Article Text

Statistics from Altmetric.com
Syncope is a symptom, defined by the European Cardiology Society as a transient, self-limited loss of consciousness (TLOC), usually leading to falling. The onset of syncope is relatively rapid, and the subsequent recovery is spontaneous, complete and usually prompt.1 However, for reasons that become clearer later, we prefer the physiologist's definition: “Syncope is a transient loss of consciousness resulting from an insufficient supply of oxygen to the brain”.2
In a population-based study, the incidence of syncope coming to medical attention in childhood and adolescence was 126/100 000.3 Up to 15% of children will experience at least one episode before the age of 18.4
The reported incidence reaches a peak in 15- to 19-year olds and is more common in females. In the population-based study, neurally mediated syncope (NMS) was by far the most frequent type of syncope (75%), cardiac disease was diagnosed in 10%, psychogenic or unexplained TLOC and syncope of unknown cause accounted for 8%, and possible epilepsy accounted for 5%.3 In our recent series, psychogenic or unexplained TLOC was more common (17%) in hospital patients undergoing more specialist investigation and was recognised in young people with concurrent NMS.
The collapse and loss of consciousness that occur during fainting or syncope are due to the abrupt cutting off of the energy substrates to the cerebral cortex. This is usually through a sudden decrease in cerebral perfusion by oxygenated blood from a reduction in cerebral blood flow itself, a drop in the oxygen content or a combination of these.5
There are many variations in clinical phenomenology: syncope can be of gradual or sudden onset, with or without a recalled warning, with hypotonia or an extensor spasm with upper limb abduction and or extension, or hypermotor with chaotic thrashing about. It may be accompanied by urinary incontinence. Recovery may be quick (mild syncope), or there may be postictal confusion or sleep (severe syncope). The key to diagnosis is the history immediately preceding the attack and the occurrence of pallor. Rarely, an acute symptomatic epileptic seizure, referred to as an “anoxic–epileptic seizure”,6 may occur in the course of a syncope—for example, during the recovery phase causing diagnostic confusion.
Categorising syncope
Syncope can be categorised descriptively from the history: reflex (ie, triggered by a stimulus, eg, an unexpected pain or sight of blood); orthostatic (predominantly on standing up); convulsive (with abnormal postures or a convulsion); sudden (with no warning and so a risk of injury) or gradual onset (with presyncopal symptoms and behaviours); mild or severe.
Presyncope describes the occurrence of warning symptoms without loss of consciousness. Presyncopal symptoms include a faint or dizzy feeling, nausea, feeling hot, or cold and/or sweaty, sometimes with visual perceptual changes, and/or a rushing noise in the ears.
Syncopal seizures were first described by Gastaut in 1974 as anoxic seizures7 and refer to the variety of clinical “epileptiform” postures and movements that can accompany syncope whatever the cause. They encompass atonic, tonic, clonic, tonic–clonic and hypermotor subtypes, may appear asymmetrical, and are associated with attenuation (flattening) of the EEG during severe syncope. Tonic, clonic, tonic–clonic and hypermotor varieties are called convulsive syncopes.
Mild syncope can be defined clinically by rapid recovery within seconds and neurophysiologically by an ictal/postictal EEG that is either normal or demonstrates transient high-amplitude slow waves only.
