Article Text

Abstract
A 15-year-old boy was admitted with a history of cytopenia (white blood cell count 3.170/μm, platelets 90.000/μm) associated with splenomegaly, found during investigations for recurrent mild jaundice due to Gilbert’s syndrome.
He was in good general health, without systemic symptoms; therefore, the leading causes of asymptomatic splenomegaly were excluded. Coagulation, liver tests and abdomen ultrasound (US) were normal, showing a hepatopetal portal flow to the colour-Doppler. There was no sign of haemolysis on haematology investigations. The C reactive protein, immune globulins levels and erythrocyte sedimentation rate were normal, excluding both an infective and an immune regulation disorder. We excluded the haematological malignancy and lymphoproliferative disorders through a peripheral blood smear and a bone marrow biopsy.
His history was remarkable for neonatal sepsis, which required umbilical venous catheter during hospitalisation in a neonatal intensive care unit (NICU). The patient follow-up was interrupted for a while, probably due to his good health condition.
At age 17 years, the child accessed our emergency department. for a minor trauma to the limbs, and his physical examination was unremarkable, except for the splenomegaly. We repeated the abdomen US, with colour flow Doppler (figure 1).
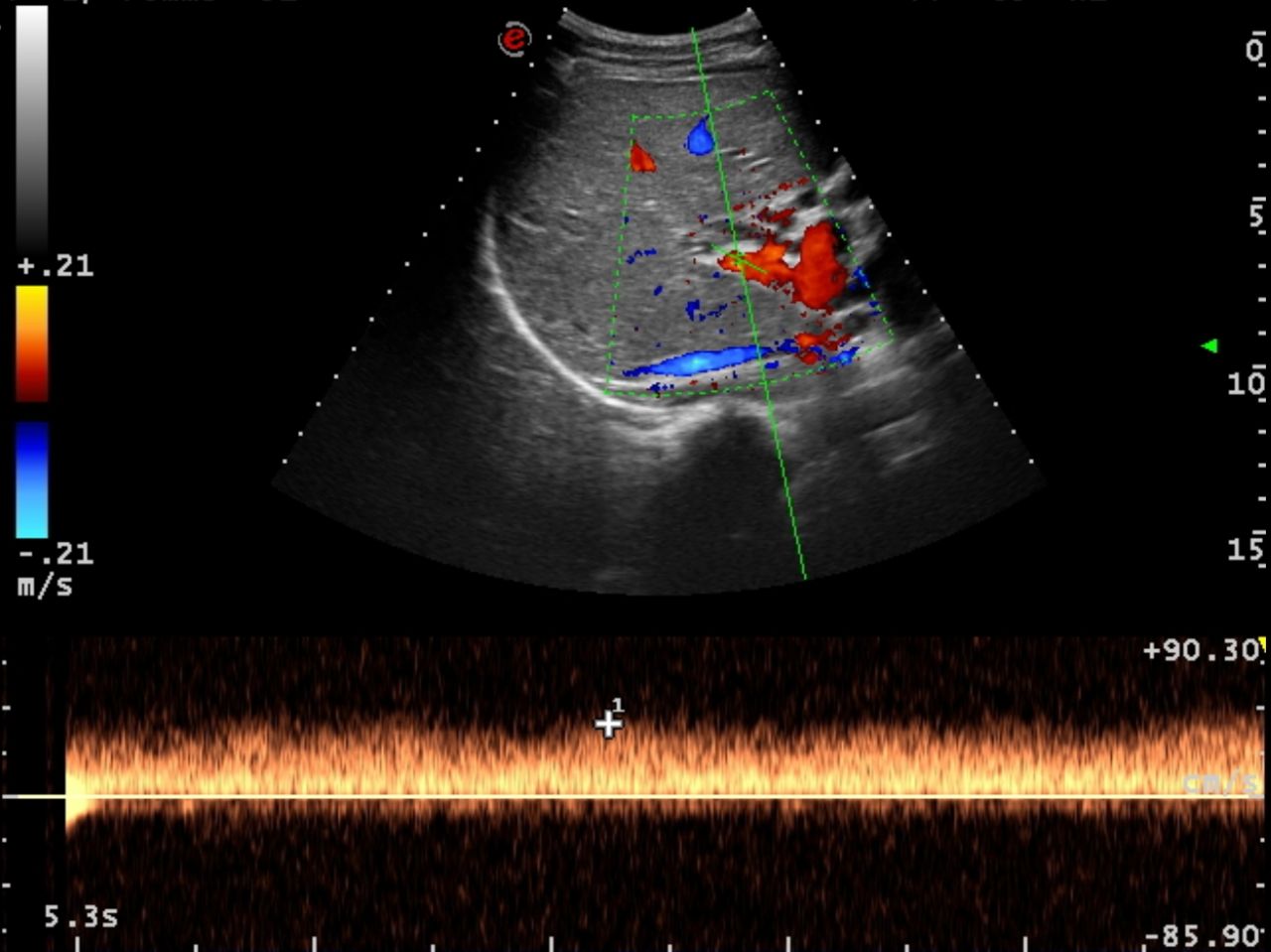
{kind=link}
What is the most likely diagnosis?
Portal vein obstruction
Gaucher disease
Autoimmune sclerosing cholangitis
Leukemic hepatic infiltration
What is the gold standard imaging for diagnosis?
Abdomen Doppler US
Contrast-enhanced CT
CT without contrast
Ultrasound-based elastography
How should this child be managed?
Upper gastrointestinal endoscopy
Beta-blocker therapy
Left-mesenteric portal vein bypass (Meso-Rex bypass)
Transjugular intrahepatic porto-systemic shunt
Answers can be found on page 02.
- general paediatrics
- gastroenterology
- hepatology
- neonatology
- paediatric practice
Statistics from Altmetric.com
Footnotes
Contributors LDN and CZ drafted the manuscript. DS and LB did the ultrasound and processed images. GDL contributed to the conception of the work. EB critically revised the article for relevant intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.