Article Text

Abstract
Blood culture is one of the most important diagnostic tests in medicine, considering the significant morbidity and mortality associated with bloodstream infection (BSI). However, it is an often misused and misinterpreted test in everyday paediatric practice. In this article, we explore the evidence related to paediatric blood cultures, with the aim of providing clear and clinically-relevant recommendations for its judicious use.
- microbiology
- neonatology
Statistics from Altmetric.com
Introduction
Blood culture (BC) is routinely performed in the assessment of children with fever; however, there remains considerable ambiguity as to best practice for optimal timing, adequate blood volume and correct interpretation of results.1
With increasing global antimicrobial resistance, it has never been more important to better understand the critical role of BC in antimicrobial stewardship by minimising inappropriate antibiotics, reducing length of hospital stay, improving patient safety and preserving existing antibiotics for future generations.2
In this article, we will follow the BC journey from the patient’s bedside to the microbiology laboratory and back. Our aim is to provide a pragmatic guide to aid clinician understanding, focus rationale for performing and assist in the interpretation of results.
Laboratory functions are grouped into three phases:3
Preanalytical phase: time from when a test is performed to when it arrives in the laboratory.
Analytical phase: handling and analysis of the sample.
Postanalytical: what happens after a result is obtained, including reporting.
Preanalytical phase
Case 1: A previously well 3-year-old boy attends the emergency department with a 2-day history of fever (38°C) and an erythematous tender rash on his right thigh. The working diagnosis is moderate cellulitis and you plan to prescribe oral antibiotics. You wonder, should I send a BC?
Diagnostic stewardship: testing the right patients for the right reasons
Before obtaining a BC, it is crucial to establish the pretest probability of bloodstream infection (BSI).3 Selecting patients with reasonable suspicion of BSI improves diagnostic yield4 and helps when interpreting the significance of a positive culture. If you do not suspect BSI, do not send a BC.5
This is especially important, given that multiple studies have found the majority of positive paediatric BCs are contaminants.6 When obtaining a BC, careful skin preparation and aseptic technique is vital to reduce the risk of contamination with skin commensals.7
When to perform a BC can be perceived as an unclear issue for clinicians. In essence, it is important to consider
The clinical presentation and severity of condition.
Probable source of infection.
Medical history.
Relevant risk factors for the development of BSI.
If there is a clinical impression of mild infection and low probability of BSI, performing a BC is rarely indicated. The British Society for Antimicrobial Chemotherapy has recently published detailed clinical pathways for common paediatric infections. These provide evidence-based, focused guidance on presenting features, diagnostics, interpretation of investigations and management advice. Clinicians caring for children in any healthcare setting should familiarise themselves with these pathways, which promote sage diagnostic and antimicrobial stewardship principles.8
Invasive bacterial infection (IBI) is very rare in previously well children, and two-thirds of community-acquired infections occur in children with pre-existing comorbidity.9 BSI is often secondary to focal infection at another site, rather than a primary intravascular infection. However, this can occur and is more common in neonates and neutropenic patients.2
BC is extremely low-yield in uncomplicated community-acquired pneumonia and soft tissue infections.10 Furthermore, isolated pathogens in these infections are often susceptible to first-line antibiotics, meaning empiric antibiotic treatment is generally most appropriate. No single temperature threshold is adequately sensitive to exclude IBI and forego diagnostic evaluation. When determining pretest probability of BSI, height of fever should be considered in the wider clinical context, rather than in isolation.11 Later in the article, we review risk factors and clinical predictors of BSI; these can be used as a guide to determine which children should have BCs sent.
Anaerobic BCs
Anaerobic bacteria are typically fastidious, slow-growing and difficult to culture. Anaerobic BSI is significantly less common in previously well children, compared with the adult population.2 The practice of obtaining routine anaerobic BC remains contentious, and there is broad variation in practices among paediatric centres globally. Current Infectious Diseases Society of America guidelines recommend obtaining both aerobic and anaerobic BCsfor adult and paediatric patients with suspected BSI or septic shock.12
Many of the common commercial BC detection systems (eg, BacT/Alert (BioMérieux) or BACTEC (Becton Dickson)) can provide suitable environmental and nutritional conditions for the growth and detection of some of the more common, clinically relevant anaerobic micro-organisms, in addition to aerobic and some fungal species. For this reason, many paediatric centres advise a more pragmatic approach to a small-volume paediatric blood sample, which involves preferentially inoculating one aerobic BC bottle. Nevertheless, many of these centres do promote the judicious use of separate anaerobic BC in paediatric patients at higher risk of invasive anaerobic infection. These include immunocompromised children, those with head and neck, intra-abdominal or pelvic infections, or severe sepsis.2 12
Case 2: A 5-day-old preterm baby has new temperature instability and feed intolerance. You are concerned about necrotising enterocolitis. You obtain 1.5 mL of blood and wonder: what volume is sufficient for BC?
