Article Text

Abstract
Insulin pump therapy is a current treatment option for children and adolescents with type 1 diabetes. Insulin pumps can provide a greater flexibility in insulin administration and meal planning, as compared with multiple insulin injections, and they may be particularly suitable for the paediatric age group. Many young people with diabetes have integrated insulin pumps into their daily practice. The use of insulin pumps can also be supplemented by the information retrieved from continuous glucose monitoring in the sensor-augmented pump therapy, which may improve glycaemic control. In this review, we describe the principles of pump therapy and summarise features of commercially available insulin pumps, with focus on practical management and the advantages and disadvantages of this technology.
- Type 1 Diabetes
- Paediatric Practice
- Insulin Pumps
- Sensors
Statistics from Altmetric.com
Introduction
The Diabetes Control and Complications Trial provided conclusive evidence that strict glycaemic control reduces the development and progression of complications in patients with type 1 diabetes mellitus (T1D).1 Optimal diabetes control requires replacement of insulin that mimics normal physiology, in a basal bolus regimen, as either multiple daily injections (MDIs) or a continuous subcutaneous insulin infusion (CSII). CSII or insulin pump therapy is now well established and accepted as a safe therapeutic option to deliver insulin in toddlers, children of preschool age and adolescents with T1D.2 ,3
Although data from paediatric studies of CSII show contradictory results in terms of improvement in HbA1c and incidence of hypoglycaemia,4–6 it provides flexible insulin administration which may be particularly suitable for young children, who have unpredictable eating and exercise patterns. In addition, beneficial effects of insulin pump therapy on quality of life and fear of hypoglycaemia have been described in both parents and children.7
NICE guidelines
Guidance on the use of CSII, published by the National Institute for Health and Care Excellence (NICE) in the UK in 2003, recommended it as an option for people with T1D where MDI had ‘failed’ (it had been impossible to maintain HbA1c below 58 mmol/mol (7.5%)).8 That guideline was updated in July 20089 with the indication that CSII could be recommended in children with T1D aged 12 years or older where either attempts to achieve target HbA1c levels with MDI resulted in disabling hypoglycaemia or where HbA1c levels remained high (>69 mmol/mol (8.5%)). CSII was also recommended in children younger than 12 years with T1D when MDI is considered to be impractical or inappropriate. However NICE recommends that this group of children would be expected to undergo a later trial of MDI between the ages of 12 years and 18 years. Although currently not recommended by NICE, CSII may be the treatment of choice in those younger than 5 years where MDI may be difficult for parents10 and review of NICE recommendations is currently underway. Although these UK guidelines may not apply to other countries, with differing levels of reimbursement for CSII, they reflect overall evidence based guidelines.
Increasing use of insulin pumps
The use of insulin pump therapy has increased in most countries, with around 40% of people with T1D using insulin pumps in the USA but there is a substantial variation in usage within Europe.5 At the time of the 2003 NICE guideline, it was estimated that around 1%–2% of people with T1D in the UK would be expected to use CSII. However, the first UK audit of insulin pump use, supported by the Association of British Clinical Diabetologists, Diabetes UK and Juvenile Diabetes Research Foundation, published in May 2013, revealed that 19% of paediatric patients with T1D are on CSII.11 Overall, the uptake has been much better in children than in adults (7%), but it generally falls behind the uptake in most Western European countries and North America.5 Possible reasons for this difference may be the reduced availability of funding or reduced resources to support the use of insulin pumps in the UK, that is, a lack of trained professional staff with CSII expertise.
With the recent introduction of best practice tariff in the UK for children with T1D, appropriate use of resources, improved commissioning, establishment of paediatric diabetes regional networks, improved training of health professionals and national initiatives to improve access to CSII,12 it is anticipated that CSII use in the UK may catch up with other European countries.
As a result of these developments, paediatricians and paediatric trainees will be increasingly exposed to children on CSII in acute care settings. It is important for these healthcare professionals to familiarise themselves with the basic principles of CSII and management issues related to this form of insulin therapy.
