Article Text

Abstract
There have been rising concerns in the UK about the levels of serious violence between young people, especially serious physical violence and knife crime. Interactions with young people in the emergency department (ED) at the time of injury provide an opportunity for screening and intervention in order to reduce the risk of repeat attendances. However, paediatricians and other healthcare workers can feel unsure about the best way to intervene. Embedding youth workers in EDs has started in some UK hospitals, making use of a potential ‘teachable moment’ in the immediate aftermath of an event to help change behaviour. Based on a rapid review of the literature, we summarise the evidence for these types of interventions and present two practice examples. Finally, we discuss how EDs could approach the embedding of youth workers within their department and considerations required for this.
- accident & emergency
- adolescent health
- general paediatrics
- health services research
- multidisciplinary team care
Statistics from Altmetric.com
- accident & emergency
- adolescent health
- general paediatrics
- health services research
- multidisciplinary team care
Youth violence attendances in the emergency department (ED)
A possible increase in serious youth violence has been a major news story in recent years. In most cases, serious youth violence is defined as murder, knife and gun crimes and serious physical violence or threat of it by young people aged up to 25 years. The Local Government Association,1 Lord Mayor of London2 and Department of Health and Social Care3 all advocate for a ‘public health’ model to tackle the problem, looking at root causes and addressing drivers of violence, rather than taking a purely criminal justice-based punitive approach.
Statistics suggest that levels of violent injury among young people in London, for example, appear to have remained constant or to have risen in recent years. There were 5053 finished consultant episodes recorded in English hospitals in 2017/2018 due to assault by a sharp object. This was an increase of 14% compared with 2016/2017 and 39% higher than in 2014/2015, and 19% of the 2017/2018 incidents involved those young people who were under 19 years.4
Historically in the UK, prevention of youth violence has been left to outside the hospital with community and police interventions, although healthcare professions in the ED setting are well aware of relatively high reattendance rates in violent injuries5 and programmes addressing this have been established in some parts of North America since at least the 1990s. Anecdotally, healthcare workers can feel overwhelmed and uncertain about the best approach to young people they see who have been victims or perpetrators of violence and other criminal activity. It is not a routine part of training, particularly in UK paediatrics, and many members of the team feel out of their depth in handling such complex issues.
Although part of the solution may lie in improved training, another possibility lies in the introduction of other kinds of professionals into the team who may bring complementary skills in youth engagement and violence prevention. As a result, there has been increasing interest in the potential role of youth workers in EDs in recent years, working specifically with young people around the time of entry to the department. Most of these models include both some kind of contact at the point of entry to the hospital (the ‘teachable moment’) and longer-term efforts to network the young people into other kinds of community-based support to help reduce recidivism. However, as we will see, the range of interventions using ED as the springboard to tackle this is very diverse across both the type of intervention and who delivers it.
Much current UK interest is in the application of the teachable moment model, often through youth workers, to reduce repeated incidents of violence (recidivism) among young people arriving at the ED. We wanted to explore the evidence related to this model and undertook a rapid review of the literature, and explored some existing models of delivering interventions based on the teachable moment. We have done this with paediatricians in the ED in mind, to enable informed discussion on what programmes may already exist for young people and what the evidence base for these is, but the issue is a broader one about expanding the ED’s connections to providers in the local community and making the most of other professionals with particular expertise in delivering services to young people.
Evidence for basing youth violence interventions on a teachable moment
A teachable moment has been described as ‘a naturally occurring life transition or health events thought to motivate individuals to spontaneously adopt risk-reducing health behaviours’.6 In theory, this moment provides a ‘window' for delivery of a brief intervention which may have more impact because the events that have just happened may make the individual more open to change. In the review, we focused on understanding the kinds of models used, particularly those based on a teachable moment and using youth workers for delivery, and also looked for evidence on their impact on youth outcomes.
Using the search terms ‘teachable moment’ AND variations on ‘young person’ in PubMed, MEDLINE and Embase and ‘youth worker’ AND variations on ‘Emergency Department’ (searched separately as all four terms together produced minimal results), we located 192 papers. Of these, only 30 related to youth. Some further papers were found through ‘snowballing’, reviewing cited literature, and correspondence with an author. After screening, only 13 papers using empirical evidence of ED programmes were found. These included eight randomised controlled trials and some case–control or cohort studies, the majority undertaken in the USA. UK literature currently provides no empirical evidence on outcomes gathered in the UK context, though papers do exist providing descriptive data on uptake of services, ED usage after violent assault and making the case for the use of youth workers with description of barriers to usage.7 A North London project was described in conference abstracts.8 Table 1 presents more details on the studies included.
