Article Text

Statistics from Altmetric.com
Answers TO THE QUIZ ON PAGE 146
-
Figure 1 shows an abnormal bowel gas distribution with central paucity, and the impression that bowel is displaced into the upper abdomen.
-
Figure 2 shows a large fluid-filled mass occupying most of the central abdomen but not extending above the liver (arrowed) into the subphrenic space. This was initially erroneously reported as gross ascites.
-
Figure 3 shows a large septated cystic abdominal mass, with no discernible cyst wall. Its maximum dimensions are 18.5×10.5×23.5 cm (transverse × antero-posterior × cranio-caudal diameters).
-
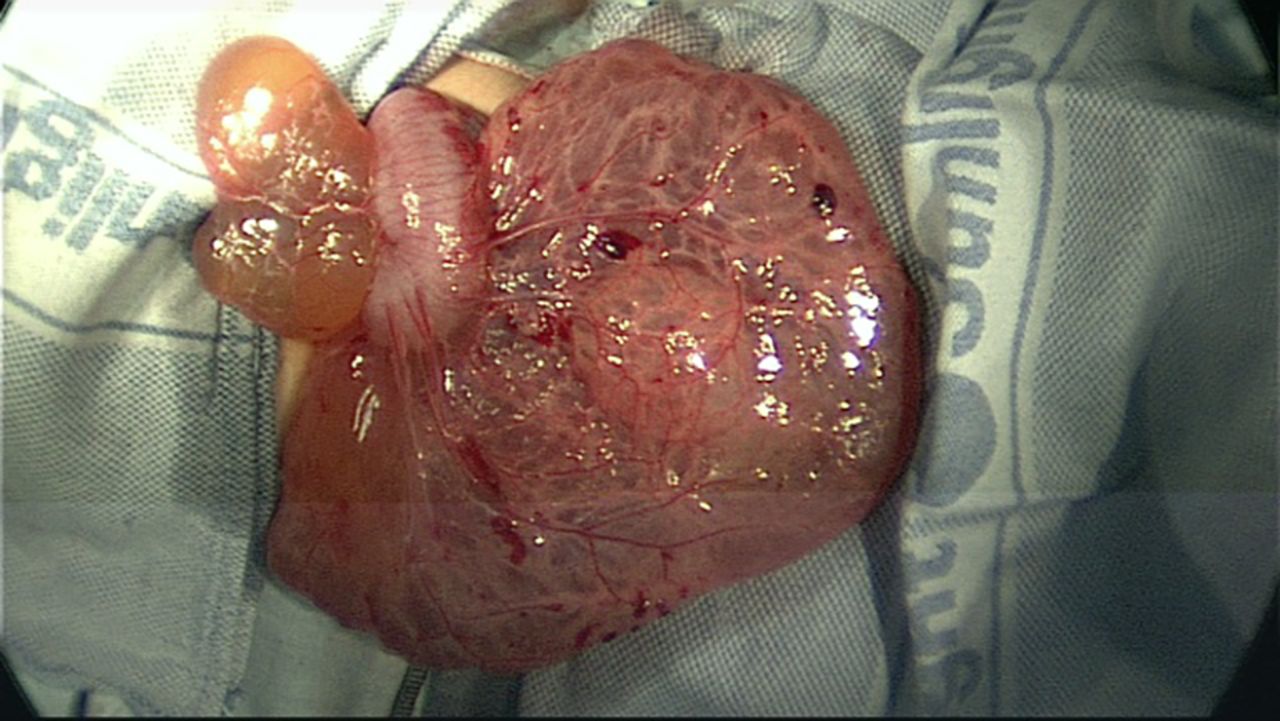
The consensus in this case was that it was likely to be a congenital mesenteric cyst. He underwent a diagnostic laparoscopy, which confirmed the presence of a cyst arising from the sigmoid colon and its mesentery. An 800 mL of clear sterile fluid was drained and a dissection of the cyst attempted. Dense adhesions of the cyst to the sigmoid colon, however, required the resection of a segment of the sigmoid colon laparoscopically (figure 4) along with subsequent primary anastomosis. He was discharged 3 days postoperatively with no complications. He was reviewed 3 months later with ongoing mild constipation, hence abdominal USS was repeated which confirmed no recurrence of the cyst.
Histological examination of the multiloculated cyst showed that it was lined by flat cells and the wall varied in thickness. Some locules were thin-walled and others had a thicker wall that consisted of vascularised fibrofatty tissue containing smooth muscle fibres and scattered lymphoid aggregates. These appearances are in keeping with mesenteric cyst with features of lymphatic cyst. There was no underlying bowel pathology.
Retroperitoneal and omental cysts can have similar appearances and presentation.1 ,2 Other differential diagnosis includes acquired cysts such as hydatid cyst which is commonly caused by Echinococcus granulosus or Echinococcus multilocularis and frequently occurs in liver and lungs.3 Intraperitoneal hydatid cyst is often secondary to rupture of primary hepatic cyst,4 whereas primary intraperitoneal and mesenteric hydatid cysts are rare.5 ,6
-
Mesenteric cysts are rare benign intra-abdominal tumours which are not easily detected clinically.2 They originate from ectopic lymphatic tissue and their precise aetiology is uncertain. Several theories have been suggested: failure of benign ectopic lymphatic proliferation to communicate with the functioning lymphatic system, lack of connection between the lymphatic and venous systems, neoplastic obstruction of the lymph system, intra-abdominal trauma and lymph node degeneration.1 ,2 ,7 They can occur anywhere between the duodenum and rectum but are commonly found in the small bowel mesentery associated with the ileum.2 ,8
-
In this case, the presentation was chronic with abdominal distention, constipation and mild abdominal pain. Mesenteric cysts can also present with a painless mass or acutely with intestinal obstruction secondary to volvulus.1 ,9 These cysts may be detected on antenatal ultrasound or as incidental findings on imaging studies at any age.1 ,7 ,9 As reported in this case, large mesenteric cysts can simulate ascites with abdominal distension, shifting dullness and fluid thrill, but useful distinguishing features include the lack of abdominal flank bulging, pouting of umbilicus and scrotal swelling.10
Mesenteric cysts are very rare and their presentation is variable. In this case, the initial USS findings were misleading and a subtle but important radiological sign did, in fact, argue against the presence of gross ascites, namely, the absence of fluid in the subphrenic spaces. The appearance of the abdominal radiograph was inconsistent with large amounts of ascites in which, typically, the bowel is displaced into the central abdomen rather than away from it.

{kind=link}
The excised mesenteric cyst with a segment of the sigmoid colon.
Acknowledgments
We thank Shirley Weekes, paediatric secretary at Birmingham Children's Hospital.
Footnotes
-
Funding None.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.