Principles of pump therapy
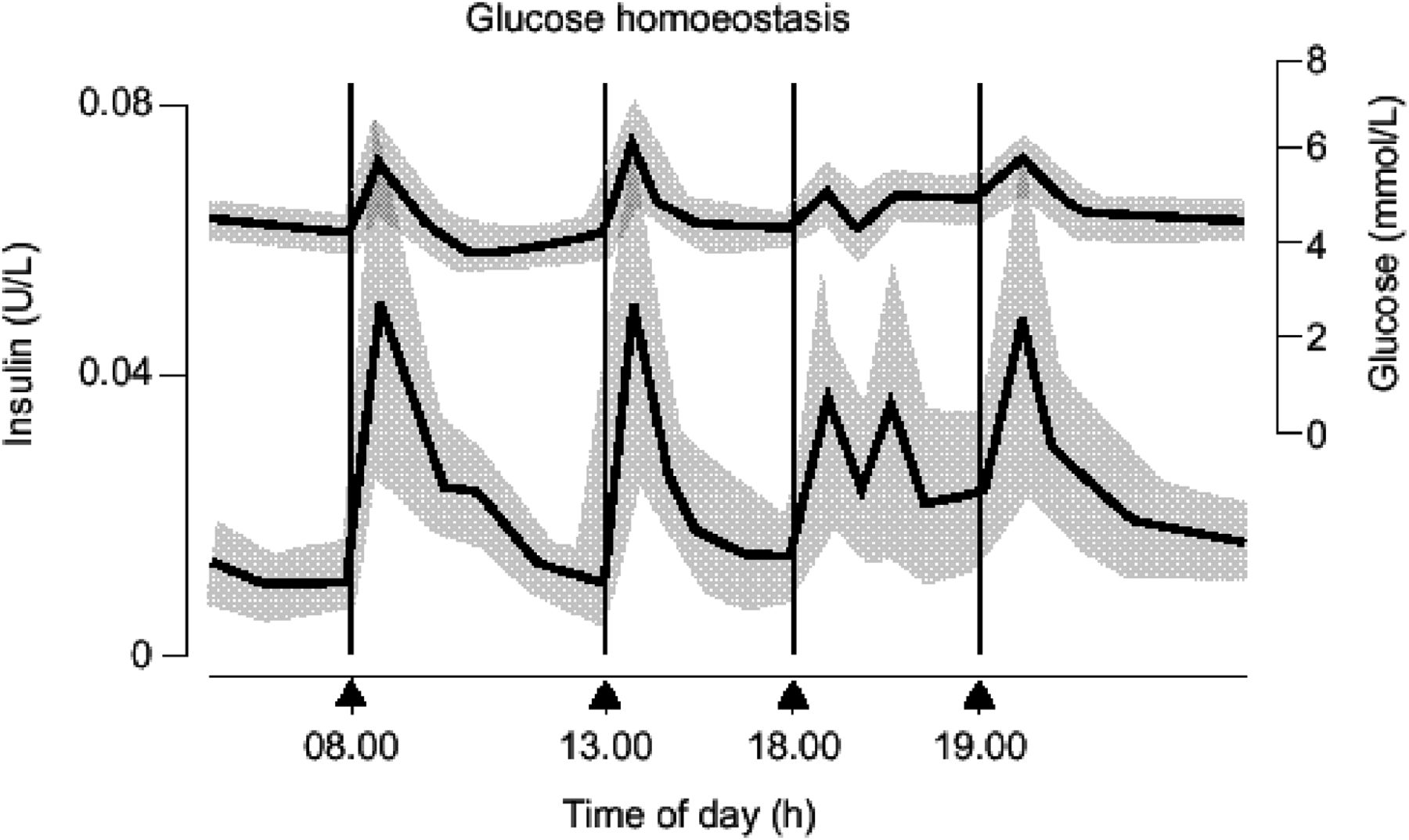
In a person without diabetes, the pancreas produces small amounts of insulin (basal insulin) continuously throughout the day to suppress hepatic glucose production and a larger amount of insulin is required when a meal or snack is eaten (figure 1).