BC volume: you just can’t get enough!
Due to the inherent difficulty of paediatric venepuncture, BCs are frequently sent alongside cannulation ‘just in case’. Likewise, in a febrile child that may need BC sent (based on clinical progress or inflammatory markers), they are often sent pragmatically to avoid repeated venepuncture. Unfortunately, this means cultures are often inoculated with small volumes, and a negative culture is practically inevitable in a significant proportion.13
Numerous factors contribute to BC sensitivity, including
Blood volume.
BSI periodicity (transient, intermittent or continuous).
Causative organism.
Bacteria density in the bloodstream.14 15
However, it is widely accepted that blood volume is the single most important factor1 and the main variable determining BC sensitivity and specificity.16 In the adult population, each additional millilitre of blood cultured has been associated with an almost 3% increase in microbial yield.17 Increased BC yield with larger volumes has also been observed in children, with one study reporting an increase from approximately 2% among cultures inoculated with ≤1 mL, up to >6% among cultures with >4 mL.18
Obtaining a larger volume not only increases probability of detecting a pathogen but also inversely correlates with bacterial time to detection.14 Volumes of <0.5 mL especially reduce culture sensitivity for fastidious organisms, such as Haemophilus influenzae, Streptococcus pneumoniae and Neisseria meningitidis.1 Additionally, risk of contamination and false-negative cultures are elevated by inadequate blood volume.19
BC volume should be proportional to the child’s total blood volume and weight. While there remains no absolute consensus, and established practice often involves obtaining much lower volumes than BC manufacturer recommendations, the minimum BC volume we should aim to collect is the child’s age in millilitre, with special consideration for very small babies, where no more than 4% of total blood volume should be collected.4 Our suggested minimum volumes are as follows.
Suggested minimum BC volumes dependent on patient age and weight
<1 kg: ~0.5 mL,<5 kg: 0.5–1 mL, <1 year: 1 mL, 2–5 years: - 2–5 mL, 5–16 years: 5–15 mL
Case 3: A 6-year-old girl is being treated for pyelonephritis. She has been on intravenous antibiotics for 2 days but remains febrile (>39°C). Her BC on admission (prior to antibiotics) is sterile to date. She is due for further blood tests, and you wonder: should I send a repeat BC?
The best time to culture for BSI is ‘as early as possible’ in the febrile illness,13 with sample collection guided by patient acuity and necessity to commence antibiotics.2 20
In children already receiving antibiotics, there is considerably reduced detection of bacteria by culture and, to a lesser extent, by nucleic acid detection methods.21 Several studies show that antibiotics prior to BC sampling decreases the rate of culture positivity by 45%–50%.17 22 In any child already receiving antibiotics, BC should be obtained immediately prior to an antibiotic dose, when antibiotic concentration will be at its lowest.2
A common paediatric practice is to obtain BC during or immediately following fever, in the hopes of increasing diagnostic yield. However, research has demonstrated that fever has no influence on the likelihood of obtaining a positive result.22
Analytical phase
In the UK and Ireland, it is routine to use a fully automated and continuously monitored commercial system to process BC. A blood:broth ratio of 1:15 is essential to inhibit the antibacterial effects of normal blood.23 Given the acknowledged challenges of paediatric venepuncture, this requirement suggests that many paediatric samples may have a suboptimal ratio and may contribute to a false negative. Additionally, exponential growth within the BC media means that contamination with just one bacterial colony can result in a false positive.
Samples should be loaded within a maximum of 4 hours to ensure optimal growth. The importance of this practice is highlighted by a neonatal study, which found that mean total time to positivity (TTP) (time from BC inoculation to positive culture), for all isolated organisms at all concentrations, was significantly increased with increasing delay in BC entry into an automated system.24 A temperature of 35°C–37°C for 5–7 days is recommended. If a slow-growing organism is suspected, the incubation time should be increased, and it is vital that clinical teams provide this information.
