Article Text

Abstract
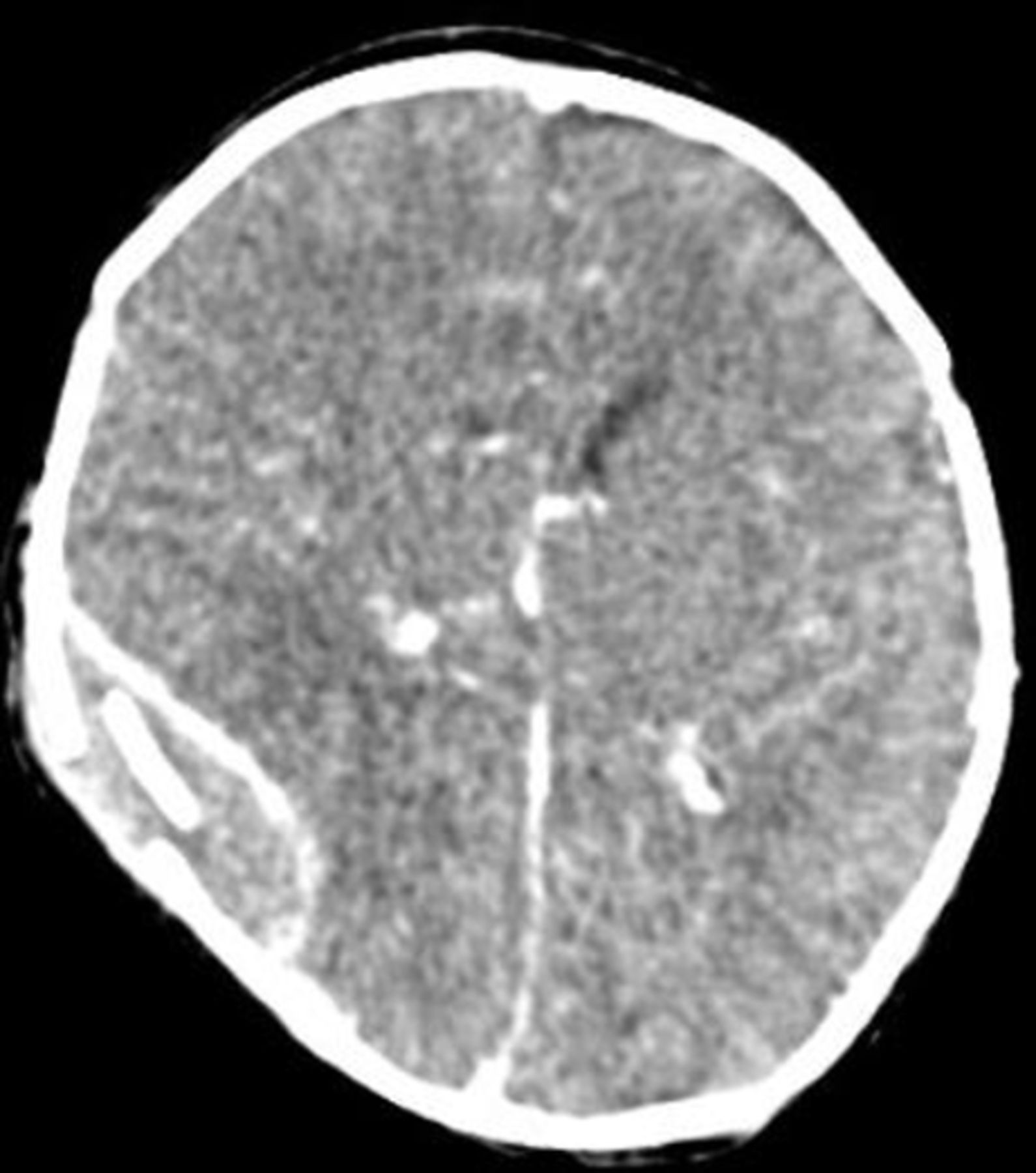
A baby boy was born at term by spontaneous vaginal delivery to non-consanguineous parents following an unremarkable pregnancy. He was admitted to his local neonatal intensive care unit shortly after birth following several episodes of eye-rolling, colour change and apnoea. He had bilateral parieto-occipital cephalohaematomata, scattered petechiae and intermittent hypotonia. He was otherwise neurologically normal. A septic screen was completed and antibiotics and aciclovir were given. Cranial ultrasound, cerebral function monitoring and electroencephalography were normal. An echocardiogram demonstrated normal function and intracardiac anatomy but was suspicious for a dysplastic aortic arch and anomalous left pulmonary artery–aorta connection thus he was transferred to the regional paediatric cardiology centre where cardiac CT (figure 1) was undertaken. CT brain (figure 2) was performed simultaneously to delineate the cerebral vascular anatomy but demonstrated an intracranial lesion that accounted for the baby’s presentation.

{kind=link}
{kind=link}
Questions
What diagnosis was confirmed by cardiac CT?
Scimitar syndrome
Partial anomalous pulmonary venous drainage
Major aortopulmonary collateral arteries
Neonatal pulmonary embolus
Arterial tortuosity syndrome
What is the inheritance pattern of this condition?
Sporadic
Autosomal dominant with high penetrance
Autosomal dominant with low penetrance
Autosomal recessive
X linked
Which of these features is not associated with this diagnosis?
Increased risk of stroke
Pulmonary artery stenosis
Abdominal ascites
Joint hypermobility
Facial dysmorphia
What abnormality is demonstrated on CT brain?
Neonatal stroke
Subdural haematoma
Normal cranial sutures
Extradural haematoma
Ruptured intracranial dermoid cyst
Questions Answers can be found on page 02.
- Neonatology
- Congenital abnormalities
- Vascular
- Imaging
- Cardiology
Statistics from Altmetric.com
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.