Article Text

Abstract
Drooling beyond the age of 4 years is neurodevelopmentally abnormal. Chronic “sialorrhoea” is seen in children with abnormal oral sensation and/or motor control and more infrequently when there is excessive production of saliva. Salivary production from the paired glands is under autonomic parasympathetic control. Management of the problem relies on multidisciplinary teams with a focus on assessment and when appropriate conservative interventions, oral motor training, dental appliances, medical and surgical treatment programs. Medically, the focus is on modifying the neuroglandular control of saliva with the use of anticholinergic agents. The article covers these areas of background, assessment and management in detail.
Statistics from Altmetric.com
Drooling (or dribbling), where saliva is present beyond the lip margin, is normal in babies and infants. As neurological control of the tongue and bulbar musculature develops, salivary “continence” normally occurs by 15–18 months, though a high number of typically developing children will continue to drool up until the age of 3 years, especially during eating and drinking. The ability to control saliva develops alongside normal feeding and oral-motor control. It is certainly considered abnormal to have problems with saliva control (sialorrhoea) beyond the age of 4 years.
The unconscious swallowing of saliva is a complex process and is indeed one of the most intricate motor functions in a human. The coordination of over 25 pairs of bulbar muscles is vital to maintain the integrity of the swallow reflex.
Acute sialorrhoea may be associated with inflammation or infections of the oral cavity or dental problems causing hypersalivation. Some anticonvulsants, such as clonazepam and clobazam, may also increase saliva production (hypersialia). Chronically, it is seen in children with a general physical disability or a specific oral-motor difficulty.1 2 Drooling is normally due to inefficient tongue and/or bulbar control rather than poor lip closure or hypersialia in isolation.3 This can be a multifaceted dysfunction, with lack of external somatic and intraoral sensation being involved as well as the impaired motor coordination in or around the mouth. Head control and the posture of the individual are obviously also important.4 5
The overall prevalence of significant chronic drooling in childhood is put at up to 0.6%.The commonest population group with severe and persisting difficulty is children with quadriplegic cerebral palsy where the prevalence rate is as high as 30–53%.6
The consequences of poor saliva control include negative comments from other children, unpleasant odours, social embarrassment and isolation and specific physical problems such as dehydration and skin breakdown (table 1).4 5 7
Possible causes of sialorrhoea
Saliva production
A child will typically produce 1–1.5 litres of saliva everyday. There is little information available on the frequency of swallowing in children, but adults swallow approximately once every minute while awake. Although this is an automatic act, it is also dependent on the ability to feel the build-up of saliva within the mouth as well as normal movement of the tongue to collect it and transfer it to the back of the mouth for swallowing.
Saliva production occurs predominantly in three pairs of salivary glands, the submandibular, sublingual and parotid. The submandibular glands produce the watery saliva that bathes the oral cavity at rest, approximately 65–70% of total production. The sublingual glands produce a small amount of thicker saliva that tends to coat the teeth and the parotid glands produce about 20% of the total, comprising watery secretions that are important for chewing and swallowing.
Neurologically, the salivary glands are under the automatic control of the parasympathetic (secretory excitation) as well as the sympathetic (alters viscosity) nervous system. These in turn are regulated by external somatic stimuli such as vision, smell and taste. The parasympathetic fibres originate in the pons and medulla of the mid-brain and synapse in the otic (parotid) and submandibular (submandibular and sublingual) ganglia. The postganglionic parasympathetic fibres release acetylcholine (ACh) at the nerve endings; this neurotransmitter directly stimulates the secretion of saliva in the relevant gland.
Saliva is important for maintenance of a homeostatic microenvironment in the mouth, at rest and at times of feeding, keeping the acid–base and bacterial balance optimal, having bacteriostatic and bactericidal effects. Lubrication of the oral cavity is vital to maintain dental and oral hygiene and to facilitate ease of swallowing. It is also important for the early stages of carbohydrate digestion.
Clinical assessment and management
Ideally, as with most elements of neurodisability care, assessment and management of salivary control difficulties should be carried out by multidisciplinary teams.8 9 These should include expert speech and language therapists, occupational therapists, dentists, ear nose and throat surgeons and interested paediatricians. Many tertiary centres run specific salivary control clinics; others have specialists who have developed an interest in this area of management.
It is important to take a thorough history, focussing especially on oral-motor control and aspects that may increase the problems of drooling such as posture, medication, dental health, ENT symptoms and neurological status. Gastrointestinal reflux and constipation, the frequency of urinary flow and chest health are also of relevance.
