Article Text

Abstract
This study considers different ways of maximising learning opportunities during ward rounds, with particular emphasis on the strengths and challenges of the paediatric environment. The focus is on the most common types of ward round – in acute units involving predominantly trainees – but we hope there will also be much that will interest those who work in other settings such as community clinics. Alongside a review of the best available evidence from the literature, and underpinned by educational theory, suggestions for maximising learning on ward rounds are presented. Many of these ideas were generated from working in small groups with over 90 experienced paediatricians, each with particular experience and interest in medical education, as part of the Royal College of Paediatrics and Child Health's Paediatric Educators' Programme, the PEP.
Statistics from Altmetric.com
Background
With the need to balance learning needs against service requirements, teaching on a ward round has been described as being like delicately walking a tightrope.1 In 1959, in a Royal Society Lecture, Jennett lamented at the lack of recognition good teachers received for their great instruction on ward rounds. ‘Participation is key and (a ward round) should not just be a mobile lecture…“walking the wards” was a nineteenth century expression’ he said; are we still plodding the same path in the 21st?2
Changes to the training of junior doctors have increased the need to maximise the educational opportunities available during routine work.3 Every acute paediatric service has inpatient beds and with this is the need for a daily (at the very least) review of the patients. Indeed, a consultant review of every paediatric admission within 24 h is now a specific Royal College of Paediatrics and Child Health (RCPCH) recommendation.4 This gives the ward round an opportunity to provide learning on the back of its important service role. However, there is a tension between the model of a consultant-delivered service and that of a learning ward round. While the daily presence of a consultant on a ward round may provide regular high-quality training, support and learning, there are situations where the presence of the consultant stifles opportunities for trainees to experience decision-making and independent thinking. Ultimately, the ward round has to fulfil both roles; the business requirements of providing care and the need to open up teaching and learning opportunities.
This study considers different ways of maximising learning opportunities during ward rounds, with particular emphasis on the strengths and challenges of the paediatric environment. This study explores different types of ward round and the ideas presented should be of interest to paediatricians working in a variety of different settings.
As an educational initiative to improve the quality of education and training in paediatrics in the UK, through supporting the development of educational leaders, the Paediatric Educators' Programme (PEP) was introduced by the RCPCH in 2007.5 Nearly 100 paediatricians have completed the PEP courses, brainstorming ideas and sharing their experiences. The authors have collated the themes from these discussions, drawn on the experiences of the facilitators leading the course and explored published literature to seek out previous work in this area.
Methods
We worked with about 90 paediatricians drawn from across the UK and Ireland, each with a particular experience and interest in medical education and selected for the PEP programme based on submission of precourse reflective portfolios detailing their previous educational experience and learning needs.5 During the programme, the participants worked in small groups to consider learning and teaching in ward rounds as part of a situational learning session. They were prompted to consider three areas, drawing inspiration and examples from their own experience, for each type of ward round as described in table 1:
(1) pros – what is good about the learning possible in that type of ward round;
(2) cons – where the pitfalls and problems are for that type of ward round;
(3) how to innovate the various types of ward round and enhance the teaching–learning experience.
Definition of different types of ward round
Each group was facilitated by one of the authors (AR) and another facilitator. The themes and ideas were analysed in a similar way to that described previously.6 While many of the candidates had good ideas about teaching and learning on ward rounds, there was some overlap with service needs of a ward round. In analysing the information gathered during these sessions, attention was diverted from these to concentrate on the educational issues.
Introduction
Definitions
O'Hare described a ward round as ‘a parade through the hospital of professionals where most decision-making concerning patient care is made’,7 but the traditional concept of a ward round can be more specifically defined as follows:
‘a service-driven clinical review of any patient admitted to hospital and residing in an inpatient ward. The patient is usually receiving specific treatment or care, and is seen or discussed in turn by the attending medical team. The round is often led by a consultant, and may involve other members of the multidisciplinary team’.
While traditional ward rounds could be considered to be all about the senior physician's interaction with the patient, with an entourage of junior doctors and nursing staff ‘hanging off the consultant’s coat tails', the health service of today has different emphasis. There is now a universal need to quality assure documentation, communicate effectively and involve the patient in all aspects of their care.
For the purpose of this study, the components of the ward round will be discussed as three distinct entities as listed in table 1. Ward rounds in reality might be a blend of these aspects.
Each of these components has their merits. The first two are part of the same process but in considering the educational value, there are reasons for the distinction.
Similar rounds occur, for example, on the neonatal and intensive care units, but in a community paediatric service, the multidisciplinary case meetings are usually a sit-down discussion. This is often replicated in the acute services in the form of a sit-down ‘grand round’ where the patient information is presented verbally or displayed digitally. This might apply more closely to a case meeting or to a multidisciplinary developmental assessment review in the community paediatric clinic.