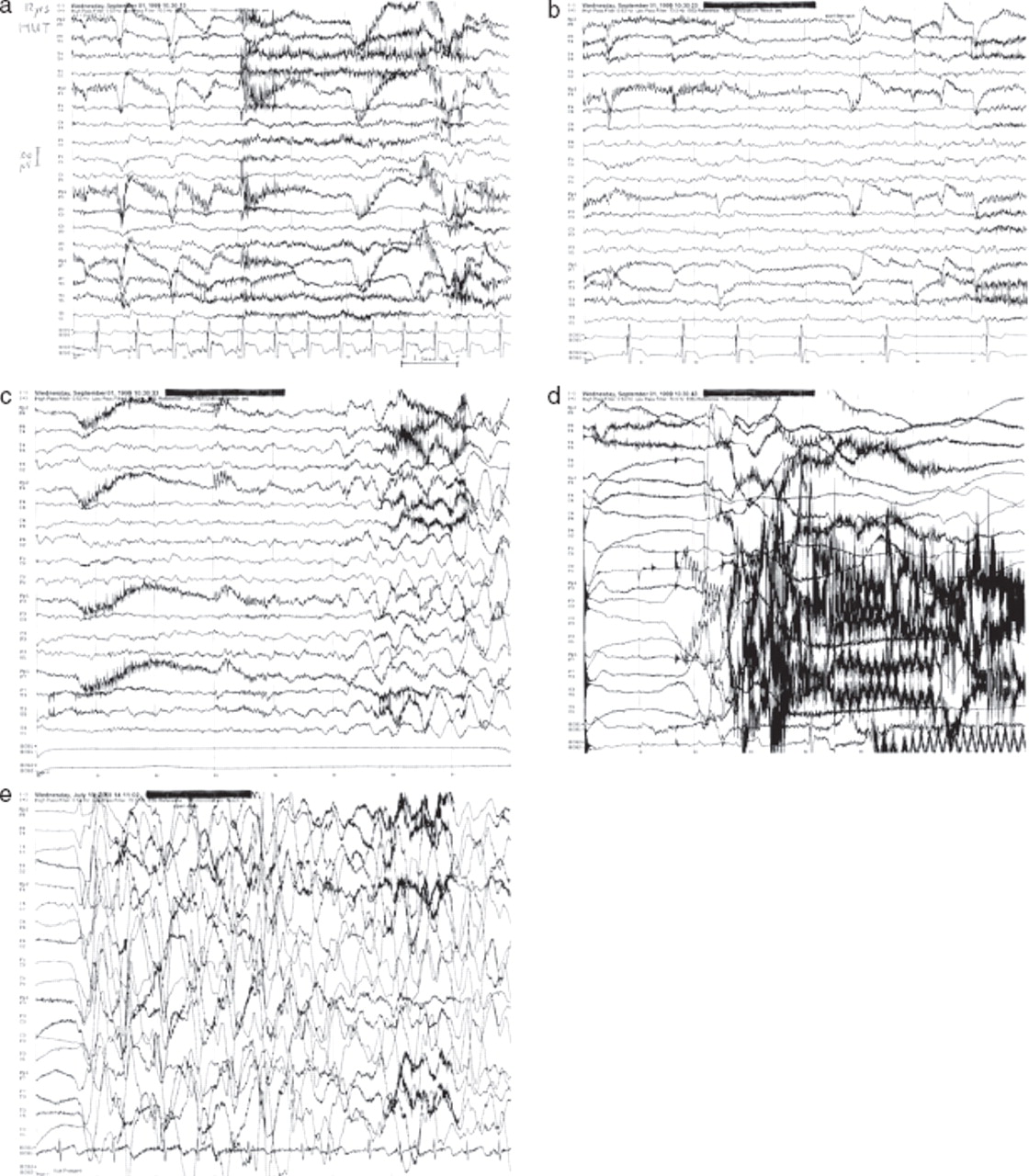
Severe syncope can be defined clinically by a prolonged postictal cerebral impairment (confusion or sleep) that lasts minutes or hours and neurophysiologically by the ictal/postictal EEG demonstrating the “slow–flat–slow” pattern (figure 1).
{kind=link}
EEG–ECG during severe convulsive syncope triggered by head-up tilt test in a child aged 11 years. (A) Normal background EEG with eye blinks and some muscle artefact, and normal ECG (bottom channel); patient conscious. (B) Normal background EEG with eye blinks, and start of sinus bradycardia; patient conscious. (C) Appearance of background EEG slow waves and high-amplitude slow waves after 5–6 s of asystole; patient feeling “faint” and loosing consciousness. (D) Attenuation (“flattening”) of background EEG after 8–9 s of asystole and marked muscle artefact corresponding to the extensor spasm and “convulsive syncope” from 10 to 17 s of asystole; patient unconscious flops then trunk stiffens and upper limbs stiffen and wave about. (E) Return of background EEG high-amplitude slow waves as sinus rhythm resumes; patient relaxes but appears sleepy and remains unconscious.
Alternatively, syncopes can be classified by their pathophysiological mechanisms and causes (in table 1, those relevant to paediatric practice are in boldface).
Classification of syncopes by patho-physiology and causes
Neurally mediated (neurocardiogenic, or reflex) syncopes
The archetypal variety is also known as vasovagal syncope. This refers to attacks of syncope experienced by children and adults that are autonomically mediated and associated with a reduction in (1) sympathetically mediated peripheral vasomotor tone and therefore peripheral vascular resistance and systemic blood pressure (the “vaso-“) and with an associated parasympathetically mediated bradycardia (the “-vagal”). The relative contributions of “vaso-” and “vagal-” components vary from predominantly “vaso-” (as in vasodepressor syncope) to exclusively “-vagal” (as in reflex asystolic syncope (RAS); see below).