Quantification of the problem focuses on how disruptive the drooling is on general activities of daily living and quality of life. The Thomas-Stonell and Greenberg classification is generally accepted as useful.10 Also a “bibometer” or “bib diary” of how many bibs are necessary during the course of a day is useful as a rough measure of sialorrhoea. In research, absorbent dental rolls can be placed near the opening of salivary ducts to more specifically delineate the quantity of saliva produced pre- intervention and post-intervention (table 2).
Drooling Rating Scale—Thomas-Stonell and Greenberg
Observation is made of feeding, drinking and swallowing and the child at rest and when performing a simple task which requires concentration, appropriate to the child's neurological status.
A clinical examination is then performed, focusing on the dental health, postural control and the neurology of the tongue, cranial nerves, bulbar region, swallowing and the respiratory system.
Management
Management of sialorrhoea can be simply broken down into five areas, which are not necessarily mutually exclusive. This paper will outline current practice in:
Conservative/alternative
Specific oral-motor exercises
The use of intraoral devices
Medical
Surgical interventions to help individuals with saliva control.
A specific, individualised management plan is then drawn up with the child and family. Many different aspects of salivary control may be focussed on. The overall guiding philosophy is to optimise the quality of life of the child, without compromising oral health. Significant improvements in self-esteem and social interaction can be gained by successful management programs.7
Conservative/alternative
If dental problems, such as malocclusion, gum disease or caries, are found at the time of assessment, then these should be dealt with specifically. Routine good oral health is vital, especially if considering treatment options that may reduce the amount of saliva secreted into the mouth. If problems with the adenoids or tonsils causing nasal obstruction are discovered, referral to ENT may be indicated. Postural control of the head, neck and trunk may also need to be addressed.
If a child is able to wipe his/her own mouth, the use of sports towelling wristbands may be more socially acceptable, particularly to peers, than handkerchiefs or bibs as the child gets older. “Dabbing” rather than “wiping” across the mouth and chin causes less local stimulation to the salivary glands.
In severe or profuse drooling, where protection of clothing is necessary, there are specialist providers of absorbent neckerchiefs and bandanas that are more age appropriate than infant bibs. A trawl via an internet web search engine will give numerous examples applicable in different countries; a good United Kingdom example is http://www.dribble-bandanas.co.uk/.
Prevention of excessive mouthing of fingers or objects helps reduce the stimulus of saliva production and encourages lip closure. Simple distraction therapy is generally best for this, providing alternative sensory input, though the problem can be so severe that it may be necessary to provide gloves or elbow splints.
Sweet fizzy drinks can cause direct effects on increasing saliva production, as can very acidic food stuffs such as vinegar or lemon juice. It is, therefore, best to avoid them.
Acupuncture11 and homeopathic remedies have been used with individual good effects, but no controlled clinical trials have been reported. Similarly, over the counter acupressure, wrist bands are helpful in some individuals, especially for short periods of time, and may, therefore, be used for special occasions, such as family events, parties or photographs.
Oral-motor exercises
If an individual child has appropriate levels of attention and compliance, specific oral-motor exercises can be helpful.12 Some children, if they are able to follow directions, can achieve control of their saliva with the help of tongue and mouth exercises organised by speech and language therapists. It often takes a considerable period of time to improve the situation, and the control gained is often very dependent on the level of concentration of the child and what other tasks are being performed at the same time. Programs may include measures to improve oral-facial tone, increase sensory awareness and develop voluntary control of movement. Short-term effects on facial tone are reported following oral-facial facilitation techniques such as brushing, vibration and manipulation, but there is little published research confirming longer-term effects on saliva control. Some of these techniques suggested in the literature, including “icing” and use of vibration, where sensory stimuli are applied to the facial muscles, may have potential harmful effects if applied with inadequate knowledge.
The family and carers must “buy in” to oral-motor programs too as the child will need considerable long-term encouragement and support in order to gain any degree of success. The evidence base for oral-motor therapy is very limited, particularly in children with severe disabilities, and clinical experience suggests this approach is only applicable to children with mild to moderate oral dysfunction, good cognitive skills and a high level of motivation.
The use of biofeedback systems to improve background swallowing frequency has also been looked at in some centres with a degree of success.13 Here, an auditory cue is used to remind an individual to swallow, helping them to develop a better pattern of control.
