming increasingly clear that if clinicians are to make even the crudest estimate of the likelihood that the fracture found can be explained by the history offered, we need to be much more ‘forensic’ in our recording of the incident. Specifically, when presented with a fracture due to an alleged fall, it is important to document the fall height, weight of the child, surface on which the child landed and the way in which they landed to at least estimate the likelihood that the injuries found can be explained by the history given.
Which fractures cause the most concern?
As with bruising, the level of independent mobility of a child is an important aspect of your assessment of fractures. Children who are not yet walking, are far less likely to sustain accidental long-bone fractures.42 43 Overall, the probability that a femoral fracture in a child is due to abuse is 28% (95% CI 15% to 44%), but the majority of abusive femoral fractures are in younger children, particularly those aged <1 year.44 While spiral fractures of the femur are the commonest femoral fractures referred under the child protection procedures, they are only recorded as the commonest abusive fracture in children <15 months of age.45 Overall, the commonest accidental and abusive fracture of the femur is a mid-shaft fracture.44 The published data in relation to determining the precise probability of abuse for metaphyseal fractures are sparse, but in relation to the lower limb, they are certainly more commonly due to abuse than other causes (p<0.001).46
Humeral fractures in children aged <3 years, have a probability of abuse of 48% (95% CI 6% to 94%),44 but here age <15 months versus age 15–36 months, seems a strong predictor of abusive fractures.47 In addition, fracture type is a key element, as supracondylar fractures of the humerus are far more likely to be accidental (though not exclusively so).48 The commonest abusive fractures, on the other hand, are spiral or oblique fractures (in children <5 years old).47 49
Skull fractures are a common fracture in young children, with 80% of accidental and 88% of abusive skull fractures occurring in infants under 1 year of age.49 Thus, although the probability of abuse for a skull fracture is 30% (95% CI 19% to 46%), there are few distinguishing features. The commonest accidental and abusive skull fractures are linear, and usually parietal.50 51 The significance of complex, multiple, diastatic or depressed skull fractures is difficult to define, as published data are conflicting.50,–,52
The fractures with the highest specificity for abuse are clearly rib fractures (probability of abuse of 71%, 95% CI 42% to 91%). These are a rare accidental fractures, but may occur as a consequence of metabolic bone disease, birth injuries or major trauma.53,–,55 Multiple rib fractures, in the absence of a history of bone disease, or major trauma are highly specific for abuse.46 There has been considerable emphasis on the association between abuse and fracture location in rib fractures. While posterior rib fractures raise concerns of abuse immediately, overall, anterior rib fractures are commoner in abuse, while lateral rib fractures are more common in non-abused children.54 56 Cardiopulmonary resuscitation (CPR) has been proposed as a possible cause of rib fractures, potentially creating diagnostic confusion where a child has presented collapsed, with injuries later thought to be abusive. The current published evidence suggests that CPR is a rare cause of rib fractures, and when they do occur they tend to be anterior and may be multiple, but do not occur posteriorly.57 However, the current CPR method proposed by Advanced Paediatric Life Support (includes encircling the chest with the hands, and no studies have yet been conducted to determine the risk of rib fractures from this method.
How are occult fractures best detected?
All children <2 years of age with suspected physical abuse should have a full skeletal survey (SS) performed. Both the recently agreed standards for radiological investigations of suspected non-accidental injury by the Royal College of Paediatrics and Child Health and the Royal College of Radiology58 and the American Academy of Pediatrics59 are explicit about the standard of SS that must be conducted if occult fractures are to be identified, or excluded. This involves 19 images, and must include oblique views of the ribs, which have been clearly shown to enhance the detection of rib fractures, particularly posterior rib fractures.60 61 In addition, it is clear that acute fractures may be missed on SS, or equivocal findings may be misinterpreted as fractures, and as such a single SS may not be adequate.62 If an initial SS is negative or equivocal, but concerns remain then consideration should be given to either conducting a radionuclide bone scan (RNI) in addition,62 or a follow-up SS 11–14 days later.63 64 The advantage of a RNI, is that it can be performed at the same time as the original SS, thus avoiding any concerns surrounding the child protection status of the child on discharge, and fractures become apparent on RNI within 4 h of occurring.65 However, the drawbacks are that not all units can perform or interpret such scans in young children, and certain fractures such as skull or metaphyseal fractures are less accurately defined.