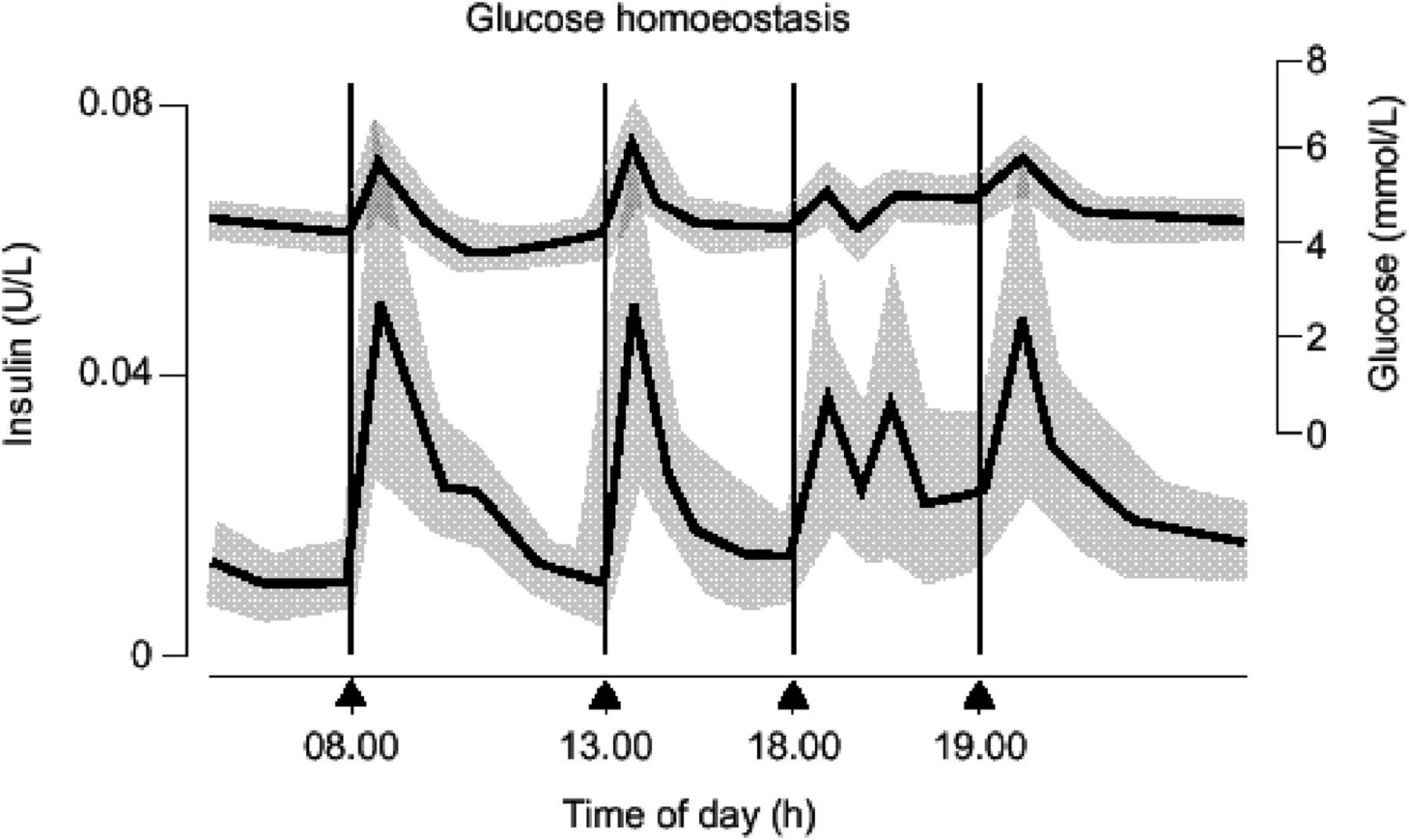
Normal glucose and insulin excursions related to meals and during fasting. Adapted from Owens et al.13
Insulin delivery via an insulin pump aims to mimic this physiological basal-bolus pattern. Insulin pump therapy can be commenced as early as at diabetes diagnosis, where the total daily insulin dose is more typically calculated as 0.3–0.5 units/kg to reflect lower insulin requirements during the honeymoon period. The total daily dose can be divided into continuous basal delivery and premeal insulin boluses, as described below.