The automated system continuously agitates, incubates and monitors the BC bottle. A sensor at the base of the bottle detects hydrogen ions generated from the reaction of water and carbon dioxide, which is produced by growing organisms. This results in a colour change in the indicator contained in the sensor. An optical sensor monitors this change and will flag the bottle as positive once one or more criteria are met:
Acceleration of CO2 production.
The rate of CO2 production exceeds a predetermined threshold.
Initial CO2 concentration is above a preset value.
A positive bottle will then be removed from the system and gram stain, along with subculturing, performed.
Gram staining
This test allows classification of bacteria based on the constituents of the cell wall. The morphology of the bacteria is also used to help with further identification. A sample of blood from a positive BC is mixed with saline and streaked on a microscope slide. It is then dried on a heat plate and stained using the Gram stain method. The slide is examined by microscopy and categorised by the organism’s ability to retain the stain.
Gram-positive organisms will appear violet as they have a thick layer of peptidoglycan in the cell wall allowing retention of the crystal violet stain.
Gram negative organisms possess a thin layer of peptidoglycan between two membranes and cannot retain crystal violet. As a result, they are stained pink by a fuchsin counterstain.
Postanalytical phase
Case 4a: A 1-year-old boy is admitted with fever (38°C) and poor oral intake. The presumptive diagnosis is a viral upper respiratory tract infection. On day 2 of admission, he is well and afebrile, but remains on intravenous antibiotics. At handover, you ask whether a negative BC excludes BSI and, if not, why it is common practice to wait 48 hours before stopping intravenous antibiotics?
A negative BC does not always exclude BSI, especially if a small inoculum was obtained. In any child with high pretest probability and negative BC to date, and particularly in those with suspected sepsis, it is worth considering repeat culture and targeted PCR testing; such as for meningococcus, pneumococcus and group B Streptococcus in neonates.
Waiting until 48 hours to stop antibiotic therapy in all children is an outdated approach. Research shows that 90% of bacteria will have grown by 24 hours and 95% by 36 hours.25 In children with low BSI suspicion, stopping antibiotics at 24–36 hours with good safety-netting advice avoids unnecessary hospitalisation without jeopardising patient safety.4
Case 4b: Later that day, the microbiology registrar informs you that this patient has grown Gram-positive cocci in clusters/clumps, from an aerobic peripheral BC at 32 hours. You review the child, who remains well and afebrile, and ask the consultant, what is the significance of this positive BC?
Species Identification & Clinical Implication
Few micro-organisms are unequivocal pathogens, and the significance of any positive culture should be interpreted in the context of the clinical scenario. Several questions should be considered:
1. What is the TTP?
2. Is it a pure culture or mixed growth?
3. Is the micro-organism isolated on more than one occasion (persistent positive culture)?
4. Is the organism a common commensal (could it represent contamination)?
5. Does the presence of this organism fit with the clinical picture?2
It is important to note that TTP is inversely proportional to the bacterial density in blood, with infected blood typically having a higher concentration of bacteria than contaminated blood.26 As such, any culture yielding growth within a short duration has a higher probability of being a true pathogen.27
Factors indicative of true BSI include suggestive history and clinical examination, shorter TTP, risk factors for BSI (See table 1), fever and raised inflammatory markers.28
Bloodstream infection risk factors35
A suggested approach to positive BC interpretation is demonstrated in figure 1, with common paediatric species summarised.

Holistic approach to positive blood culture interpretation. BSI, bloodstream infection; HACEK, Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella species, PMHx, past medical history.
Contaminants
Contaminants create diagnostic conundrum and lead to unnecessary antibiotics. They expose children to antibiotic side effects, contribute to the selection of antibiotic-resistant bacteria and cause distress through repeated cannulation and culture sampling.26 Contaminants also have financial implications, increasing length of hospital stay, laboratory costs and antibiotic duration.29 With any positive BC, if the diagnosis of true BSI is in doubt, an accepted strategy is to obtain repeat samples.18 If multiple BCs are taken and only one is positive, or different bacteria are isolated from repeat culture, this likely represents contamination.