Clearly if unexplained fractures are identified in any child, then consideration must be given to any predisposing factors such as a history of osteogenesis imperfecta, prematurity, chronic disease with possible associated rickets, and other metabolic diseases, and where appropriate, investigations should be performed to identify/exclude such conditions.
When does a burn raise safeguarding concerns?
Burns are a common cause of emergency department attendances, particularly in children <5 years of age.66 Within this age group, mortality from burns is also highest, and the survivors may have significant physical and psychological morbidity. Boys uniformly have more burns than girls (2:1 overall, but nearly double this for children aged 10–14 years).66 While in the Western world, scalds are the predominant burn type,66 in developing countries where gas cylinders are a common cooking utensil, flame burns are by far the commonest type.67 The true prevalence of intentional burns is difficult to determine, and is estimated to range between 10% and 12% of abused children.68 69 What percentage of children admitted to burns units have sustained an intentional burn is unclear, with estimates varying between 1% and 35%.70 However, it has been suggested that burns resulting from neglect, outnumber intentional burns by 9:1.71
Distinguishing intentional scalds from accidental scalds
Accidental scalds in young children are predominantly ‘pull over’ scalds, where the child pulls down a container of hot liquid on themselves, giving rise to a classical pattern of scald burns affecting the upper limb, face, anterior trunk, and/or neck (see figure 3).72 These burns are usually asymmetric, and have an irregular edge, and irregular burn depth. Children may also fall accidentally into a hot cooking liquid. An increasing number of scalds are occurring when older children spill food/drinks straight from the microwave.73 Hot tap water may be a factor in accidental scalds, particularly where there is no legislation about domestic hot water temperature (as in the UK), given that it only takes 1 s for an infant to sustain a full-thickness burn from a liquid at 60°C.74

Accidental scald pattern.