Vasovagal syncope is more likely to happen when tired, hungry, stressed, feeling crowded, with pain, in the sight of blood or injury, in a fright, unwell, anaemic, dehydrated, hot, immediately after exercise, standing up suddenly and especially with combinations of such provoking or risk factors. These risk factors comprise emotional or psychological stress, hypotensive effects of hypovolaemia or vasodilation and orthostatic challenge. Because there is often a clear provocation, “reflex syncope” is the term preferred by some authors. That anaemia lowers the threshold for NMS is evidence that it is not the cerebral perfusion per se that counts but rather the oxygen delivery to the brain. This model would predict that NMS was more likely to occur when hypoxic.
Because presyncope is a common in NMS, and acts as a warning, injury is uncommon.
Chronic orthostatic intolerance
Orthostatic intolerance is observed in some patients with recurrent vasovagal syncope. Chronic orthostatic intolerance8 is defined as the occurrence of various symptoms including syncope on standing for a duration of at least 3 months. The other features include symptoms of presyncope: lightheadedness, “dizziness”, blurred vision and also exercise intolerance and chronic fatigue. Migrainous headache, nausea, abdominal discomfort, chest discomfort, palpitations, shortness of breath, hyperventilation, peripheral cyanosis, sweating and flushing on standing are also common. Stewart proposes that tiredness and excessive dislike of exercise can be useful aids to diagnosis. Chronic orthostatic intolerance is often part of the clinical picture of chronic fatigue syndromes, and it may be helpful to consider this treatable disorder as a differential of idiopathic chronic fatigue syndrome.
Postural tachycardia syndrome
One clinical picture including chronic orthostatic intolerance in teenagers and young adults is the postural tachycardia syndrome.9 10 Patients have symptoms of chronic orthostatic intolerance with significant daily disability, associated with a marked tachycardia on standing: a heart rate increase of >30 beats/min, or >35 beats/min in children <16 years of age,11 or a heart rate of >120 beats/min within 10 min of standing up from supine or head-up tilt.
Reflex asystolic syncope or reflex anoxic seizures
Reflex anoxic seizures has been the preferred term for paroxysmal episodes of collapse (usually with stiffening or jerking) provoked by pain or surprise in children and some adults.12 In the United Kingdom, it has superseded other terminology such as white breath-holding and pallid infantile syncope.12 In the North American literature, it is still known as severe breath holding,13 which encompasses a variety of other phenomena. The term “infantile vasovagal syncope” has also been suggested, although there is no evidence of a “vaso-” component, and has the advantage of implying the typical preschool age group. Older children and adults with the same disorder have “convulsive cardio-inhibitory NMS”.
In a typical attack, a toddler will have had a bump to his head or another unexpected, sudden pain or shock. He will cry out and fall limply to the floor within a few seconds. Because there is no warning, injury is common, although usually mild. The child will appear deathly pale and “lifeless” for around 5–30 s (with asystole lasting 5–30 s). Frequently, there will be, at the onset or within a few seconds, upward eye gaze and stiffening of the trunk in extension, typically with the upper limbs extended at the elbows and partly abducted or flexed at the shoulders, wrists and hands clawed in a dystonic posture for several seconds, sometimes with asymmetric limb jerking. Occasionally, there may be symmetrical jerking and urinary incontinence. During the extensor spasm, there is apnoea. After about half a minute, the child then comes round in a rather confused or distressed state before going off to sleep for an hour or so. In a child with recurrent reflex anoxic seizures some, attacks will have a history of no provocation.
The resemblance to epileptic seizures is clear enough, although careful history-taking concentrating on possible trigger events should be sufficient to ensure correct diagnosis. Traditionally, reflex anoxic seizures have been viewed only as an important exclusion in the diagnosis of paediatric epilepsy, and few have deemed it worthy of investigation or treatment in its own right. The fact that it falls in the hinterland between paediatric neurology and cardiology practice has added to this reluctance. Despite adult continuity it is rarely described at all in the adult literature and has been subsumed within the concepts of “breath-holding” or convulsive neurally mediated (ie, neurocardiogenic) syncope.14
Population estimates of the incidence and prevalence are lacking; however, in the toddler age group, from 1 to 4 years of age, where the incidence seems highest and the prevalence appears to be close to but less than that of epilepsy (4/1000),15 the prevalence can be estimated at about 1/1000. It is recognised that syncopes account for a large number of false diagnoses of epilepsy in all ages,16 RAS being the main differential in toddlers.
