Article Text

Abstract
A 13-year-old girl presents to the emergency department for the second time with an unresponsive episode. She has a GCS (Glasgow Coma Scale) score of 11 on arrival and all other observations are normal. The story is unclear, but there are ongoing safeguarding concerns and the family are known to social services. All investigations are normal. After a period of observation on the ward, her GCS returns to normal and she appears well. Both on the first presentation and this presentation ingestion of a toxin was suspected. However, this was denied by the patient and urine toxicology screen was negative. Does this rule out toxin ingestion? Will this change your management?
- biochemistry
- general paediatrics
- neonatology
- toxicology
Statistics from Altmetric.com
Introduction
The paediatric population are exposed to toxins more than any other age group. In the USA in 2016, 60% of all exposures were in the paediatric population and 1.6% of all children had a reported exposure to a toxin. Seventy-seven per cent of paediatric exposures were in children aged <6 years.1
Most cases of toxin exposure in the under 12s are accidental, whereas the teenage population tend to have intentional exposures.2 The adolescent group carry higher rates of morbidity and mortality following exposure. Of all toxin-related fatalities, 73% of the total fatalities (across children and adults) were in the paediatric population, with 42% being in the 12–19 age group.1
Clearly, toxin exposure in paediatric patients is an important and serious presentation. However, detecting the toxin involved can be difficult, and toxin screening as a diagnostic tool is controversial, poorly understood and consensus on how it should be used is lacking.