Intraoral devices
Palatal training appliances can also be very effective in some children, normally those with mild to moderate difficulty who have had eruption of their adult teeth.14 The highly specific, modified braces have a series of ridges and bumps over the intraoral surface and often a wire loop at the back. These encourage active lip, tongue and palatal movements, moving saliva to the back of the oral cavity for swallowing rather than passive spill from the front. The risk of aspiration or airway blockage means they are not suitable for children or young people with severely limited control of tongue movement, and epilepsy is a contraindication.
Medical
Anticholinergic medication/botulinum toxin injections
As the secretion of saliva is under parasympathetic autonomic control, with ACh working as the specific neurotransmitter, downregulation of ACh would theoretically lead to a reduction in the production of saliva. However, the use of transdermal and oral medication is often poorly tolerated due to a high prevalence of unwanted side effects.
All medicines are used off license for the management of sialorrhoea and careful discussion particularly about potential side effects must take place between the assessing team, child, families and local prescriber before the initiation of therapy.
Targeted injections of botulinum toxin type A directly into the salivary glands are also used in many specialist centres. These block ACh release, therefore, reducing secretion of saliva.
Other drugs such as antipsychotics, tricyclic antidepressants and behavioural modifiers such as Methylphenidate can all cause dryness of the mouth but are not regularly used for that effect in children.
Anticholinergic medicines
▶ Hyoscine patches
▶ Glycopyronnium bromide
▶ Trihexyphenidyl–benzhexol hydrochloride
▶ Benztropine
▶ Ipratropium bromide
Many medicines with anticholinergic (antimuscarinic) properties have been developed for medical use. Some are used for motion sickness or gut “spasms”, others for preanaesthetic drying of secretions and others in primary or secondary dystonic movement disorders, such as Parkinson's disease.
Common-autonomic-system-mediated side effects include blurred vision due to accommodative difficulties, constipation and urinary retention due to relaxation of bowel smooth muscle and the detrusor muscle of the bladder. As sweating is mediated by the parasympathetic nervous system, it is advisable to be cautious about using anticholinergics in very hot weather as the temperature control homeostatic system may be compromised. Central-nervous-system-mediated side effects include sedation, irritability, headache and increase in frequency of seizures. There is an absolute contra-indication of using anticholinergics in individuals with glaucoma, myasthenia gravis and a history of urinary retention. A cautious dose implementation should be taken in individuals with severe gastrointestinal disorders, including gastro-oesophageal reflux and/or constipation.
A systematic review of the literature in 2003 on the use of oral anticholinergics showed limited published evidence for their use. Some benefit was shown with trihexyphenidyl, glycopyronnium and benztropine, but no comparative data or meta-analysis was able to be made.15
Hyoscine patches—topical
Transdermal hyoscine patches (scopolamine, Scopoderm TTS, Novartis Consumer Health) have been used in the management of sialorrhoea for a long period.16 There is considerable variation in efficacy between individuals; many find them extremely useful, especially for short-term use.
However, allergic skin reactions at the site of use are frequent and troublesome, and problems with deterioration in seizure control have been reported.17 Xerostomia (uncomfortable dry mouth) and dryness of the eyes are often observed with a consequent compromise of oral-motor function and/or functional visual disturbance.18 If used continuously, the patches tend to lose benefit (table 3).
Hyoscine patch doses and administration
Glycopyronnium bromide—oral
Glycopyronnium bromide (glycopyrollate, Robinul, Antigen) is a preanaesthetic medicine used to reduce oral and airway secretions. It is generally better tolerated than transdermal hyoscine, with a less frequently observed but similar side effect profile.19 20 It can be given orally or via an injection.
It has a rapid onset of effect, within 1–5 min when injected and within 15–30 min when given orally. Peak of effect occurs within 1–4 h with duration of action up to 6–8 h, depending on individual response. It should be given with meals at breakfast, lunch and supper. It can be particularly useful if a child is troubled by secretions at night time (table 4).
Glycopyronnium bromide doses
Trihexyphenidyl–benzhexol hydrochloride—oral
Trihexyphenidyl (benzhexol, Broflex, Alliance) is an oral anticholinergic primarily used in dystonic movement disorders. As such, it reduces ACh release at the basal ganglia level to help improve fluidity of motor control. It can be given as a tablet or liquid preparation.
For sialorrhoea management, doses should be started very low, with slow incremental doses, weekly at most.21 After oral administration, trihexyphenidyl has an onset of effect within an hour, a peak effect at 1–3 h and a half-life of 6–8 h. It should be given with meals, at breakfast, lunch and supper (table 5).