Studies included in the rapid review (overall, 13 papers were included in the review)
The first finding was that the use of the construct of the teachable moment is not very consistent. An earlier 2009 review concluded that there were three ways in which the term was used. First, the term is used colloquially, simply meaning any ‘opportunity for change’. Second, it is used to denote general opportunities associated with a distinct moment in life, such as admission for a heart attack. Third (and more rarely), it can be used in a more academic way to describe the stages of a theoretical model of behavioural change drawing on health beliefs model and social cognitive theory.9 ,10 11 These more theoretical approaches are related to, for example, the health behaviour model, which is a framework for motivating people to take positive health actions to avoid negative consequences, and the transtheoretical model of change, which suggests there are stages of behaviour change that people move through that can be predicted and influenced accordingly.
Results were not conclusive about impact, but did suggest some emerging evidence for crime reduction and for positive responses from the young people involved. Reduction in attendance at the ED was mixed, with some studies showing reduction in reattendance rates and others showing no difference between groups. No study found harm to patients by being enrolled, and generally, the response to such an intervention was felt to be positive by participants.5 7
Separating the use of the teachable moment itself from a case-based ongoing intervention was not possible from these studies, limiting our ability to determine which bits of the intervention may be responsible for change. It is important to note that we did not find any evidence that specifically tested using the teachable moment of ED admission against other intervention methods.
These results may be a reflection of the lack of evidence quality and quantity rather than a finding of lack of effect, particularly in terms of the UK context. Box 1 summarises the limitations in the evidence base. A wider review, drawing in findings from use of similar kinds of teachable moment interventions in other settings, such as youth justice, may help to shed more light, and more research is warranted on the specific role of youth workers in medical settings.
Data limitations from assessing complex behavioural interventions
The data limitations we found here are not unusual in assessing the impact of complex behavioural interventions on hard-to-reach groups of this age group. The young people being offered these kinds of interventions are usually particularly vulnerable. One London programme found 10% of their referrals were homeless and 27% had an unstable home situations,28 making even basic demographic data difficult to collect. Identifying the appropriate outcomes is also challenging; process measures can be confused with outcome measures, and measures may not give enough time between an intervention programme and the outcome in order to demonstrate impact.
In addition, all studies, even randomised controlled trials (see table 1) were limited by numbers of participants (only one had more than 90 participants in each arm of the trial, and a couple had only 40) and wide CIs. All interventions were slightly different, ranging from a 30 min intervention by computer program17 to a 1-year face-to-face intervention for the whole family,12 reducing comparability. Who delivers these programmes also varies. Briefly trained volunteers to salaried professionals and different approaches to lived experiences also contribute to the diverse mix of available intervention types to study limiting the measurable impact across sites and programmes.
All of the studies included in the literature review suffered from at least one of these potential limitations. It is important to note, however, that there was no evidence that these kinds of projects did harm. As our understanding of complex interventions grows, future studies, codesigned with relevant stakeholders to address a wide issue, should be implemented with a flexible approach to feedback, and evidence gathered as it can be sometimes across years and decades.
Examples of interventions currently in use in EDs
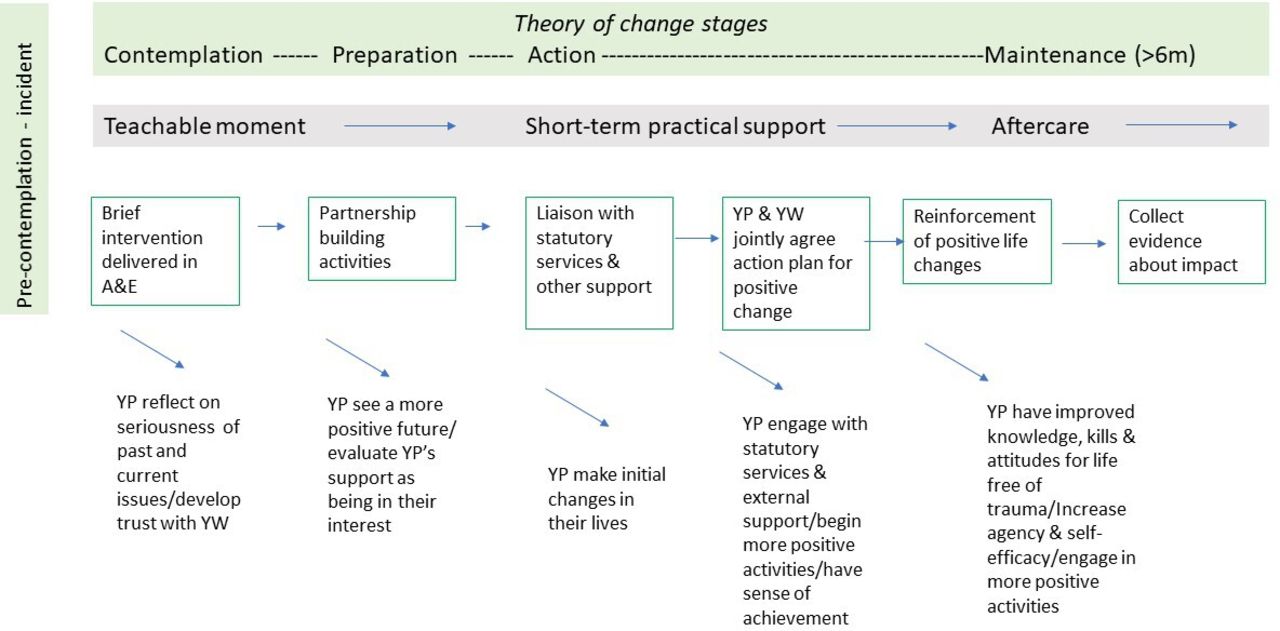
Despite the lack of definitive evidence on impact, hospital-based youth violence intervention programmes are gaining traction. The most widely used model in the UK is run by a charity called Redthread, which is now working in five major trauma departments around the UK and other non-specialist EDs (figure 1). Box 2 presents a case study outlining their work. Others doing similar work in the UK at the time of writing include the St Giles Trust and the Oasis programme.