Qualitative urine toxicology screens are relatively low cost and straightforward tests, and many are requested by paediatricians every day. The use of this test is significantly increasing, but there is often a lack of clarity regarding interpretation ofthe results.3
Physiological background and technical background
A urine toxicology screen is a qualitative test of specific drugs or their metabolites in the urine.2 Substances are detected in the urine by enzymatic immunoassays (EIAs). However, many of these lack specificity and/or sensitivity, and they are limited to drugs that reach detectable concentrations in the urine.3
With an immunoassay, an antibody binds to a specific part of a molecule’s structure as shown in figure 1. This causes problems as many drugs and toxins share similar structures, and conversely within the same class of drugs, compounds may have quite differing structures.3
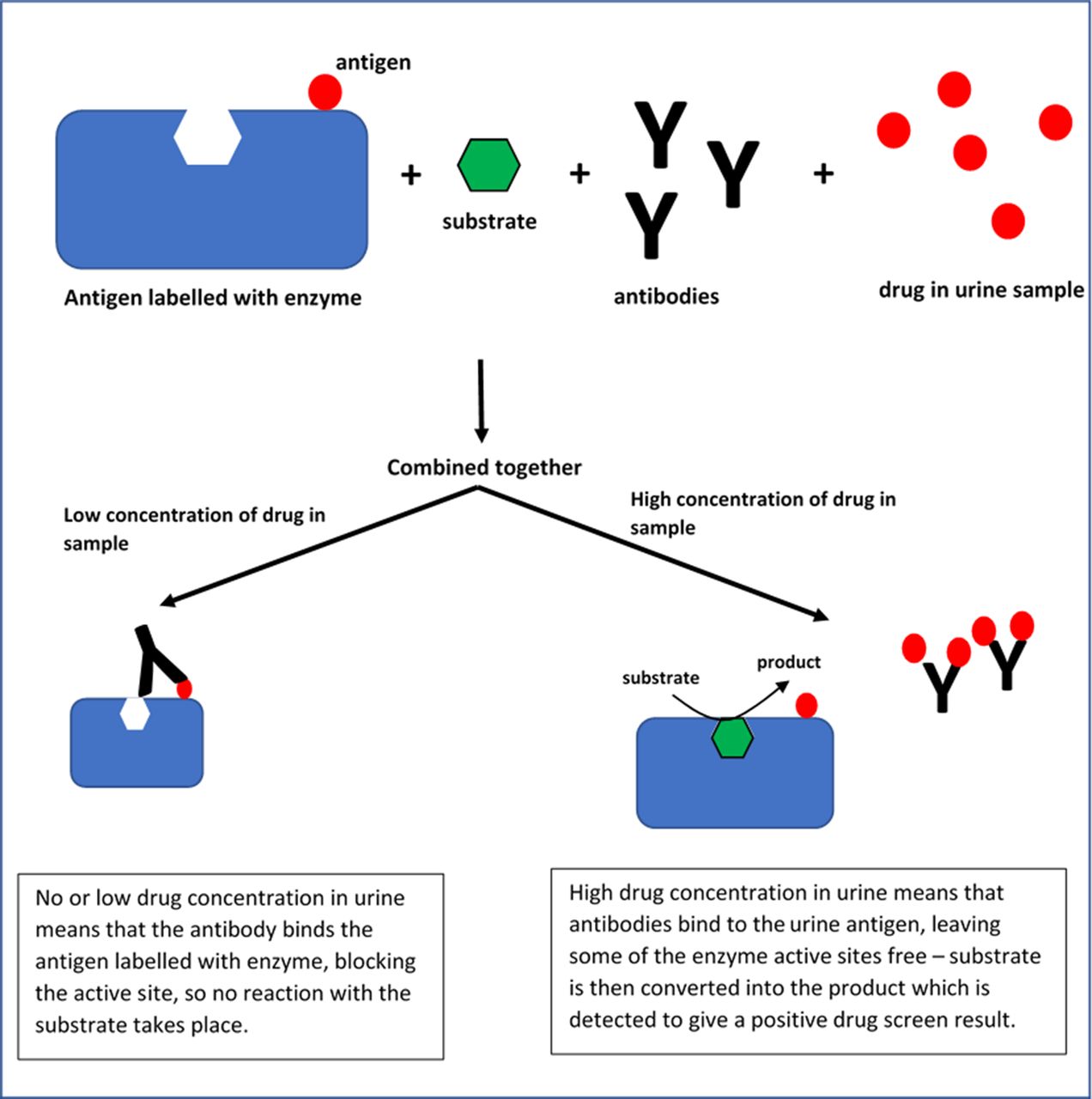
Enzyme immunoassay in urine toxicology screen—a commonly used technique.
Urine collection pads in younger children, are an accurate way to take urine toxicology samples and so this test is relatively straight forward to perform even in younger children without bladder control.4
Indications/limitations
Interpreting a urine toxicology test
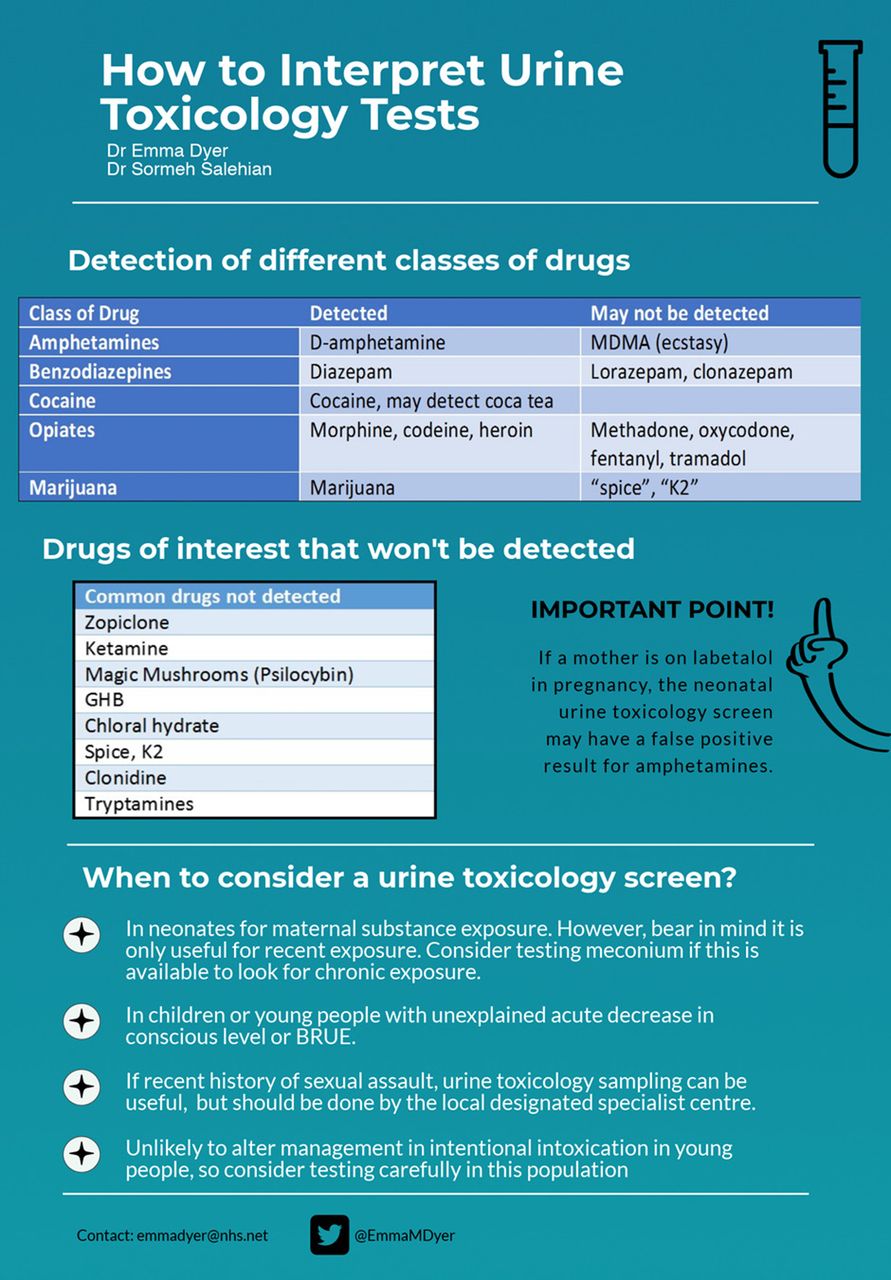
The sensitivity and specificity of urine toxicology screens vary depending on which toxin you are detecting. The EIAs may be able to detect one drug in a particular class, but not others. Table 1 outlines the main classes of drugs tested for on a urine toxicology screen including what will be picked up and what it may miss.
Extent of urine toxicology detection for different classes of drugs.3 7
In addition to these toxins, there are other classes that would not be picked up at all by a routine screen, but may still be of interest, as seen in box 1.
Drugs/toxins not detected by routine urine toxicology screening3
Non-benzodiazepine hypnotics (zolpidem, zopiclone)