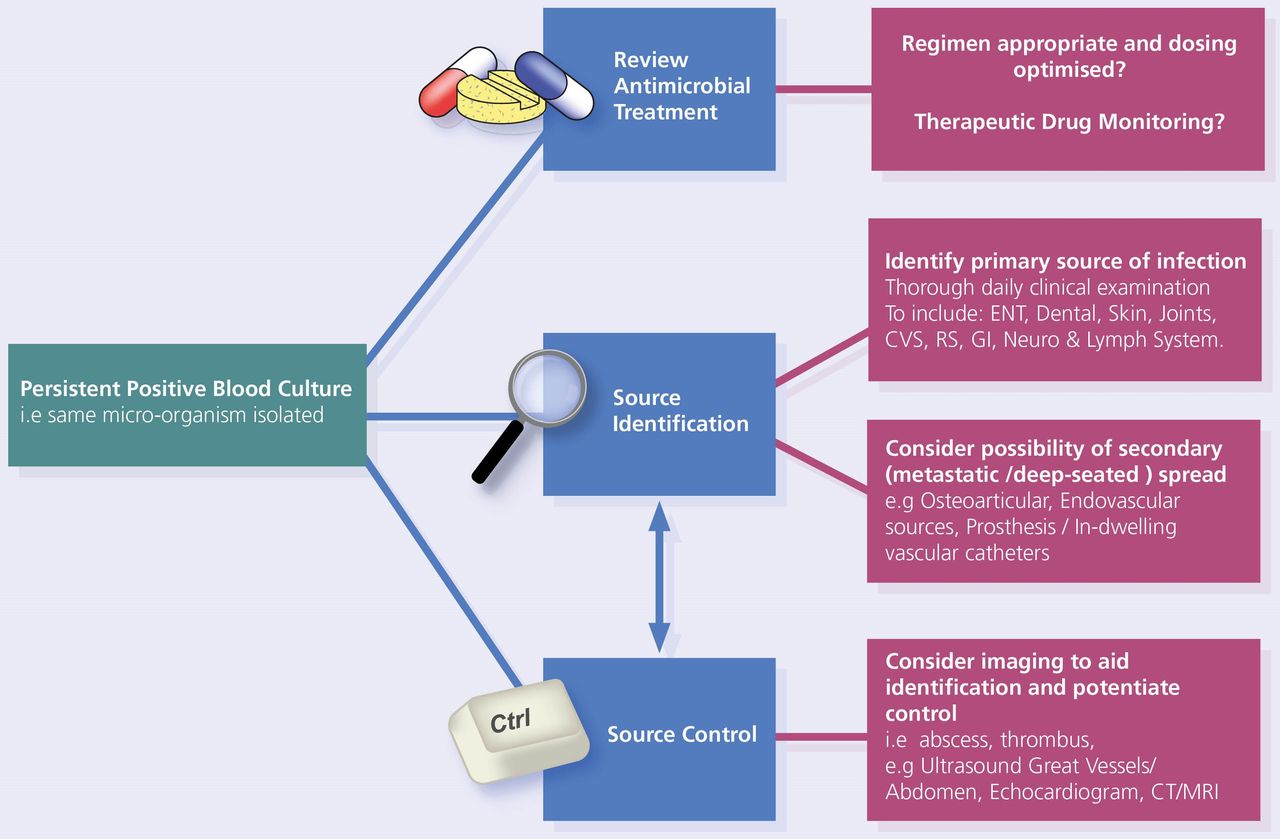
Persistent positive BC
When the same micro-organism is repeatedly isolated from repeat cultures, thorough daily clinical re-evaluation is warranted. There must be active attempts for source identification and concerted efforts to achieve source control. A suggested approach is provided in figure 2.

{kind=link}
{kind=link}
Suggested approach to persistent bacteraemia. ENT, ears, nose and throat; CVS, cardiovascular system; RS, respiratory system; GI; gastrointestinal.
Pathogens
Modern automated BC systems are highly effective at identifying the most prevalent bacterial bloodstream pathogens. The most common pathogens, categorised according to age, are summarised in table 2. Importantly, Staphylococcus aureus, Candida spp. and Gram-negative bacilli isolated from BC are predominantly significant organisms, and very careful consideration should be given before discounting these as contaminants.27 28
Common bloodstream infection pathogens in children1
Case 5: A 9-year-old boy, with background of previous cardiac surgery, presents with a 6-week history of malaise, night sweats and intermittent fever (38°C). The clinical suspicion is subacute bacterial endocarditis (SBE). The infectious diseases team recommend taking three sets of appropriate-volume (~10 mL) peripheral BCs over the next 24 hours. You consider which organisms are particularly difficult to detect on BC?