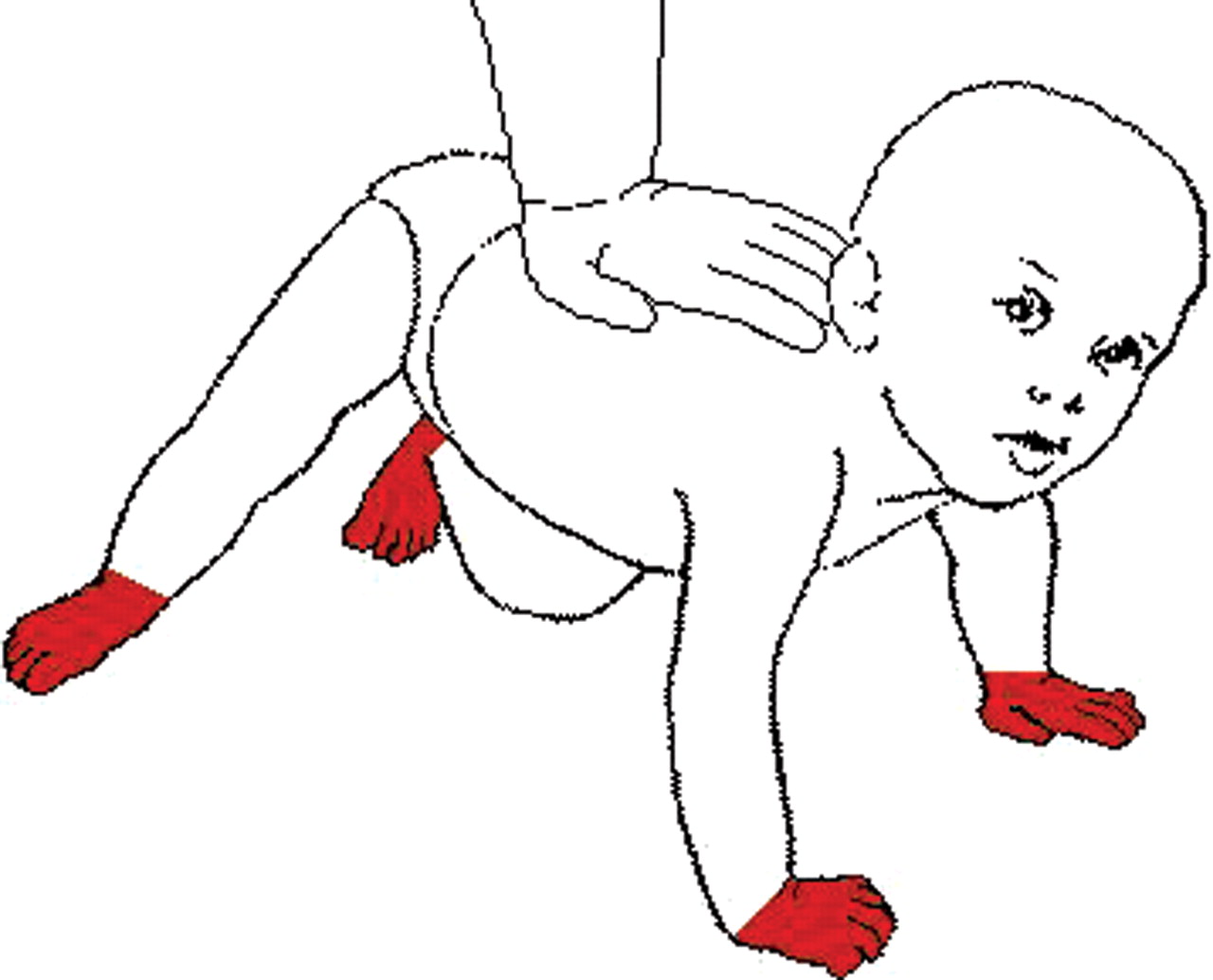
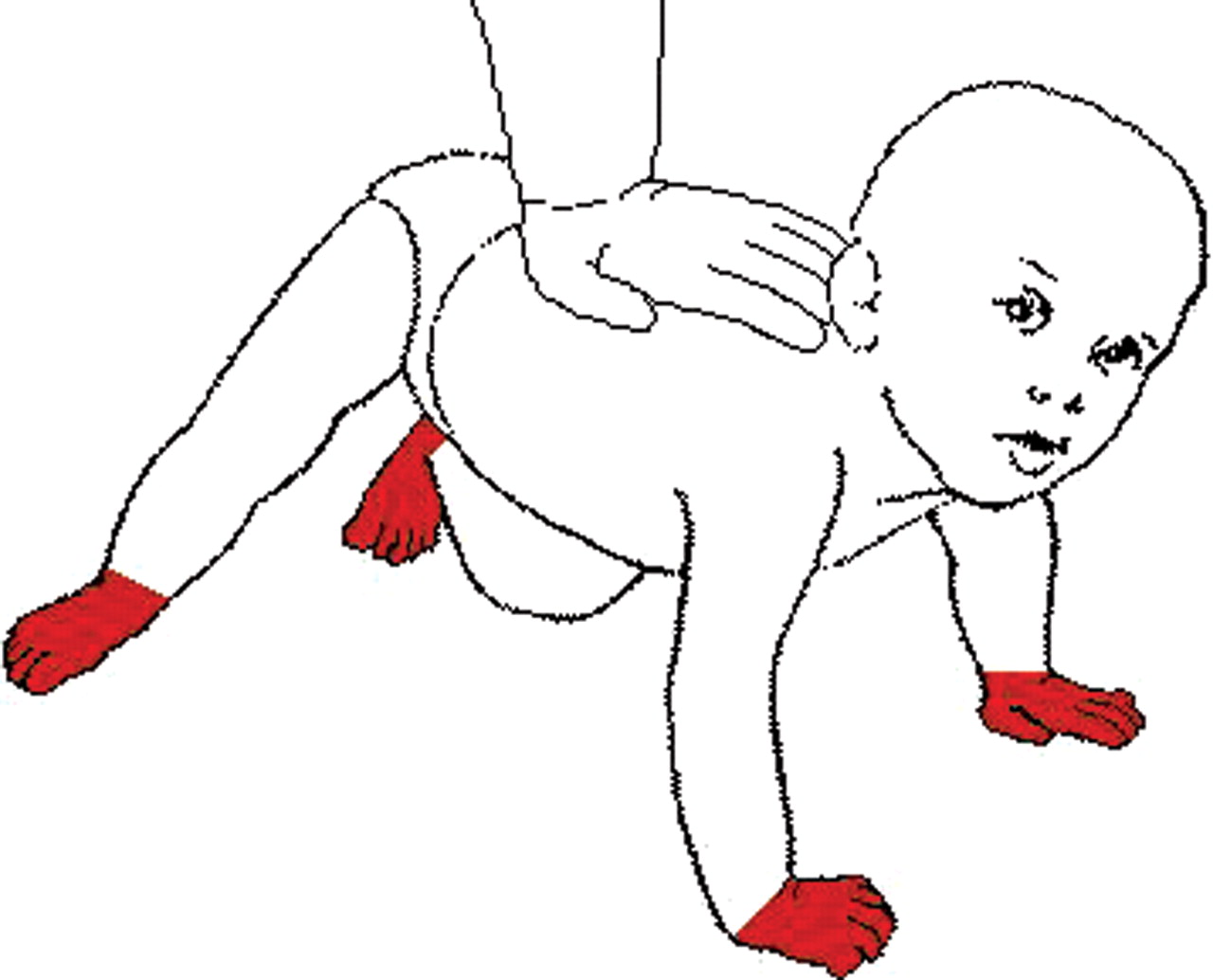
In contrast to the accidental scalds, the intentional ones documented in the literature are predominantly hot water immersion scalds, involving lower limbs, and/or perineum/buttocks, due to immersion injuries (see figure 4). There may be ‘glove and stocking’ burns to hands and feet (figure 5). A single upper limb, or more rarely the whole face may also be involved. Key distinguishing characteristics are that the burn has clear upper limits, is of consistent burn depth, and is symmetrical, in contrast to the accidental scalds.70 Other worrying features are skinfold sparing, presence of other unrelated injuries, previous burns, occult fractures, associated neglect, sibling being blamed and the family already known to social services. However, the current world literature is predominantly drawn from burns unit admissions, and may not reflect the pattern of accidental or abusive scalds which are less severe.

Abusive scald pattern.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abusive scald ‘glove and stocking’ pattern.
The other major burns that children may sustain accidentally or abusively are thermal burns (from flames or hot surfaces). These account for the second largest group of burns in young children.75 76 These tend to be on the palm of the hands, particularly in toddlers. There has been an increase in contact burns due to heated hair devices (eg, curling tongs, hair straighteners) recently, and these may cause initial concern as the burn may be on both the palm and dorsum of the hand or foot.77 These are commonest in toddlers who have had access to devices used by older children, where the device can stay extremely hot for more than 10 min after being switched off. Intentional contact burns tend to be full thickness, affecting the back or neck, have a clear demarcated edge, and it may be possible to match the burn to a household item which has been used to inflict the injury.56 78 In contrast to scalds, these intentional burns occur throughout all ages in childhood.