Ketamine
Mescaline (peyote)
Psilocybin (magic mushrooms)
Gamma-hydroxybutyrate (GHB)
1,4-Butanediol (precursor to GHB)
Chloral hydrate
Synthetic/designer cannabinoids (‘spice’ and ‘K2’)
Tryptamines
Phenethylamine derivatives (synthetic stimulants, ‘bath salts’, ‘2C’ drugs)
Imidazoline receptor agonists (clonidine, tetrahydrozoline, oxymetazoline)
The presence of drugs at a detectable level in the urine is generally short lived, although metabolites may be present for longer.2 3 Different substances remain in the urine for different lengths of time after ingestion, and this influences interpretation. Table 2 demonstrates the timelines for detection of some of the more common substances.3
timelines for detection3
Any positive test should ideally be sent for confirmatory testing, the gold standard being gas chromatography or mass spectrometry. This is time-consuming and expensive and may not be widely available. Even this may still fail to detect certain substances.3
A positive test may suggest exposure to a substance, however that does not mean that the signs or symptoms demonstrated are attributable to that substance. There is a danger that with a positive screen other diagnoses may be missed, and it is important to remember that a urine toxicology screen is not a diagnostic test.2 3
A negative test tells you that the substance was not present at the time of testing at the minimum threshold quantity for detection, but cannot rule out exposure to the substance.2
Due to all of these factors, a urine toxicology screen should only be part of the overall picture. The clinical assessment of the patient and knowledge of signs and symptoms associated with ingestion of certain substances should be the basis for clinical decision-making and should take precedent over urine drug screening results.3
When might a urine toxicology screen be used?