Blood injury phobia
Despite being viewed by many as a pathological extreme of the natural human anxiety around blood or injury, blood injury phobia (BIP) differs markedly from other simple phobias. In contrast to other phobias where exposure leads to a sympathetically mediated and sustained “flight or fight” response, those with BIP demonstrate transient tachycardia followed by bradycardia and even asystole after exposure to the feared stimuli. In addition, there is no increase in associated neurotic conditions or depression as has been found for simple phobias. Marks speculated that BIP may be the result of “pairing”, a conditioned psychological response arising when a strong vagal response (which may or may not amount to full syncope) coincides with exposure to blood or injury. Thereafter, the child will link blood or injury to the previous unpleasant reaction and start to display phobic avoidance behaviours.17 In support of his premise are two lines of evidence. First, it would be in keeping with the mean age of onset of BIP, which is 7 years.18 Second, there are case reports demonstrating continuity from RAS in early childhood to BIP in later childhood and adulthood.19 20 In the second case, the authors are unaware of the RAS diagnosis, but the clinical description is compelling. Marks also suggests that such children come from families with a genetically determined extreme bradycardic response. A strong family history exists for both BIP and RAS.
In patients with recurrent NMS—for example, vasovagal syncope, RAS and those with BIP, a strong family history has been described, especially when the onset is <20 years of age.21 22 Clinical histories are relatively stereotyped with typical symptoms including nausea, flushing, sweatiness and perceptual disturbance. The investigation of choice is head-up tilt testing, which typically causes bradycardia and hypotension, sometimes with a preceding tachycardia and reproduces premonitory symptoms. This procedure is also helpful for older children with RAS and may be combined with EEG and video.
Stephenson makes the useful distinction between vasovagal attacks and the purely vagally mediated events of RAS where there is no drop in peripheral vascular resistance.19 However, in clinical practice, we find that children with RAS can have identical attacks provoked by febrile illness or rapid standing rather than the usual sudden, unexpected pain. This suggests a degree of clinical overlap.
Vagovagal syncope
Another associated condition is vagovagal syncope.14 In this less common disorder, children and adults may collapse due to the direct vagal stimulation that can occur with swallowing, coughing, vomiting or gastro-oesophageal reflux, or intubation. Although usually viewed as benign, this can mean that migraine or viral gastroenteritis can lead to a run of disabling collapses and unconsciousness necessitating hospital admission. On occasion, cardiac pacing becomes necessary and this is discussed later. (See cardiac pacing on page 71).
Apnoeic syncope
Reflex prolonged expiratory apnoeic syncope (“reflex apnoeic syncope” or “blue breath-holding spells”)
Attacks caused by prolonged expiratory apnoea, without asystole but with cyanosis and collapse, can be hard to distinguish from RAS with asystole on history or casual observation.
“Breath-holding” can cause syncope, occur with syncope and may need to be differentiated from other syncopes or epilepsies. All of us have experienced the end-expiratory apnoea associated with uncontrollable crying; it precedes a loud inspiratory gasp before the next (expiratory) cry. It is recognised by the sudden but transient silence. In some toddlers the end-expiratory apnoea is prolonged and can, in those susceptible, produce TLOC or syncope. The view of some that this susceptibility indicates a naughty or spoilt child, poor parenting or lack of discipline is ill informed and usually incorrect. The image of a selfish wilful child deliberately holding his or her breath (in inspiration) to induce fainting as an act of aggression is a misconception.
To complicate matters further, some children seem to have both reflex apnoeic syncope and reflex asystolic syncope, on different occasions. Composite attacks, with crying, expiratory apnoea, asystole and severe syncope, are not rare. Whenever there is asystole—for example, R-R interval of 5 s or more, then reflex asystolic syncope or “RAS” can be diagnosed.5
In addition, we suggest that the term “reflex anoxic seizures” can still be useful in this situation, where it is impossible without ictal ECG to differentiate reflex apnoeic syncope and reflex asystolic syncope. The assertion that “blue breath-holding” and “white (asystolic) breath-holding” are reliably clinically distinguishable is unfounded.