When assessing potentially inflicted burns the precise history, supplemented if necessary by a home visit (eg, to check domestic water temperature, measure the height of the side of the bath, find relevant household electrical devices, etc), is absolutely crucial. A number of conditions have been mistaken for abuse, including infections such as impetigo,79 scalded skin syndrome,80 photodermatitis (particularly where a child has had contact with a psoralen such as lime juice, or rue and is then exposed to the sun, and over the next 24 h a blistering rash appears)81 or traditional remedies such as moxibustion.82 Moxibustion is the practice of burning the ‘moxa herb’ (although other substances may also be used) over the site of the symptoms—for example, around the umbilicus for abdominal pain, on the chest for dyspnoea, etc.
While cigarette burns are recorded in abused children, unfortunately no comparative studies have explicitly documented the pattern found in intentional as opposed to accidental burns. The few case reports giving details, confirm that intentional cigarette burns are circular, approximately 1 cm in diameter, and may occur on exposed parts of the body. Clinical confusion can arise between cigarette burns and impetigo, but the latter will have scaling around the lesions, and swabs should confirm the presence of the infecting organism.46 Disappointingly, there are to date no comparative studies detailing the difference in location, shape or depth between accidental or inflicted cigarette burns, despite the fact that many paediatricians report seeing such cases. Radiation burns, the commonest of which is sunburn in children, raise the dilemma of whether the burn is an ‘accident’ or ‘neglect’, particularly in young infants. While it is recognised that neglectful burns are commoner than intentional burns, they can be difficult to identify in practice.71 Drawing a distinction between momentary inattention on the parents' part, and inadequate supervision, however, is not always easy. The pattern of burns found in cases of neglect overlap significantly with the pattern found in accidental burns, as these are essentially accidents which could have been prevented, and should have received prompt and appropriate first aid.83
Is a torn labial fraenum indicative of abuse?