Pathogen identification
Where there is a clinical suspicion of SBE, international guidelines recommend at least three BC sets should be collected, each containing 10 mL of blood, with samples incubated in both aerobic and anaerobic culture bottles. Particularly in stable patients with clinical suspicion of SBE, antibiotics should be withheld and cultures obtained prior to antibiotic administration to maximise likelihood of identifying a causative organism. Once an organism is identified, BC should be repeated 48–72 hours after starting antibiotics to assess the effectiveness of treatment.30
Traditionally, growth characteristics and a range of biochemical tests were used to identify the species of bacteria cultured. Matrix assisted laser desorption/ionisation time of flight is a semiautomated form of mass spectrometry which allows rapid identification of cultured organisms, following detection of growth in BC. This has revolutionised laboratory identification methods.2 It has also been shown to be cost effective and to shorten the time until appropriate antibiotic therapy in paediatric inpatients.31 This assay can, however, misidentify uncommon and fastidious organisms, and results should be analysed in conjunction with the clinical presentation.32
Bacterial identification directly from positive BC bottles by PCR is also becoming increasingly available, with systems such as the FilmArray Blood Culture Identification Panel (Biomerieux). Early micro-organism identification can highlight likely contaminants and allows rapid antibiotic rationalisation. This helps to reduce the use of broad-spectrum antibiotics, improves antibiotic stewardship and can facilitate earlier discharge from hospital.33
Fastidious organisms require different growth media, temperatures and atmospheric conditions compared with those routinely used to culture organisms. For example, Haemophilus spp. (which can cause SBE) require two additional growth factors to aid culture. This once again reiterates the importance of providing comprehensive clinical information, including the suspicion of SBE, when requesting BCs.
Typically, it takes 24–48 hours from detecting a positive BC to ascertaining antibiotic susceptibility. Antimicrobial sensitivity testing is performed using standardised antibiotic impregnated discs and automated broth microdilution systems, which analyse the minimum concentration of an antibiotic required to inhibit growth.
Novel identification methods: bacterial 16S PCR
If BC has not yielded a pathogen and BSI is strongly suspected, 16S PCR testing can be performed. All bacterial ribosomes have a highly conserved 16S subunit with variable regions specific to different species. Using 16S PCR and DNA sequencing, any bacterial DNA in the sample can be amplified and help identify the genus and species. This is particularly useful in culture-negative endocarditis and can be applied to any sterile sample that has not been cultured an organism.34 However, availability of this method is predominantly limited to reference laboratories. Additionally, any 16S PCR result must be interpreted within the clinical context, as any bacterial cellular material will be detected, including sample contaminants.
Areas for further research
Rapid identification and sensitivity testing for cultured organisms is an area of ongoing research. In the future, this will help to guide clinical decision-making in real time.
Clinical bottom line
(See online supplemental infographic)
Supplemental material
Judicious use of BC should always be employed. Consider both diagnostic stewardship and pretest probability of BSI, alongside clinical assessment.
Numerous factors impact on BC sensitivity, but adequate blood volume is of utmost importance.
When interpreting a positive BC, adopt a holistic approach. Always ask, does this fit with the clinical picture?
In persistent positive BC, or where there is clinical concern, seek early advice from microbiology and infectious diseases specialists. Review the antimicrobial treatment and consider source identification and control.
When pretest probability of BSI is high but no organism is cultured, consider 16S PCR testing. This can detect fastidious organisms, which can clinch an undiagnosed clinical syndrome.
Ethics statements
Acknowledgments
The team acknowledges colleagues in clinical microbiology and paediatrics within Royal Group of Hospitals. The authors thank Joseph Kelly and the medical illustrations team in Royal Victoria Hospital. Additionally, we thank Nathan Warnock for designing the article infographic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SimEdRBHSC
Contributors PMa conceived the idea of update on the earlier version. SOH and PMa drafted and revised serial manuscript versions. PN provided microbiology expertise and edited the manuscript. LS and PMo reviewed and edited the manuscript. All contributed to the final review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.