{kind=link}
Redthread model set in context alongside the stages of the transtheoretical model of change. The five stages of the model of change are precontemplation (not shown, as this would be pretrauma), contemplation (at the moment of arrival at the trauma centre), preparation (including partnership building with the youth worker and development of an action plan) and action (including engagement with other support services and the start of more positive activities) through to maintenance (reduction in risky behaviour several months later). A&E, accident and emergency department; YP, young people; YW, youth worker.
Case study 1: Redthread model, UK
Informed by the frameworks of the health behaviour model and transtheoretical model of change and experience in the field, Redthread, a voluntary sector youth work organisation based in the UK, uses the teachable moment with young peoplepresenting to local trauma centres to reduce the risk of further trauma. Both theoretical frameworks emphasise the importance of developing self-efficacy and of being offered opportunity for change or a prompt for action. Arrival at the accident and emergency department (ED) potentially offers this kind of prompt.
The aim was to enable more engagement with young people at the time of being a victim of an assault to break the cycle of violence and to facilitate referrals to other third sector and statutory agencies.
What happens
The youth worker meets the young person during their time in the ED and starts to establish rapport. After consenting, the youth worker and young person work through the ‘you and your health’ questionnaire, designed by Dr Steph Lamb, providing a basis to establish goals and build an action plan with referrals into local community services who can help to address underlying risk factors. The youth worker remains in contact after discharge and continues to act as a key worker for varied lengths of time, depending on need.
Does it work?
An unpublished evaluation of Redthread’s impact over 3 years at St Mary’s Paddington (2015 and 2017) by NPC Associates found that of those young people who were followed up after 6–12 months (only possible for 117 of 703 referrals), 73% had seen a reduction in their ‘total risk score’ (part of the risk assessment each young person undergoes on consenting to Redthread involvement); 59% had reduced involvement with violence; and 53% reported a reduced involvement in crime. This was among a group of young people who had high risk scores initially, with a large number being involved in violence, crime and reacting violently to situations.28 However, the low take-up of follow-up risk assessments limits the interpretation of these results. A separate exercise to track reattendance rates at the St Mary’s emergency department suggested that the rates fell significantly for those seen by the service. The lack of peer review through using unpublished data limits further interpretation.
As the literature suggested, the model is more common in the USA, and box 3 presents a well-established American model for comparison, which is the National Network of Hospital-based Violence Intervention Programmes. This grew from the work of Youth ALIVE!, a non-profit, public health agency based in Oakland, California, USA, which established one of the first hospital-based violence intervention programmes, Caught in the Crossfire, in 1994.12
Case study 2: Health Alliance for Violence Interventions (HAVI), US group
The HAVI (also known as the National Network of Hospital-Based Violence Intervention Programs (NNHVIP)) is a group of over 30 hospitals in North America with violence intervention programmes, not all targeted at youth. The group collaborates on research and runs a conference to support the evidence base behind these interventions and to help in the development of their strategies.
The individual hospital programmes vary, but all these programmes are based on five core values: community (interventions by those who themselves have been victims of violence; ‘healed people, heal people’); equity, everyone deserves good care; that violence is preventable; there is opportunity for intervention and change provided by injury; and that programmes should care for ‘physical, psychological and emotional wounds’.29
The US Centers for Disease Control and Prevention, which has released guidance alongside the NNHVIP, describes the three key elements to NNHVIP fidelity as ‘1: violent injury serving as teachable moment, 2. culturally competent case management, 3 addressing risks associated with violent injury’.30
What happens
The groups all ‘employ’ either volunteers or paid workers who are specially trained in interventions for young people, some of whom are previous victims or perpetrators themselves. These workers engae with young people who are recovering from violence-related injuries in the ED and provide follow-up for different periods of time, depending on the programme. Services include crisis intervention, case management, linkages to community services and peer mentoring. They may involve the whole family and usually lead to onward referral and liaison with other agencies or third parties (such as education, housing and criminal justice).