Insulin pumps are devices with extremely reliable software, which are reasonably small in size (to fit in the pocket or clipped to a belt or clothing) and can be used to deliver insulin in response to these physiological requirements. A reservoir is filled with a rapid acting insulin analogue (insulin lispro (Humalog) or insulin aspart (NovoRapid) or insulin glulisine (Apidra)). The insulin is then delivered through an infusion set placed in the subcutaneous tissue which is changed every 2–3 days. The infusion set can be placed in any of the sites recommended for insulin injections (figure 2).

Drawing representation of insulin pump and infusion set. Adapted from http://diabetes.niddk.nih.gov
Basal insulin
The ability to deliver preprogrammed basal insulin, to meet increased or decreased demands all through 24 h, is particularly important in paediatric practice due to the wide range of insulin requirements, relating to puberty and other physiological factors.14 In addition, the basal insulin requirements can be programmed to give different amounts at different times of the day. Basal rates can be increased during early morning to prevent the rise in blood glucose (BG) before breakfast associated with the dawn phenomenon15 or decreased during exercise or at other times when hypoglycaemia is anticipated. The basal rates can be adjusted every 30 min; however, in practice, five to eight adjustments in any 24 h are sufficient.
The contribution of basal insulin to the total daily dose is dependent on the age of the child.16 ,17 There are several rules for calculating the basal insulin requirement but the most commonly adopted principle is to calculate the total daily insulin requirement on their previous insulin regimen, which is typically in the range of 0.5–1.5 units/kg/day and then using 30%–50% of this figure to calculate basal insulin requirement.18 Typical basal rates by age are listed in table 1.
Daily insulin and basal insulin requirement by age group (mean±SD)19
Bolus insulin
Insulin pumps can deliver extremely accurate doses of insulin as a bolus (as little as 0.025 units) and this allows the patient to administer a frequent number of boluses every day, providing more flexibility around eating times and boluses before snacks.
Pump bolus calculators integrated within the infusion devices allow calculation of the bolus according to expected carbohydrate (CHO) intake and current BG level. CHO counting is required to help determine the amount of food related insulin bolus and there are several tools (nutrition labels, measuring spoons, weighing scales, calculator, reference books, software programs and many apps for Android and Apple devices) to help patients and parents calculate the CHO content of the food. However, every person responds differently to insulin which means that any two people with diabetes can have quite different insulin-to-CHO ratios (ICRs) (ICR: the amount of CHO that 1 unit of rapid acting insulin can cover). For young children, 1 unit of rapid acting insulin may cover 20 g of CHO, whereas for adolescents it may cover only 10 g. Healthcare professionals typically estimate a starting ICR by calculating the total insulin dose per day and dividing this by the total CHO consumed per day, which can then be adjusted depending on the time of day. The 500 rule (500 divided by the total insulin per day equates to 1 unit of rapid acting insulin for every x grams of CHO) is typically used to calculate ratios for children on CSII.20 For very young children, some clinicians use the ‘300–450 rule’ to allow more insulin with the meal boluses.21
Patients are also advised to use ‘corrective doses’ of bolus insulin if BG levels are above targets before meals. The insulin sensitivity factor helps to calculate the dose of rapid acting insulin required to correct high BG above the target range. It is calculated by using the ‘100 rule’ where 100 is divided by the total daily dose.20 Based on previous observations in that patient, they predict the drop in glucose in mmol/L for every unit of rapid-acting insulin delivered by the pump.
Commonly used advanced features of pump therapy
Regular pump users, particularly children may be aware of other pump features advised by healthcare professionals that may mystify the general paediatrician. These might include:
-
Keeping track of bolus doses: in order to make sure that the cumulative dose of insulin from boluses is not excessive, pump software tracks insulin administered. There are several terminologies used for this concept, depending on the type of the pump (insulin on board (Animas, OmniPod), active insulin (Medtronic) acting time (Roche)).
-
Temporary basal rates: a temporary basal rate follows the normal basal rate pattern, but allows either higher (when BG levels are high or during management of ketonaemia) or lower (when BG levels are low, during or after exercise) basal rates. This allows flexibility to plan activity at short notice especially in younger children when activities are unpredictable.