The preliminary genetic data suggest they may be phenotypic variants.23
In practice, the distinction becomes important when therapy (atropine, gylcopyrronium or cardiac pacing) or other causes, such as imposed upper airway obstruction (see below), are considered.
The fainting lark
Another version of prolonged apnoea is seen in older children: the “fainting lark” or “mess trick” is a game played by mid- and older-aged school and college students. Typically the child or young person squats down (on his toes; ankles, knees and hips flexed, head-up), takes several deep breaths until he feels faint then stands up suddenly and holds his breath forcibly against a closed glottis (a valsalva). In some versions a friend leans on his chest, pushing him against a wall at this stage. He then collapses and becomes unconscious.
Valsalva-induced syncope is well recognised also in men with prostatic enlargement who rise at night with full bladders, strain to achieve a urine flow and collapse in the toilet or bathroom. In both, venous return and therefore cardiac output is temporarily impaired.
Compulsive valsalva can occur in children and young people with autism spectrum disorders, especially those with more severe autism and learning difficulties. This can produce syncope and convulsive syncope, easily mistaken for epileptic seizures, especially in this population where epilepsies are more common.
Other forms of syncope (by mechanism or cause)
Cardiac syncope is rare. It is suggested by extreme pallor (like RAS), evidence of injury from the collapse (unlike vasovagal syncope) and an association with tachycardia—for example, with exertion, or sleep, but lack of other triggers. There may or may not be a warning. There are various causes including the long QT syndromes, heart block, other disorders of cardiac rhythm, cardiomyopathies and congenital heart disease—for example, aortic valve disease and aberrant coronary arteries. These can prove fatal, so all patients with any TLOC should have, at least, a cardiac examination and ECG.24
Vascular syncope, caused by a sudden drop in blood pressure—for example, with hypovolaemic shock from a sudden haemorrhage or extensive burns, or with septicaemic shock or anaphylaxis, is familiar to most doctors and nurses. There may be pallor or flushing and typically a tachycardia.
Cerebral syncope refers to syncope due to impaired cerebral blood flow in the presence of a normal systemic blood pressure and cardiac output. This can be recognised in older individuals with severe cerebrovascular disease—for example, on head turning in extension and also in some healthy teenagers and young adults who are able to induce syncope by extending their necks: adolescent stretch syncope.25 26
Important differentials
“Brainstem attacks” are a very important clinical differential for TLOC and may be very difficult to distinguish from convulsive syncope or epileptic seizures by ictal observation alone. Attacks can occur in the course of a complex migraine headache—for example, basilar migraine with a loss of consciousness. They can occur with hydrocephalus with sudden increases in intracranial pressure and/or mechanical distortion of the brainstem: hydrocephalic attacks, or with pressure-induced hindbrain or brainstem herniation. Measurement of the head circumference and determination of the centile for age will demonstrate patients with clinically un-noticed macrocephaly. If present, neuroimaging for hydrocephalus and other structural causes of brainstem dysfunction—for example, tumours, hindbrain hernia, will be needed.
Epileptic seizures may be misdiagnosed from the description or even the observation of a syncope. Furthermore, a mild generalised clonic or tonic–clonic acute symptomatic or reflex epileptic seizure may occur—for example, during the recovery phase.
These are sometimes called anoxic epileptic seizures (see page 66).6
The EEG in a severe syncope—for example, RAS, will demonstrate a normal background, then slowing as consciousness is lost then attenuation of the amplitude (flattening), during the tonic extensor spasm, followed during recovery by slow waves again before returning to normal, seconds or minutes later (figure 1).
Medically unexplained TLOC (including “psychogenic TLOC” or “syncope”)
Medically unexplained TLOC may present in a young person in addition to syncope, especially NMS, or as the only complaint. Features suggesting this diagnosis include multiple episodes in a day and significant increase around times of stress or upset. Investigations such as the head-up tilt test may reproduce symptoms with no correlating physiological abnormalities in heart rate or rhythm, or blood pressure. Ideally, synchronous video and EEG will demonstrate a normal ictal background EEG, including α-rhythm when eyes are shut.