Benzhexol doses
Individuals who also have a dystonic movement disorder may particularly benefit from trihexyphenidyl. In these children, much higher doses may be necessary. For dystonia management, Professor Robert Surtees from Great Ormond Street recommended total upper dose limits of 9 mg/day in infants, 30 mg/day in children and 60 mg/day in adolescents.22 As these doses are far higher than those recommended in the British National Formulary, careful review of children is necessary. However, it may take such a significant dose to help with motor fluidity. Obviously with higher doses, there is a greater potential of side effects; primarily of urinary retention, gastrointestinal disturbance, irritability or paroxysmal increased dyskinetic movements. The side effects are reversible with dose reduction.
Benztropine—oral
There have been a few reports of limited validity that benztropine also has a positive effect on drooling. Dose ranges of 3–3.8 mg/day have been cited. High levels of side effects are seen including anxiety, depression and sedation.23
Ipratropium bromide—inhaled
Inhaled ipratropium bromide (Atrovent, Boehringer Ingelheim) is a quaternary ammonium derivative of Atropine. It is an anticholinergic compound with bronchodilator properties. It is used in the management of asthma, and on inhalation, it has an onset of effect within 5–15 min, a peak effect at 1–2 h and a half-life of 3–4 h. Some effect is observed up to 8 h post-inhalation (table 6).
Ipratropium bromide doses
There is a low level of observed systemic side effects, most commonly headache, tachycardia, blurred vision from accommodative problems and gastrointestinal dysmotility. The most common observed “side effect” is drying of the mouth in between 9.3% and 15%. In adult populations, this side effect has been used to some effect to reduce sialorrhoea in individuals with Parkinson's disease.24 As it is generally well tolerated and easy to give via a nebulised solution, it is a useful adjunct in children. However, no trials as yet have been reported in the paediatric literature
Botulinum toxin type A injections (Botox, Allergan; Dysport, Ipsen)
Considerable work has been reported on over the last decade looking at the use of targeted botulinum toxin type A injected into the salivary glands.25,–,34 When injected directly, this potent neurotoxin is taken up into the parasympathetic end plate and irreversibly blocks release of ACh. Reinnervation occurs as regression of the terminal end plates within the injected salivary gland occurs followed by re-sprouting from the end of the axonal sheath to create a new neuroglandular junction. Quantitative and qualitative benefit is reported for between 1 and 6 months with maximum benefit at 4–6 weeks post-injection. Potential side effects are major, particularly thickening of secretions and dysphagia.
This is an off-license use of botulinum toxin type A but has been recognised in peer-reviewed documents such as the European Consensus statement as causing reproducible benefit.35 Injection must occur under ultrasound guidance to ensure correct positioning of the needle.36 Dosing and volume of diluent (aliquot) are also vital (table 7).
Botulinum toxin A—dose ranges
Generally, those of us who regularly perform injections to the salivary glands would recommend the following:
▶ Do not do it—use a tertiary specialist centre, it is scary up there!
▶ Keep doses low to limit potential side effects of dysphagia due to mal-placement or spread of toxin to surrounding muscles
▶ Consider halving recommended doses in children <8 years old or if the salivary glands look small
▶ Keep diluent of normal saline aliquot low for the same reason
▶ Ensure adequate local anaesthetic and sedation; many units use general anaesthetic alone
▶ Specialist personal practice will lead to which combination of salivary glands is injected, generally submandibular glands plus one or two parotid glands.
▶ Most studies use Botox; there is some anecdotal evidence for less spread and, therefore, a safer side effect profile but use which ever preparation your centre is used to.
▶ Do not attempt to do it unless you are well trained and confident of your skill; talk to your ENT and radiological colleagues.
Surgery
A number of different surgical approaches have been used to help with sialorrhoea.37,–,40 Also, in adults targeted, radiotherapy is used, though this is not a treatment approach in the paediatric population (table 8).
Surgical procedures
Results of drooling surgery in children are variable.41 Some children gain considerable long-term benefit. For others, there is only a temporary improvement, with consequences of a dry mouth, poor oral hygiene, dental decay and difficulty in chewing. Obviously, the expertise of the surgeon is vital when considering any “definitive” procedure.
Summary
The assessment and management of chronic drooling in children is best coordinated by a specialist multidisciplinary team liaising with local services. There are a considerable number of options for treatment depending on the age of the child and the severity of the problem. Therapy-based and conservative options should be considered first, after potential dental or “conservative” ENT options are ruled out. Unless there are specific contraindications, it is best to then try medical treatment before progressing to surgical procedures.