The head is the commonest target organ in child abuse,84 with a wide range of oral injuries noted.85 A torn labial fraenum has long been held to be pathognomonic of child abuse, particularly in younger infants.86 Likewise, however, a laceration to the labial fraenum is recognised by dentists as a frequent, and trivial oral injury, occurring owing to a direct blow or fall (eg, from a swing, or falling against a table, etc). In addition, CPR has been noted to be a rare cause of a torn fraenum,87 although it is likely that this will be apparent at the time it occurs. In accidental torn fraena, the injury is usually immediately apparent owing to the profuse bloody saliva produced; thus an accidentally torn fraenum should be a memorable event for parents. Unfortunately, there is a lack of comparative studies in the literature to define the distinguishing characteristics of abusive and accidentally torn fraenum.88 What is clear, however, is that when a torn fraenum is found in abused children, they are almost invariably very seriously or fatally injured (90%).46 Coexistent injuries are common—in particular, fractures and head injury,89 90 abdominal injury87 or sexual abuse.91 It is clear that while there is no published evidence to say that a torn labial fraenum in isolation is not diagnostic of abuse, it is vitally important to fully investigate any infant presenting with an unexplained torn fraenum, particularly those who are not yet independently mobile. If a torn fraenum is found in a child aged <2 years, without adequate explanation, then a full examination and SS should be performed, and if the baby is <1 year formal ophthalmological examination and neuroimaging should also be considered. The injury can only be deemed to be ‘in isolation’ when any other occult injury, or social concerns have been excluded.
Many other oral injuries have been described in abused children, including lacerations to lips or mucosa, dental intrusions, extrusions,88 even forcible dental extractions of healthy teeth by parents as a punishment.92 None of the injuries has unique distinguishing characteristics, other than an absent or inappropriate history. Some injuries may be very subtle, such as dental microfractures causing brownish/grey discolouration, which may be difficult for a paediatrician to distinguish from dentinogenesis imperfecta or other congenital abnormalities.93 Dental neglect commonly coexists with oral injuries, and may be so severe as to lead to complete extraction of deciduous teeth owing to dental caries.94 All children being assessed for suspected abuse should have a full examination of the mouth, and if any abnormal/unusual findings are present, it is important to consult dental colleagues to clarify the full extent of injury and distinguish it from common accidental trauma in children. It is estimated that up to 30% of children aged <6 years sustain accidental dental trauma, with the peak age being 3 years.95 Thus any injury found should be evaluated by dentists experienced in the care of children.
What abdominal injuries occur as a consequence of physical abuse?
While abdominal injuries are rarely recorded in child abuse, they are the second commonest cause of fatal physical abuse.96 Abusive abdominal injuries have a higher mortality and morbidity than accidental abdominal trauma,97 with solid organ (liver/spleen) and bowel injuries being described almost equally. Many children may have sustained both bowel and solid organ injuries.98 Accidental small bowel injuries—in particular, duodenal injuries, are extremely rare in children <5 years of age, and if present without explicit accidental trauma, child abuse should be actively excluded.99 While up to 60% of children with abusive abdominal injury may have abdominal bruising, the absence of bruising does not preclude serious injury. Abusive abdominal injury should be considered in children aged <5 years, with abdominal signs or symptoms, or where severe coexistent head injury is found and such signs cannot be elicited, or in young children with non-specific abdominal symptoms where other abusive injuries are present. If abdominal injury is thought to be present, the optimal imaging strategy is abdominal CT scan with or without contrast, as ultrasound may miss some injuries.100
Summary
When assessing any child, particularly a younger child, a careful note should be made of injuries that are found. There are well-recognised patterns of typical accidental injuries in children, and likewise there are certain injuries that are strongly associated with abuse. As with any other differential diagnosis that is being considered, investigations must be performed to identify occult injury when abuse is suspected, in conjunction with relevant social enquiries. Clearly an injury can only be deemed to be the result of abuse if appropriate medical explanations have been considered, and excluded appropriately, and where the injury has been evaluated in the context of the history offered, past medical and developmental history, and where a full investigation of social factors and any previous concerns has been conducted.
It is recognised that up to 50% of children found to have abusive head trauma had been seen by a health practitioner in the month before this, without abuse being recognised.101 While no injury makes the diagnosis of abuse in isolation, failing to investigate possibly abusive injuries may miss the only ‘window of opportunity’, and the next time the child presents it may be fatally injured.
Acknowledgments
Grateful thanks to Laura Wain for editorial assistance.
References
Footnotes
-
Funding We are grateful for the research grants funding our work, provided by the NSPCC, RCPCH, Welsh Assembly Government and the MRC.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.