Article Text

Abstract
The Bayley Scales of Infant and Toddler Development—Third Edition (Bayley-III) is a gold standard series of behavioural assessments used by clinicians and researchers to assess the developmental functioning of young children. The rigorous psychometric properties of the tool are attributed to the carefully standardised normative sample and quantitative scoring system. It is a common end-point assessment used in neonatal trials and is routinely used in a clinical setting to assess the development of children at risk of delay. Incidence of developmental delay is higher in clinical populations such as those born preterm or with complications such as neonatal encephalopathy. Early identification of delay is critical as early intervention is most effective in minimising impairment; therefore, routine assessment of developmental outcomes is recommended, particularly among high-risk populations.
- neurodevelopment
- child psychology
Statistics from Altmetric.com
Introduction
Developmental delay affects approximately 15% of children worldwide.1 It occurs most commonly in clinical populations such as children who experience difficulties during the prenatal period, neonatal period or early infancy.2 Early identification of developmental delay is critical as early intervention is likely to be the most effective in decreasing impairment. Careful evaluation of the strengths and weaknesses of a child’s development is recommended in order to identify areas where support may be required.
The Bayley Scales of Infant and Toddler Development—Third Edition3 (Bayley-III) is one of the most widely used standardised tools for the assessment of neurodevelopment in early childhood. This paper aims to outline indications for the use of the Bayley-III in comparison with other commonly used tools for the assessment of developmental outcomes in children. It discusses the value of the Bayley-III and some of its limitations.
Background
Applicable to children aged 1 month to 42 months, the Bayley-III uses a series of play tasks and parent report questionnaires to assess the child’s level of functioning across various developmental domains, including cognitive, language, motor, social-emotional development and adaptive behaviour. The language and motor scales are divided into further subscales: the language scale assesses receptive and expressive language abilities, and the motor scale assesses both fine and gross motor skills (see figure 1).
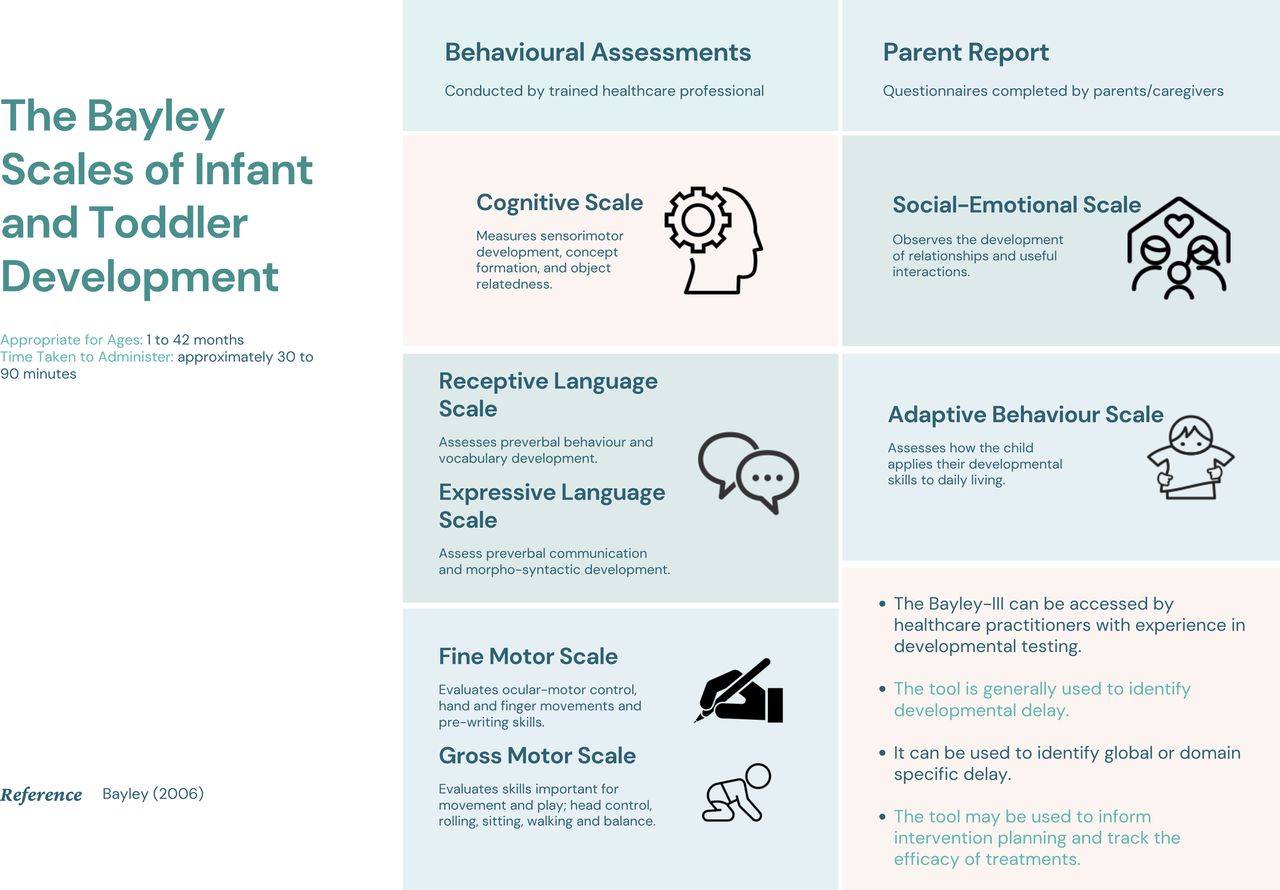
Summary information for using the Bayley Scales of Infant and Toddler Development – Third Edition.