However, the published evidence base for many of the treatments described is patchy at best. As the problem is so significant to many children and their families, this is undoubtedly an area that needs future large-scale comparative study.

{kind=link}
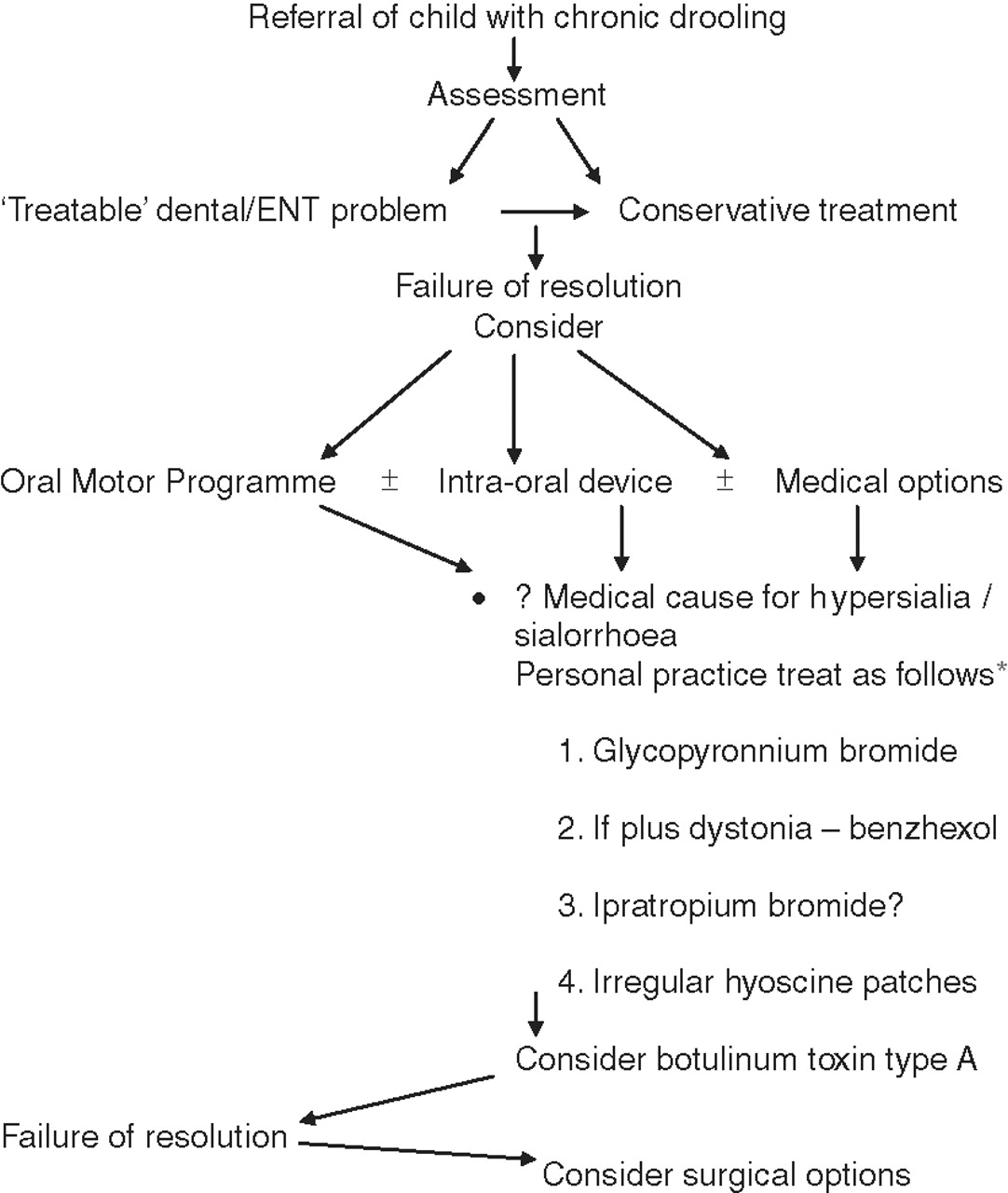
Personal practice algorithm.
*Just to stress that the proven efficacy of the various oral, topical and inhaled anticholinergics is limited and others individual practice may vary as to the order of which to use. I use this algorithm.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.