-
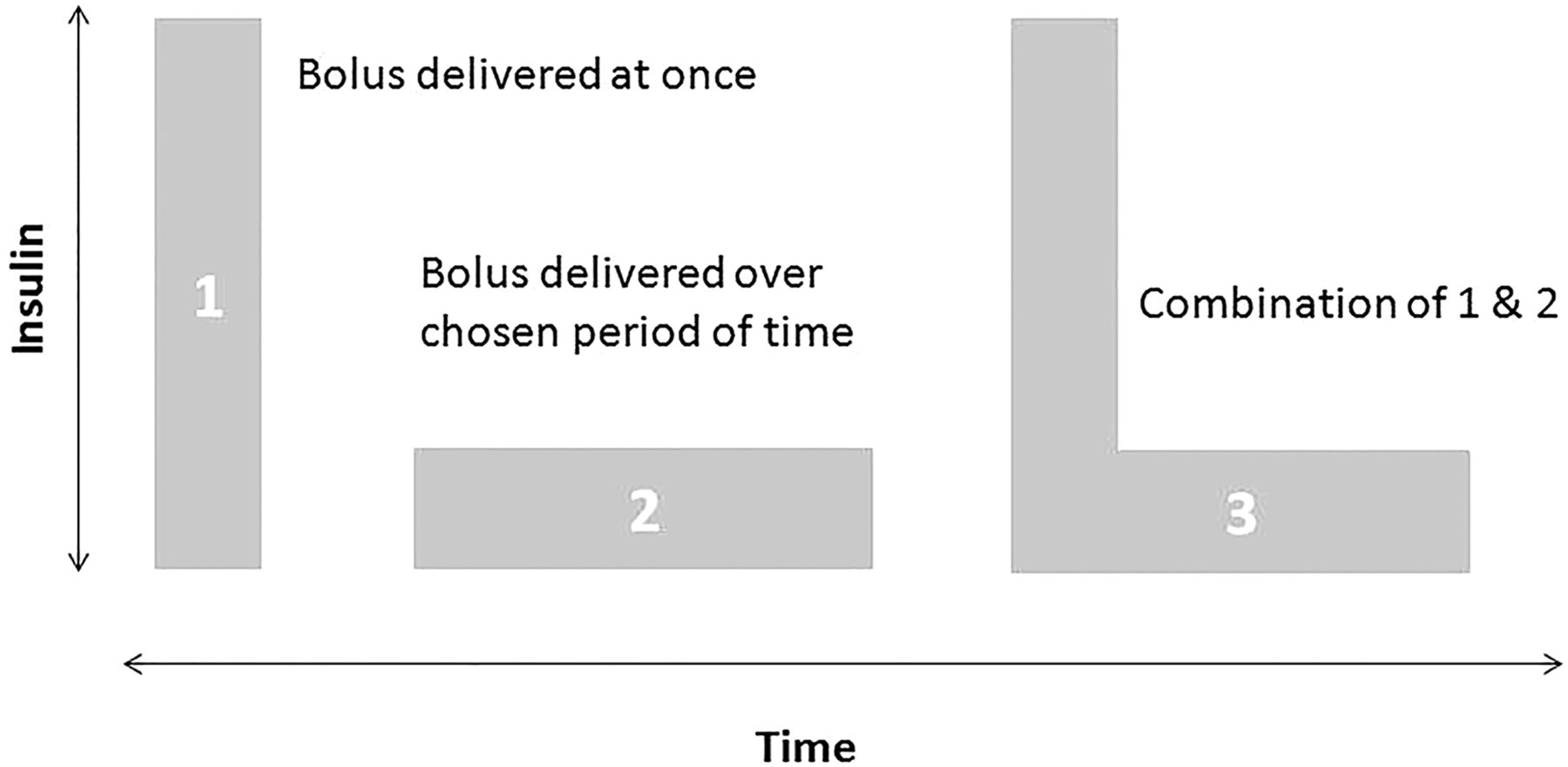
Bolus types: the insulin pump may also permit changes in the profile of delivered insulin after the meals to keep the BG in target range. There are three types of boluses, and different manufactures use different terminologies (figure 3).