As with Redthread, the key is that the ED is used as the stimulus for making a connection between the young person and the youth worker after a violent event in the youth’s life.
Does it work?
There are 28 published works sited, with 15 published since inception in 2009, and only seven clearly relating to youth (as of September 2019). One of the most consistent groups for publishing about youth violence intervention, the Emergency Department Violence Intervention Programme in Winnipeg, which was undertaking extensive research, has recently had its funding cut, and the programme has been suspended. Therefore, robust studies into long-term outcomes continue to be lacking.
Approaches to setting up youth intervention programmes in the ED
The National Network of Hospital-Based Violence Intervention Programs and the American College of Surgeons Trauma committee have both released guidance on how to set up violence intervention programmes in the hospital. They have differences, but their core themes are very similar, and much of the advice applies to any new service introducing non-healthcare professionals into the health environment. These are an essential and useful read for anyone considering youth workers in the ED, and we summarise some main points as follows.
The stages are13 14
Scoping . Find out about your local demographic in the community and who uses your hospital. In addition, assess what relevant services may be available locally for onward referral, including voluntary sector organisations and community projects, local authority social care and other third-party groups. How do these services work?
Define what you want to achieve . What and who is the service for? The clearer the aim, the more likely one is to achieve it as a team.
Get the right people on board . Establish ‘champions’ and advocates in hospital and out.
Establish local ‘buy-in’ from a key member of staff in the ED, managers and the youth workers (usually a collaboration with a local charity) as this helps with set-up, coproduction and engagement from other staff members. Remember the local community and engage with any passionate or helpful voices here.
Find the right external group to collaborate with: Usually third sector groups collaborate with the hospital to use their own youth workers and connections to set up the service. There are charities in UK currently that do this (Redthread, Oasis, St Giles). Whoever one collaborates with, a governance structure is still essential, as well as review of internal workings and understanding accountability and what role is required from a third party.
Work out your ‘programme ’. What will the youth workers do initially? (screening for vulnerabilities and signposting)? Who will have responsibilities for child protection and other such referrals? What happens next, once young people are engaged?
Get it started . Find the right staff; let people know about you; find a space for the team; make and maintain connections with other groups for onward referrals.
Introduce training and education for youth workers about hospital functioning and clinical issues, as well as for clinicians on how best to support their youth work colleagues.
Think about funding and sustainability . Always an issue in the tightly stretched NHS. There are a number of US papers showing the interventions save money if ED visits are reduced, and criminal charges are avoided.15 16 These could help with business planning. Investigate funding sources outside the NHS, such as local foundations or criminal justice funders. Sustainability in terms of funding and staff needs to be considered from the outset.
Plan evaluation . Showing the programme works not only helps sustainability but also adds to empirical data. This requires designing into the programme from the start.
Discussion
Young people who are victims of serious violence are a major concern in EDs. Having youth workers to engage them, similar to the use of specialist Care of Elderly Rapid Assessment Teams, makes sense not only for youth violence but also for a sophisticated and preventative approach to supporting young people to achieve health and well-being.
The use of the teachable moment in EDs, facilitated by youth workers, has provided a model for working with young people in UK EDs that face an increase in presentations associated with violence among youth. The incident bringing the young person to the ED may provide a hook for change, which is true for all sorts of hospital admissions of course, not just for violence. Hospital violence intervention programmes in the USA have provided some initial positive results, and no apparent harmful ones, but a truly robust evidence base for implementation with young people in the UK setting is currently missing, with many factors making evaluation difficult. While this is being established, the balance of evidence supports their continued introduction into EDs as better understanding of complex interventions develops. However, more efforts should be made to improve our understanding of how they work.
Conclusion
Youth workers in hospital is a developing part of ED provision for vulnerable young people who have previously not been well served by paediatric services. The successful embedding of youth workers within the ED team provides opportunities for a public health approach to complex ‘youth problems’, such as violence, drug and alcohol addiction and mental health concerns. Ongoing review and evaluation of these programmes is required to ensure the provision of effective and innovative interventions can be implemented appropriately throughout the system.
Acknowledgments
We are grateful to colleagues working in violence prevention in hospitals for useful conversations during the development of this piece, including Brendan King, Anthony Scott and John Poyton of Redthread, and to Philippa and Nick Chapman at NPC Associates.
References
Footnotes
Twitter @lizziewortley, @AYPHcharity
Contributors EW and AH jointly conceived the paper. EW undertook the literature review and collated the findings. AH undertook communication with practitioners in the field.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Redthread provided a grant to the Association for Young People’s Health (AH) in 2017 to help document their service delivery model. Material from this is used in table 1.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.