Assessment and investigation
In most cases the diagnosis of syncope, even if convulsive, will be clear if a thorough history of the circumstances of the ictal onset is taken. Population-based studies have found that history and physical examination identified a potential cause of syncope in 45% of patients whose primary disorder can be diagnosed.27
History must be obtained from the patient and from any reliable eye witnesses. The following information should be elicited: the patient's circumstances and activity immediately before the event, any precipitant factors, whether the patient was sitting, standing or lying when it occurred, and any symptoms or aura before the event. A full eyewitness account of events during the actual attack should be taken if possible. “Red flag” symptoms and signs should alert the clinician to the possibility of significant underlying pathology:
Chest pain, dyspnoea, palpitations or structural heart disease.
Syncope during exercise, with swimming, or in or from sleep is typical of the much rarer, but potentially fatal, long QT syndromes.
Low back pain, severe headache, focal neurological deficits, diplopia, ataxia, or dysarthria before the syncope.
Family history of deafness.
Family history of sudden unexpected death.
Particularly important aspects of the systems examination include evaluation of the cardiovascular system for arrhythmias or murmurs and a detailed neurological examination including head circumference (plotted on appropriate chart), fundoscopy, auscultation for carotid bruits and evaluation for cranial nerve deficits, motor deficits, deep tendon reflex asymmetries and sensory deficits.
Supine and standing blood pressure and heart rate should be recorded. Both should be within normal limits and the mean blood pressure should rise on standing. The heart rate often rises on standing also but should remain <120 beats/min and should not rise by >30 beats/min, or 35 beats/min in young people ≤16 years old.11 Excessive orthostatic tachycardia suggests postural tachycardia syndrome, whereas a fall in heart rate or blood pressure on standing may indicate an orthostatic cause of syncope. The systolic blood pressure should not fall by >20 mm Hg and the diastolic should not fall by >10 mm Hg after a minute of standing.28
If seen acutely, the patient must be examined for signs of trauma. If history or findings are unclear, the possibility of head trauma resulting in loss of consciousness as opposed to syncope resulting in trauma should be considered.
The Hallpike manoeuvre may be performed in patients who describe short, intermittent prodromes with primarily vertiginous components to assess for benign positional vertigo.29
Investigations
Video-recording the event
Video-recording an episode may help to identify the cause for a TLOC.30 With the widespread use of mobile telephones incorporating video cameras, there is a high likelihood of being able to obtain a simple home video-recording of an episode. If necessary, video-recording at the same time as physiological monitoring can improve the diagnostic yield.
Electrocardiogram
We recommend a 12-lead ECG for every patient presenting with TLOC.31 If there is any doubt about the diagnosis, the ECG should be reviewed by a paediatric cardiologist or a paediatrician with expertise.32 ECG and rhythm recordings obtained in the emergency department yield a diagnostic rate between 1% and 11% (mean 7%).33
ECG evaluation is particularly important if long QT syndrome is a possibility.34 If events appear to be related to exercise or stress and a standard ECG is normal, an exercise ECG should be performed.
Lightweight external digital loop cardiac monitors
Portable cardiac monitors are helpful if symptoms occur around once a week or fortnight; beyond this timescale, compliance with wearing the device decreases. Capturing the heart rhythm during an episode is helpful in identifying cardioinhibitory NMS, such as syncope with asystole. They can also be useful in the rare cases where repeated episodes of TLOC are caused by imposed upper airway obstruction/intentional suffocation.35
Attacks that are significant but occur less frequently can be captured using a surgically implantable digital loop recorder. This can monitor the heart for up to 18 months.
The increased availability of digital loop recordings means that Holter monitors are indicated less frequently. Holter monitors record the heart rate and rhythm continuously for, usually, 24–48 h as opposed to digital loop recorders that also monitor continuously but record only the few minutes preceding and after any events marked.
Head-up tilt-table testing
This can be useful in the evaluation of severe or frequent TLOC or syncope and can generally be performed in children >6 years of age. The patient is gently strapped on to a tilting bed with foot-plate. Head-up tilt to 60°–80° upright position is performed after a period of 10–15 min relaxation in the supine position. The tilt is maintained for 20 or 45 min, during which time various physiological parameters are monitored including ECG, heart rate and blood pressure.36 Other investigations during this period may include video, best to beat blood pressure, cardiac output, EEG, respiratory function and oxygen saturation.
If the patient's typical symptoms occur together with physiological confirmation of a cardio-inhibitory syncope, vasodepressor syncope or mixed syncope, this is considered a “positive” test. If typical symptoms occur in the absence of physiological changes, this is a “negative but symptomatic” test and suggests episodes could be due to cerebral syncope—for example, adolescent stretch syncope, hypoxia, or psychogenic or unexplained TLOC.