Drawing representing three types of insulin boluses. There are several terminologies used for these three types of boluses depending on the type of the pump. (1) Normal (Animas, Medtronic, OmniPod) or Standard (Roche) bolus. (2) Extended (OmniPod, Animas, Roche) or Square Wave (Medtronic) bolus. (3) Dual Wave (Medtronic) or Combo (Animas) or Multiwave (Roche) bolus or Extended (OmniPod).
These bolus types will have been recommended by the physician/diabetes educators to cope with different types of meals, according to the glycaemic index, protein and fat content, in response to difficulties in achieving good postprandial glycaemic control. For example, a meal that is high in fat and protein content, like a roast dinner, pizza or Chinese takeaway, might be best managed by a dual-wave or extended insulin bolus.
What types of insulin pumps are available?
Currently five Conformite Europeenne marker insulin pumps are available in the UK and most other countries. They are summarised in table 2, together with links to their specifications.
A list of the most commonly available models of insulin pumps and their specifications
Should we continue insulin pump therapy during hospital admissions?
It is recognised that patient satisfaction is high when CSII is continued during inpatient care in the hospitals22 and where possible this should be achievable.23 ,24 Most paediatricians may be unfamiliar with wide variation in insulin pump models and their particular features; however, most patients and parents are very competent in managing pump technology and can be expected to self-manage technical aspects of the device in the hospital setting.25 Healthcare professionals should also be aware that the technical advice is provided by all manufacturers of insulin pumps 365 days a year, including weekends and holidays.
Nevertheless, there are certain circumstances when CSII is considered to be unsafe or contraindicated in the hospital settings (box 1).
Contraindications for the use of continuous subcutaneous insulin infusion (CSII) in the hospital settings
-
If parents or carers are unable to support care
-
In a critically ill child
-
During management of diabetic ketoacidosis (DKA)
-
Any other circumstances identified by the healthcare professionals where an intravenous insulin infusion is required to achieve finer control of blood glucose levels
Advantages and disadvantages of insulin pump therapy, sensor augmented pump therapy and closed loop insulin delivery
CSII provides a logical and relatively non-invasive method for delivering basal bolus insulin therapy but it is not suitable for all children, adolescents and their families. The potential advantages and disadvantages of CSII are summarised in box 2.
Advantages and disadvantages of continuous subcutaneous insulin infusion (CSII)
Advantages
-
Flexibility in meal times and increased number of boluses with every meal/snack
-
Programmable basal rates allow varying amount of basal insulin at different times of the day
-
Useful tool to prevent severe overnight hypoglycaemia in children and in those with hypo unawareness
-
Improved quality of life
-
Reduces the day-to-day variability in blood glucose profile
-
Insulin pumps store the accurate record of insulin delivery: basal and boluses
-
The stored record can be downloaded and is helpful in providing advice to patients and in determining any missed boluses
-
In very young children precise amount of insulin (0.025 units) can be delivered
-
Alternative therapy in children with extreme needle phobia
-
Management of exercise and unpredictable activity is easier by using temporary basal rate
Disadvantages
-
Needs to be attached 24 h a day
-
Pump cannot be taken off for more than 1–2 h
-
As pump contains only rapid acting insulin, any interruption in the delivery of insulin increases the risk of DKA
-
Possible risk of infection at the cannula site
-
Requires more motivation and family support than multiple daily injections
-
Body image issues
-
Demands extra support and commitment for successful therapy