Literature review
The ward round continues to be an important part of the clinical care of patients, and it also remains a source of training and education. A survey of 608 doctors reported over half of Senior House Officers (SHOs)and over three-quarters of consultants regarded the consultant-led ward round as a learning method upon which most SHOs rely.8 Stanley reported on different ward round experiences (including from paediatrics and neonatal units) gathered from a survey of practices in four hospitals in the mid-1990s.9 In the context of on-the-job learning, she described variation in the ward round structures which not surprisingly contributed to a considerable variance in learning experience. She suggests planning premeeting or postmeeting or both around a ward round (sometimes called ‘prebrief’ and ‘debrief’) to be able to adapt the ward round structure to one that best maximises the participation and learning for all participants. Learning how to structure and run ward rounds is a skill that can be acquired. Weaknesses in ward round skills in final year students have been described, suggesting more resource should be directed at encouraging development in this area before and immediately after graduation.10
Prado et al report that the use of more active learning methodologies are beneficial in a paediatric ward round, compared with traditional ward round teaching in three measured outcomes (their knowledge acquisition, whether they were stimulated to do self-directed learning and the student's opinion on whether the methods improved their knowledge).11 Other novel methods of teaching and learning on a ward round have included using standardised patients in a simulated ward round, the use of video recording on ward rounds to enhance on-the-job teaching and learning and techniques to promote safe prescribing on ward rounds.12,–,14
Teaching on-the-job has its challenges, but integrating workplace-based assessments (WPBAs) or some form of structured feedback into service provision can be a useful way of orientating the team to what is expected and how they can perform better.15 The strategy of using the post-take round as a model to review the night's work has been completely disempowered by the changes in current working patterns.16 In its place, structured handover, and the potential learning within it, has emerged.6
Underpinning educational concepts
Applying best evidence to a clinical education situation such as a ward round requires a look at some of the educational theories that underpin much of teaching and learning.
In planning opportunities for teaching on ward rounds, we can seek some support from Maslow and his ‘Hierarchy of Needs’. The best example would be the early morning breakfast meetings which, through feeding the assembled learners, ensure one of their basic needs are met. More specifically relating to the education, one needs to consider the environment (clearly more comfortable in the sitting-down round), before moving up the hierarchy to consider other needs, such as whether learners feel ‘safe’ to actively contribute to discussions.17
The ward round is a good example of what Lave and Wenger called ‘legitimate peripheral participation’.18 The concept of legitimate peripheral participation means that learners start out on the ‘outside’ as observers, being allowed ‘in’ as their skills and knowledge increase. Eventually, over time, they become an integral part of the team. The key to maximising learning is to be allowed to watch, observe and develop the necessary skill set to then be included as a valuable (legitimate) person in the group. There are many simple practical ideas that can build on these theories. One example is the simple action of introducing every member on the ward round by name to each and every patient. This can help to flatten the traditional ward round hierarchy and to help to bring ward round participants ‘inside’.
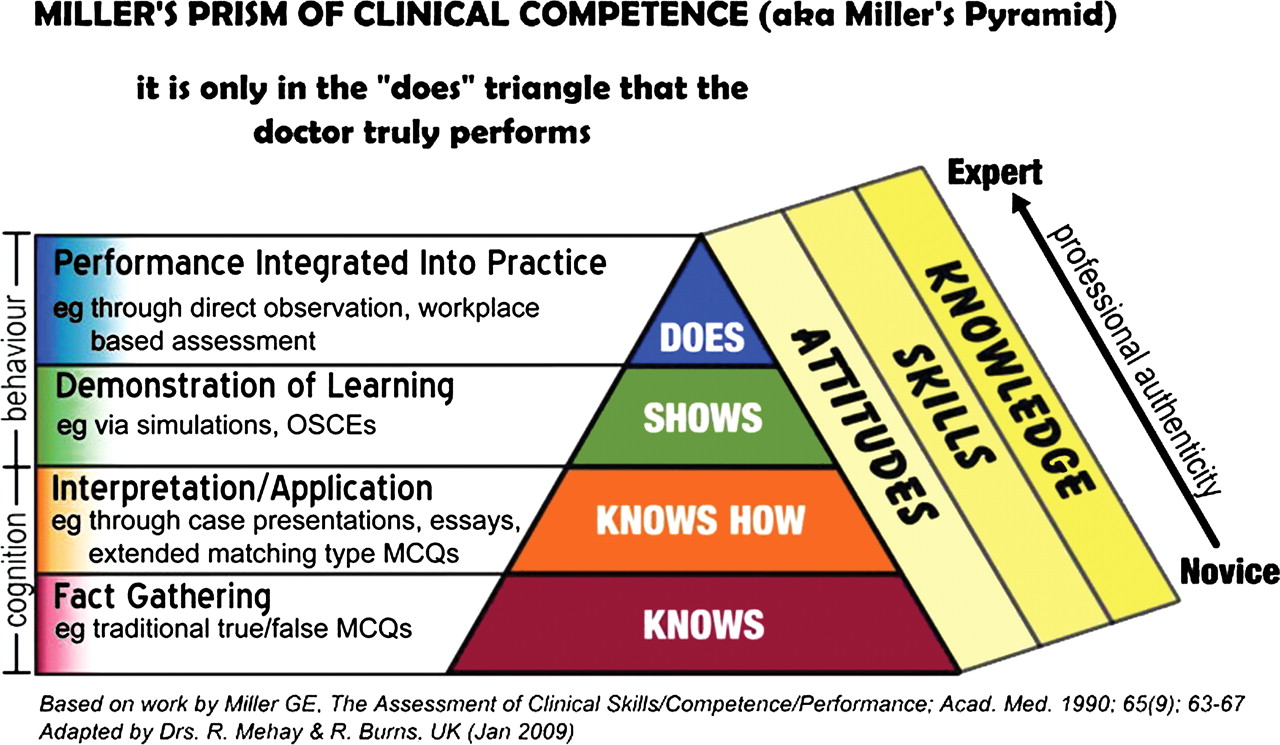