The Bayley-III is an ability test of global development. Cognitive, language and motor domains are conducted through behavioural assessment while social-emotional and adaptive behaviours are assessed through parent report. The play tasks take approximately 1 hour to conduct with young infants and up to 1.5 hours with toddlers and preschoolers (see box 1). Each behavioural domain may take up to half an hour to complete, commencing with simpler tasks and increasing in difficulty until tasks are beyond the expected capabilities of the child.
Examples of tasks administered during a Bayley Scales of Infant and Toddler Development—Third Edition assessment3
Cognitive scale: the examiner will initiate tasks such as placing block set shapes into the puzzle board or providing toys to facilitate representational play. For example, the child pretends a red block is a bar of soap used to wash the doll.
Receptive language scale: the child is shown pictures from the stimuli book and is asked to identify the ‘shoes’ or ‘ball’ from a series of pictures.
Expressive language scale: the examiner observes babbling, gesturing and vocabulary development such as naming objects, pictures, sentence formation, plurals and verb comprehension.
Fine motor scale: the child will be asked to imitate tasks such as posting coins into a piggy bank, block stacking, using scissors or lacing a card with a shoelace.
Gross motor scale: the examiner will ask the child to copy his or her actions as they model different positions and actions, such as running, ascending/descending steps and kicking a ball.
See figure 2 for examples of materials.

{kind=link}
{kind=link}
Examples of materials.
Individuals who intend to administer the Bayley must receive training and have experience in developmental assessment and interpretation. Training is administered through the manual and can be demonstrated by individuals who are familiar with the assessment. Healthcare professionals typically trained in carrying out the assessment include:
Clinical psychologists.
Occupational therapists.
Research staff.
Domain-specific specialists:
Physiotherapists.
Speech and language therapists.
And less frequently:
Paediatricians.
Neonatologists.
What factors need to be considered when choosing an appropriate developmental assessment for children at risk for developmental delay?
A number of developmental assessments are available to establish a child’s global developmental profile and should be selected for use as appropriate based on the needs of the patient and the practitioner (See table 1). Each developmental assessment is designed to assess a variety of core developmental outcomes such as cognitive, language and motor development. Assessments are administered through behavioural assessment or parent report. While behavioural assessments are laborious, potential biases of parent report must be considered when selecting an appropriate tool. Practical aspects to be considered include:
A comparison of Bayley Scales of Infant and Toddler Development – Third Edition and other standardised measures of child development
The age of the child.
The time required to complete the assessment.
Whether a comprehensive assessment of abilities or a screening test is required to direct treatment and intervention.
While the Bayley scales have been used to advise on a number of the National Institute for Health and Care Excellence (NICE) Guidelines,4 advice for clinicians and researchers on the choice of developmental assessment tools is often inconsistent or, in some cases, non-existent.5 6 The measurement of developmental outcomes in children varies widely among researchers and clinicians as these outcomes are based on the use of differing tools and measures. Reports often fail to detail how, when, where and by whom developmental outcomes are measured, so do not contribute to the standardisation of care.7 The development of a ‘Core Outcome Set’ may be beneficial for those at-risk of developmental delay.
When should the Bayley-III assessment be considered and how does this compare with other common tools?
The Bayley-III is commonly used to identify developmental delay in clinical groups and high-risk children by comparing the abilities of the child to a normative age-matched sample of children (see box 2 for list of indications). Furthermore, the assessment tool can be used to track the impact of intervention on development. In research, the Bayley is often used as an end-point assessment for neonatal randomised controlled trials and is used to draw conclusions regarding the efficacy of treatment or intervention.8 It is not designed to diagnose clinical conditions or to be used as a measure of intelligence.
Clinical indications for the Bayley Scales of Infant and Toddler Development3
Prenatal complications and congenital disorders
Congenital brain malformation.
Congenital anomalies.
Neonatal complications
Preterm birth.
Neonatal encephalopathy.
Neurodevelopmental disorders
Pervasive developmental disorder.
Cerebral palsy.