Echocardiography
Echocardiography should be performed in patients with any features suggestive of structural heart defects, including abnormal ECG findings or abnormal cardiovascular examination findings.
Electroencephalography
An interictal EEG should not be requested for any patient in whom the likely diagnosis is syncope. Misinterpretation of EEG is one of the major reasons for misdiagnosis of epilepsy.37 38 “Epileptiform” abnormalities on EEGs, which include spikes or sharp waves or spike and wave discharges, can occur in healthy children who do not have epilepsy and in those who have syncope but not epilepsy.39 40
An ictal EEG can be useful in the investigation of TLOC. During head-up tilt testing, the presence of ictal slow waves confirms syncope, whereas a normal ictal EEG pattern demonstrates medically unexplained or psychogenic TLOC.
An ECG channel added to an EEG recording will help in identifying rhythm abnormalities resulting in TLOC.41
Brain MRI or CT
Cranial imaging does not form part of the routine investigation of children and young people with TLOC unless there are reasons for suspecting abnormalities, such as signs of raised intracranial pressure or new focal neurological deficits.
Treatment/management
Management will be guided by the underlying cause. Patients with NMS should be given a clinical diagnosis and explanation as to the likely underlying mechanism, together with reassurance that the attacks in themselves, although they can be frightening and a source of stress and anxiety, are not life-threatening. Participation in normal activities should be encouraged with advice regarding general measures to minimise or abort syncopal attacks.
Known triggers such as dehydration, tight clothing and environments that are too warm should be avoided.31
If the patient is aware of presyncopal symptoms, he or she should be taught manoeuvres to abort syncope including crossing and squeezing the arms and legs, or squatting down, to increase systemic blood pressure.42
Fluids, salt, fludrocortisone
Increasing fluid intake until the urine is clear and colourless and increasing dietary salt intake are simple measures to improve orthostatic tolerance. Additional salt can be taken as slow sodium tablets (50 mmol, ie, 3 g twice daily). If these measures are not effective, fludrocortisone, which promotes renal reabsorption of sodium resulting in water retention and an increase in blood volume, can be given at a dose of 100 µg twice daily up to a maximum of 1 mg/day.43
Other medications are also used, and before commencing a specific treatment, full consideration should be given to the underlying diagnosis as well as to the significance of the attacks including their impact on everyday life and family activities.
β-Blockers
A common trigger for an episode of vasovagal syncope is thought to be the activation of cardiac mechanoreceptors by an increase in adrenergic tone. β-blockers may prevent the activation of the left ventricular mechanoreceptors and thus block the initial increase in adrenergic tone and negative inotropic effects. Randomised controlled trials have failed to demonstrate their efficacy, possibly in part because they may actually worsen syncope through their negative chronotropic effects.44
α-Agonist. Midodrine increases venous return through increasing peripheral vascular resistance. Avoid evening doses close to bedtime because lying down can lead to hypertension. Typical doses for young people and adults range from 2.5 to 10 mg two to three times a day. Smaller doses would be appropriate for younger children—for example, 40–150 µg/kg two to three times a day. Its efficacy and safety in treating paediatric NMS has been demonstrated.45
Antimuscarinics
Atropine or glycopyrronium can be helpful in cardioinhibitory syncope—for example, reflex asystolic syncope (an ictal ECG should be obtained to confirm the presence of asystole). Atropine sulphate 20–40 µg/kg two to four times daily may reduce the number and severity of attacks, although dose may be limited by anticholinergic side effects.46 Glycopyrronium 40–100 µg/kg three to four times a day has also been used.
Cardiac pacing
For very intrusive or disabling attacks associated with significant asystole or with a major vagal component and little drop in peripheral vascular resistance, cardiac pacing may be considered when medical treatments have failed. Perioperative risks are minimal; however, as the child grows, the leads may need removal with or without replacement. Because RAS and other cardioinhibitory syncopes are not fatal, there must, as always, be careful consideration of risks versus benefits of treatment.47 48
Conclusions
Recurrent syncope can be distressing and disabling for a child or young person and their family. Although many forms of syncope have an underlying “benign” cause, there are important potentially life-threatening differentials that must be considered when assessing a patient with syncope. Selected investigations may help to elucidate the underlying mechanism and thus inform treatment options. A detailed history and eye-witness account are key to save inappropriate and potentially confusing use of—for example, EEG for non-epileptic convulsive episodes.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed
-
Patient consent Obtained.