Ward rounds also present opportunities to observe and assess clinical skills in junior doctors that are high on Miller's pyramid (figure 1).19 For a controlled artificial scenario, using simulated patients, Miller suggested a student can be allowed to perform a clinical skill and be assessed on their performance, as if it was a real-life clinical situation. His model of assessing clinical competence begins with knowledge as a base and moves upward through different levels of ‘knowing how’, ‘showing how’ and ending at the pinnacle, ‘doing’ the skill being assessed. The triangle has become a pyramid as extra faces have been added including a thread of knowledge, skill and attitude running through all the levels.
{kind=link}
Miller's ‘pyramid’ of clinical competence, portrayed here as a prism.
There is some overlap here with the Dreyfus and Dreyfus model (and Eurat's refinement) which describes how individuals progress through various levels in their acquisition of skills from novice to expert and how individuals learn. Such a model is used to explain the ‘acquisition’ of clinical skills.20 21
Learning and the paediatric ward round
The paediatric environment
Challenges/problems for effective and efficient learning
While the ward environment is common to many specialities in some form or other, there are specific issues for paediatrics. Inpatient paediatrics involve short stays and rapid turnover where most of the patients are new to the incoming team on the next shift. There are issues of being able to effectively examine children in the presence of a large group and the challenges of medical students approaching parents to ask for their consent to examine their sick child.22 23 Time is an important factor with tension between service requirements to see, assess, review and discharge patients against the need to teach, train and inform on the ward round.
Strengths provided by the paediatric environment
Having acknowledged there are difficulties in teaching on paediatric ward rounds, there are also many advantages. Ward rounds are a great opportunity for modelling of behaviours, communication and clinical skills, as well as real-time learning. Those less familiar with the nuances of interacting with children and young people of various ages can be shown how it can be done by senior members of the team. There is also the opportunity to role-model real-time interview, discussion and counselling of children, parents and carers. Senior review of clinical notes and documentation to ensure standards are being met offers another avenue for feedback and learning. It is possible to bring other learners such as medical students and nursing colleagues into discussions when moving between patients. The opportunities to present children previously assessed in preparation for presentation on a round is good training, especially in a grand round. This can then springboard further thoughts and discussion which may not be appropriate at the bedside and may be too time critical at the trolley. Sharing challenging cases with senior colleagues in a grand round environment, who may have specific specialty expertise, can be invaluable.
There are many tasks on ward rounds including determining care plans, reviewing and writing notes, checking drug charts, listening to presentations, teaching consultation and physical examination skills, seeing the patients and talking to families.24 All of these, if well structured, can be used as a training opportunity on a paediatric ward round.
For each type of ward round detailed in table 1, the relevant pros and cons are included in tables 2–4 in various areas (patient factors, environment, confidentiality, teaching and team factors). There are also innovations to try and invigorate the different type of round suggested which may give rise to solutions for your own teaching and learning challenges within your own environment.
Trolley/board round
Sit-down ‘grand round’ discussion
Cot/bedside
Putting it into practice
There are many innovations which can be applied on ward rounds to increase the opportunities for learning. The challenge is to refine and adapt them as a teaching tool on your ward rounds, and then to use them regularly. This section gives some practical skills and methods to invigorate the ward round learning in your own workplace.