The Bayley-III is most directly comparable with the Griffiths Scales of Child Development-III9 and the Mullen Scales of Early Learning;10 however, there are important differences. The Mullen Scales of Early Learning is an abilities test commonly used in research that yields measures of cognitive, language and motor abilities rather than assessing for developmental delay. The Griffiths Scales of Child Development-III is a behavioural assessment for children 0–8 years of age. The Griffiths Scales can only be administered by holders of a Certificate of Registration as User from the Association for Research in Infant and Child Development, whereas the Bayley-III can be used by anyone with experience in developmental testing.
Each domain of the Bayley-III has been compared with domain specific assessments to establish the concurrent and predictive validity of the tool. The Bayley-III motor scale and the Peabody Developmental Motor Scales11 were found to be positively correlated and agreement in total scores between assessment tools was 79.17%.12 The language and cognitive scales correlate with verbal IQ (0.71–0.83) and full scale IQ (0.72–0.79) on the Wechsler Preschool and Primary Scale of Intelligence13 administered in later childhood. One advantage of the Bayley-III is that it can be used to assess either global or domain specific delay for example, if only motor or language domains require assessment.
In 2019, Pearson announced the release of the fourth edition of the Bayley assessment.14 The Bayley-4 has updated the normative sample against US norms. It has been revised to increase the sensitivity of the assessment and simplify administration procedures by:
Reducing administration time.
Facilitating digitised administration.
Introducing a polytomous scale, allowing a score of 2, 1 or 0 depending on the quality of mastery.
Bayley-4 is currently undergoing standardisation projects within the UK, Ireland and Australia and can be used once these normative samples are established.
How do you interpret the scores from the assessment and how do you manage a child with a score indicating developmental delay?
A composite score for Bayley-III is calculated for cognitive, language and motor scales (see box 3). Scores within the bottom 10th percentile signify developmental delay; children who score within this range require further examination from the healthcare team.15 Each domain is scored separately allowing specialist or multidisciplinary healthcare teams to be involved in intervention planning and implementation. Once intervention is initiated, the Bayley can be readministered and the growth chart can be used over periodic assessments to track the development of the child and the effectiveness of the intervention programme.
The interpretation of scores
The composite score for Bayley-III is calculated based on a comparison of the child to a normative age-matched sample established by the assessment. A composite score is calculated for the cognitive scale, language scales and motor scales and are interpreted as follows15:
100 (SD=15) Standardised mean score 50th percentile: mid average functioning.
<85 = (1 SD below the mean) 16th percentile: indicates mild impairment/at ‘risk’ of developmental delay – needs to be monitored/advice to parents on techniques to improve development/referral to therapist depending on degree of impairment.
<70 = (2 SD below the mean) second percentile: indicates moderate/severe impairment requiring early intervention team input.
What are the limitations of the Bayley-III and how can the accuracy of the assessment be assured?
The Bayley-III is often criticised for its lengthy administration time; it may be difficult for children to attend to activity for this amount of time, and families may find it difficult to schedule in time. Limited availability of staff and appropriate consultation space in hospital units are common issues cited. It is suggested that children at risk of developmental delay could complete a screening questionnaire such as the Ages and Stages Questionnaire as outlined in the NICE Guidelines5 before suggesting referral for the Bayley assessment.
The Bayley-III has been considered a relatively blunt measure as it assesses each developmental domain globally. Thus, subset abilities and subtle deficits may be missed within specific scales. Compared with its predecessor Bayley-II, children score significantly higher on the Bayley-III. The Bayley-III has been found to inflate scores in typically developing children and underestimate developmental delay. This inflation is partially accounted for by inconsistencies in the normative sample as well as inaccurate administration of the tool.16
Precise referencing to the manual is important when carrying out the Bayley-III, including administration and scoring procedures. The position of the child is outlined for each task, whether requiring seated, supine or standing position. Language should be chosen carefully while instructing, and awareness of body language is required to ensure the examiner is not inadvertently prompting the child. The examiner is required to make accommodations for children with known impairments such as physical or language difficulties. Flexibility during assessment may be required to elicit a representative performance. The assessment should be conducted in a clean, quiet and well-lit room, free from distractions such as additional toys and decorations. A maximum of three adults can be present during assessment including the examiner and parent/caregiver. The caregiver is instructed to be encouraging but not to interfere with their child’s performance.
Clinical bottom line
The Bayley Scales of Infant and Toddler Development is a gold standard tool that assesses cognitive, language, motor, social-emotional development and adaptive behaviour in children aged 1–42 months.
The assessment takes approximately 30–90 min to complete. It is used to identify developmental delay and can be used to track the impact of intervention on development.
Examiners carrying out the assessment must be adequately trained to do so. The tool is accessible to individuals with experience in developmental testing.
Due to the lengthy administration time, a screening questionnaire such as the Ages and Stages Questionnaire17 is recommended before referral for a Bayley assessment.
References
Footnotes
Twitter @MolloyElesean
Contributors EJM conceived the idea for the work. CDR, JQ and EN initially drafted the manuscript, and all authors provided critical revisions of the work. All authors approved final version of work for submission and agree to be accountable for all aspects of the work.
Funding This study was funded by Health Research Board.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.