-
Management of CSII at schools is very demanding
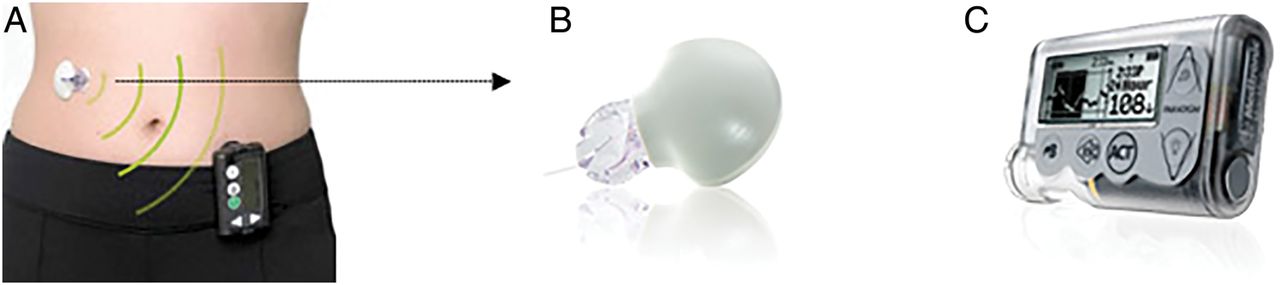
With further technological developments, paediatricians may encounter other variation in insulin delivery, such as sensor-augmented pump system,26 which combines the insulin pump and continuous glucose monitoring system (CGMS). CGMS involves the small insertion of a subcutaneous sensor that records BG levels every few minutes throughout 24 h and displays the result on the handheld monitor or directly on the insulin pump (figure 4). The sensor needs to be replaced after every 3 days of use, however, in some patients it lasts for up to 7 days.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sensor augmented pump system. The continuous glucose monitoring system (A,B) transmits blood glucose readings on the insulin pump (C). Courtesy of Medtronic.
Future technological advances may involve linking CGMS with insulin delivery to sensor data in an automated fashion. The commercially available Paradigm Veo insulin pump/CGMS (Medtronic Diabetes, Northridge, California, USA) is equipped with a low glucose suspend function, which automatically stops insulin delivery when hypoglycaemia is detected and the alarm is not acknowledged. The incidence of hypoglycaemia was shown to be reduced with the use of this system in children and adults with T1D.27
‘Closed-loop’ delivery of insulin is an emerging therapeutic approach to achieve normal glucose levels.28 A closed-loop system combines glucose sensing and insulin pump delivery, via an algorithm, which directs insulin delivery in a glucose-responsive fashion. Research studies demonstrated that a closed-loop system can improve glucose control and reduce the risk of hypoglycaemia and long-term studies in the home settings are awaited.29 ,30 These advances will provide additional challenges for those delivering routine diabetes care. However, in the emergency setting, closed-loop therapy may be discontinued and standard pump settings can be re-established.
Test your knowledge
-
How is basal insulin supplied through the pump?
-
By filling the cartridge with long-acting insulin analogue
-
By providing 24 h continuous insulin delivery using rapid-acting insulin analogue
-
An insulin pump can only deliver meal insulin boluses
-
-
How is the basal insulin dose usually calculated?
-
As 10% of total insulin requirement
-
As 30%–50% of total insulin requirement
-
The total insulin dose is delivered as basal insulin via the pump
-
-
How often does the pump cannula need changing?
-
Only when the insulin cartridge is empty
-
Once a day
-
Every 5 days
-
Every 2–3 days
-
-
How can the insulin doses for meals (insulin-to-CHO ratios) be calculated?
-
By dividing 500 by the total daily insulin dose (‘500 rule’)
-
By dividing 100 by the total daily insulin dose (‘100 rule’)
-
By weighing the meal and giving 1 unit of rapid acting insulin for each 10 g in weight
-
-
A closed-loop system:
-
Has only been evaluated in clinical studies involving adults and has never been tested in children and adolescents
-
Combines glucose sensing and pump insulin delivery via an algorithm which directs insulin delivery in a glucose-responsive fashion
-
Is a device which delivers insulin regardless of glucose levels
-
Answers to the questions are at the end of the references.
Appendix
Answers to the quiz on page 219
-
1 (B); 2 (B); 3 (D); 4 (A); 5 (B).
References
Footnotes
-
Contributors NA researched data, wrote the article and provided a substantial contribution to discussion of content, reviewing and editing the manuscript before submission. CP researched data and provided a substantial contribution to discussion of content. DE researched data, contributed to discussion of content, reviewing and editing the manuscript before submission. DD provided a substantial contribution to discussion of content, reviewing and editing the manuscript before submission.
-
Funding Support was provided by the NIHR Cambridge Biomedical Research Centre.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.