Neonatal use
In-utero toxin exposure, whether to recreational or prescribed drugs, can impact foetal development. This includes short-term effects such as neonatal abstinence syndrome and more long-term effects such as reduced growth, sudden infant death, and abnormal neurological and behavioural development. It is therefore important to identify neonates who are at risk from maternal toxin exposure. Self-reporting rates suggest that up to 10% of woman use illicit drugs in pregnancy, but screening gives higher estimates5
As maternal history may be unreliable, toxicology testing of the baby may be beneficial. Presence of drugs in the urine is particularly short lived in neonates, and only foetal exposure for 3–7 days (depending on the drug) before collection will be reflected. Therefore, a negative urine toxicology screen does not rule out maternal prenatal substance exposure. It is also worth noting that maternal labetalol use can give positive amphetamine results, thought to be due to cross-reactivity with labetalol metabolites.6
If there has been intrapartum medical use of opioids, there can be concern about that causing a positive opioid result on a neonatal urine toxicology screen. As discussed, synthetic opioids such as fentanyl and tramadol will not be detected and semi-synthetic opioids such as pethidine have variable cross-reactivity depending on the EIA. Therefore, a positive screen may not be related to medical opiate use, particularly if synthetic or semi-synthetic opiates were used.2
To screen for more chronic substance exposure, hair or meconium can be used; however, these tests are less widely available. Furthermore, if the first maternal substance exposure was very soon before delivery, it may not yet have been deposited in the meconium, therefore you may get a false negative.2
It has been demonstrated that in neonates, urine toxicology screening has a low yield. In one large study, urine screening did not pick up any non-medical drug use that was not picked up by meconium testing. However, the urine testing failed to detect a significant number of cases of non-medical drug use that were picked up by meconium analysis.6
Testing in altered consciousness
In paediatric patients presenting with Brief Resolved Unexplained Events (BRUE) (formally Apparent Life Threatening Episode [ALTE]) or altered consciousness, it is important to consider a toxicological cause, particularly given how prevalent toxin exposure is in this population.2
In one study looking at patients under two presenting with ALTEs, 8.4% had a positive urine toxicology screen that could demonstrate a possible cause. They therefore suggested that this was a routine part of investigations in an ALTE presentation.7 Similar findings have been replicated in other studies, which have also highlighted that urine toxicology screens were useful in picking up toxins as a cause of apnoea.8
In line with this, the Royal College of Paediatrics and Child Health guideline in managing children and young people with an acute decrease in conscious level suggested that 10 mL of urine be collected and saved for later analysis, including urine toxicology.9
Use in intoxication and in the teenage population
Recreational drug use in teenagers is an under-recognised cause of mortality and morbidity and those who start using recreational drugs during childhood, have a much higher risk of dependence. It is tempting to want to detect recreational drug use in order to raise the issue with young people; however, there is little evidence that positive urine toxicology tests have any bearing on reduction of recreational drug use in adolescents.10
In one study looking at urine toxicology screens performed in paediatric emergency department (ED), 7% gave an unexpectedly positive result. However, only in 1% did this lead to a change in management, and all of these cases had signs and/or symptoms consistent with the drug that had been ingested.11 Thus, they concluded that generally speaking urine toxicology screening rarely alters management and we should think carefully before testing this in ED.
Use in safeguarding/assault cases
In sexual assault cases, alcohol or drug use immediately before the event is reported in over 40% of adolescent victims and adolescent perpetrators. This may be coincidental due to recreational drug use being common in adolescents, but if drug facilitated sexual assault is suspected, it can be important to establish the substance involved.12 In the UK, the faculty of forensic and legal medicine recommends that when doing a forensic examination following a sexual assault, a urine sample to test for drugs and/or alcohol be obtained if the incident happened within the preceding 5 days. If it occurred over 3 days ago, they recommend that hair is also taken for testing due to rapid clearance from the urine.13
Some relevant drugs will not show up on the screen. It is important to be aware of the implications of positive and negative drug screens so as not to mislead the healthcare and/or litigation teams in these cases. Particularly with a negative screen as that does not rule out the use of drugs to sedate the victim.3
It is important to note that in the UK these examinations are not usually carried out by general paediatricians, and best practice is to refer patients within an hour of disclosure to the local specialist unit, who can collect forensic samples as required.14
For a summary of the article, see figure 2.

{kind=link}
{kind=link}
Summary infographic. GHB, gamma-hydroxybutyrate; MDMA, 3,4-methylenedioxyamphetamine.
Clinical bottom line
Point of care urine toxicology testing is quick, inexpensive and simple to do.
A negative result does not indicate absence of substance and clinical judgement takes priority.
Be aware of false positives in neonates where mother has been taking labetalol.
Consider urine toxicology for all cases of altered consciousness.
Urine toxicology testing is useful is cases of sexual assault, but sample collection should be done by specialist centres rather than general paediatricians.
Footnotes
Contributors EMD was responsible for all aspects of this work including the outline and content of the manuscript and design of the infographic. SS critically appraised the manuscript and contributed further ideas. All authors edited the manuscript and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Patient consent for publication Not required.