The ‘upside down’ ward round
This concept relies on the fact that the senior member usually takes the lead and in doing so, is the focus of the encounter, whether at the bedside, at the trolley or in the grand round situation. If the team is metaphorically stood on its head, so that one of the more junior members of the team ‘leads’ on that aspect of the round, there is an opportunity for a wide variety of learning. The junior doctor can practice their consultation, clinical assessment and decision-making skills while the senior doctor can model other important areas, for example, writing in the notes, checking drug charts and ensuring documentation is complete.
The ‘merry-go-round’ round
A variation on the upside down round is to assign and rotate (between each patient) roles on the round between the various learners present. These roles may include, for example, the chart reviewer, scribe, clinical examiner, questioner and ward round lead. A version of this round has been described for a sit-down meeting including offering feedback to presenters (the ‘good cop’, informing what was done well and ‘bad cop’ suggesting improvements).25 This type of round can work well in a more routine environment such as special care nurseries and when similar conditions are present between many patients (eg, bronchiolitis), as identified in table 4.
The ‘domino’ round
This is effectively a simultaneous round undertaken by two small teams (maybe each consisting of a registrar or a consultant and a specialty doctor (ST1-3) each with a nurse. Two patients are reviewed at the trolley/board and discussed, and then the teams go off and see each patient one at the same time, coming back to the trolley/board to review the clinical findings and report on the discussion and planning. Applying a more educational emphasis to this round could involve sending pairs of learners off for a short time to research a case or a condition and then to return to the main round and teach the team the topic or information they have researched. This is a variation on Sackett's Educational Prescription.26 27 Running the round in this way blends advantages of the trolley/board round and the cot/bedside (tables 2 and 4).
The ‘flying solo’ round
There is a tension between service and training as described above. Directives for service delivery put pressure on consultants to lead the daily ward round within an acute service. However, there are situations where the round can be left to an experienced trainee who can then report back to the consultant who may then do a board or a trolley round. This method cannot be used daily if the consultant is leading the care as most units require that a consultant sees the admissions. However, it can be useful way of empowering registrars who are ready to ‘act up’ and to give them some supportive autonomy in their clinical assessment and decision-making skills.
The ‘stratified learning’ round
This teaching technique works best if there are different learners on the round, including medical students and nurses/nursing students. As a new clinical topic emerges, if time is available for more detailed discussions, it can be taught in a stratified way. For example, when seeing a baby with jaundice, the medical students might be asked to describe the biochemical and pathophysiological issues behind the baby's clinical condition. The junior doctors could then be asked to discuss the clinical assessment aspects of the case, and the registrars or consultants might be asked to describe how they would counsel parents of a baby with a raised bilirubin level requiring exchange transfusion. They may also want to bring up reference to local or national (eg, National Institute for Health and Clinical Excellence) guidance. The nurses on the round might give their perspective on the nursing aspects of looking after a baby with jaundice, including how to set up phototherapy. This is a good way of involving different members of the multidisciplinary team. Although likely to take place at the trolley/board (table 2), it can be applied to the other ward round setting addressing some of the strengths cited in the ‘teaching’ domain in tables 3 and 4.
The ‘observational’ ward round
With the need for WPBA requirements, watching how juniors perform in real-time during routine work can be a useful way to assess their competency and ensure that they are meeting the requirements of training. Very few trainees seem to manage to do WPBAs evenly across the whole training year. While observing a round led by one of the trainees, it can be difficult for the trainee not to defer to a more senior clinician so the situation may need to be set up before hand, although there are occasions when WPBAs work best spontaneously. Such observation is appropriate on all of the rounds listed in table 1.
All of these can be methods that can be refined to be appropriate for different settings, for example, the community clinic.
Conclusions
Key steps to improving learning on ward rounds
For those beginning to consider their practice and who are unclear where to start, box 1 contains the key elements.
Box 1 Key steps to maximise learning on your ward rounds
Departments need to have a consistent approach that teaching and learning on ward rounds is important and valued.
Trainees come with a variety of experiences that could help or hinder local practice – capturing experiences from elsewhere can be a valuable source of new ideas.
There are endless learning opportunities within ward rounds but using these takes commitment from all participants and careful planning.
Don't be afraid to experiment with different techniques to innovate your ward rounds. Not all your changes will work first time, take feedback, reflect and try again.
We hope that there will be some useful ideas within this review to enable a suitable engaged trainee or a trainer to try their hand at some of the suggestions. The health service moves on in terms of provision and our educational training methods have to keep up. Routine rounds are part of providing good care for children within the services we work in. Without innovations to switch on learning in this clinical environment, we risk stifling the paediatricians of the future into being purely service focused, and they will miss the bigger training picture.
Acknowledgments
The authors would like to thank Simon Frazer for his original work preparing and running this session at PEP as well as the PEP participants and facilitators for their contributions.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.