Article Text

Abstract
Aims: To measure pimecrolimus blood concentrations and to evaluate tolerability and efficacy in children and infants treated topically for atopic dermatitis with pimecrolimus cream 1% for three weeks.
Methods: Three open label, non-controlled, multiple topical dose studies were conducted in children aged 8–14 years (study A, ten patients), and in infants aged 8–30 months (study B, eight patients) and 4–11 months (study C, eight patients). Pimecrolimus blood concentrations were determined on days 4 and 22 of treatment, and at end of study. Efficacy was assessed using the Eczema Area and Severity Index (EASI).
Results: Pimecrolimus blood concentrations were consistently low, typically (81%) below 1 ng/ml, with more than half of the measurements below the assay limit of quantitation (0.5 ng/ml) in studies A and B. The highest blood concentration measured throughout the three studies was 2.6 ng/ml. The cream was well tolerated, locally and systemically. The most common adverse event suspected to be related to study medication was a transient mild to moderate stinging sensation at the application site in 5/26 patients. There was no indication of any systemic adverse effect. The patients responded well to therapy with a rapid onset of action, usually within four days. Median reductions of EASI from baseline at day 22 were 55% (study A), 63% (study B), and 83% (study C).
Conclusion: Three weeks treatment of children and infants with extensive atopic dermatitis, using pimecrolimus cream 1% twice daily, is well tolerated and results in minimal systemic exposure, at which no systemic effect is expected.
- pimecrolimus
- SDZ ASM 981
- elidel
- atopic dermatitis
- blood concentrations
- AUC, area under the blood concentration–time curve
- BSA, body surface area
- EASI, Eczema Area and Severity Index
- LoQ, limit of quantitation
Statistics from Altmetric.com
- AUC, area under the blood concentration–time curve
- BSA, body surface area
- EASI, Eczema Area and Severity Index
- LoQ, limit of quantitation
Atopic dermatitis is an itching inflammatory skin disease which primarily affects children and constitutes a significant burden to the patients and their families. It currently affects 10–15% of children in many parts of the world and its prevalence is rapidly increasing.1 Topical corticosteroids are the most commonly used treatment. Their long term use is, however, limited by local and potentially systemic side effects. Effective and safe alternative therapies are therefore highly desirable. The novel ascomycin macrolactam derivative pimecrolimus has the potential to fulfil this role.
Pimecrolimus was specifically developed for the treatment of inflammatory skin diseases.2,3 It is an inhibitor of the enzyme calcineurin and selectively reduces the synthesis of inflammatory cytokines in T cells and mast cells, and blocks the release of proinflammatory mediators from mast cells after stimulation by antigen/immunoglobulin E.4 In animal models it shows high and skin specific anti-inflammatory activity.5 The clinical efficacy of pimecrolimus has been confirmed after topical application in patients with atopic dermatitis,6–8 as well as in patients with established allergic contact dermatitis9 and chronic irritant hand dermatitis.10 Excellent efficacy was also observed after oral administration in a pilot study in patients with chronic plaque psoriasis.11
Here, we report on studies designed primarily to evaluate blood concentrations, safety, and tolerability of pimecrolimus after repeated topical application of the 1% cream formulation in children and infants with moderate to severe atopic dermatitis. Pimecrolimus was shown previously to be well tolerated and safe after repeated topical application in adults with atopic dermatitis12,13 and to have, in contrast to corticosteroids, no potential to induce skin atrophy.5,14 First experiences in a limited number of children aged 1–4 years with atopic dermatitis indicated that treatment with pimecrolimus cream 1% is also well tolerated in paediatric patients and results in low blood concentrations at which no systemic effect is expected.15 Indeed, during four weeks oral treatment of psoriasis patients, associated with blood concentrations 20 times greater than the highest concentration observed after topical administration, the systemic tolerability was good.11 Before enrolment of children and infants in large clinical trials, it was essential to evaluate further the systemic absorption of the drug and its tolerance in this paediatric population in a well controlled setting.
The primary objective of the studies was to measure pimecrolimus blood concentrations and to evaluate its tolerability when administered as the 1% cream formulation, twice daily for three weeks, to the affected skin in children and infants with atopic dermatitis. The secondary objective was to investigate the efficacy of pimecrolimus cream 1% in those patients.
Three open label, non-controlled, multiple topical dose studies (A–C) were conducted, each consisting of a 1 day to 2 week screening period, a treatment period of 22 days, and an end of study evaluation one week after the last application of pimecrolimus cream 1%.
METHODS
Paediatric patients, aged 4 months to 14 years, were recruited in the Dermatology Department at the Queen’s Medical Centre in Nottingham. They fulfilled the Hanifin and Rajka16 (studies A and B) or the Sampson17 (study C) diagnostic criteria for atopic dermatitis and had at least 10% of their total body surface area (BSA) affected by atopic dermatitis at the screening examination. The patients were treated as outpatients with the pimecrolimus cream 1%, applied twice daily for three weeks (from day 1 to day 22). The cream was applied to all affected skin areas, including the face and neck. The first application on day 1 was performed in the hospital as well as the morning applications on visit days 4 and 22 for the pharmacokinetic evaluations. The amount of cream applied was determined by weighing the tubes of cream at each visit.
The use of oral or topical corticosteroids and emollients containing active ingredients such as urea, was not allowed during the study treatment period. Topical corticosteroids could be used up to the day before the first application of the study drug. The use of bland emollients was encouraged but they had to be applied at least one hour after the study cream. Concomitant prescription of antihistamines and antibiotics was permitted if considered clinically essential.
Blood samples for pharmacokinetics were collected on day 4 and day 22 (last day) of treatment, before (0 h) and 2, 4, and 6 h (study A) or 2 h (studies B, C) after the morning application, and at end of study (one week after the last application, studies A, B), one sample at any time during the visit. Samples were drawn from skin areas not treated with the cream, in order to avoid contamination by the drug. The pimecrolimus blood concentrations were determined using a radioimmunoassay with a limit of quantitation (LoQ) of 0.5 ng/ml (studies A, B),15 or by liquid chromatography/tandem mass spectrometry with an LoQ of 0.1 ng/ml (study C). Briefly, after addition of a suitable internal standard solution and buffer (pH 10, 0.5 ml), whole blood (0.5 ml) was extracted with t-butylmethylether (0.5 ml). The organic phase was recovered, dried, and reconstituted for chromatography. High performance liquid chromatography was performed using a Nucleosil 100 C18 (750×4 mm) column at 75°C with gradient elution (solvent A: methanol; solvent B: 80% methanol in 20 mM aqueous ammonium acetate); gradient: from 0 to 8 min 100% B, from 8 to 12 min 100% A, from 12 to 14 min 100% B; flow rate: 1.0 ml/min. An atmospheric pressure chemical ionisation interface was used with mass spectrometry in negative ion mode with a mass resolution of 0.7 amu and a scan time of 1.5 s.
In study A, the maximum blood concentration (Cmax) was derived from the individual blood concentration profiles. When a profile included at least three quantifiable concentrations, the area under the blood concentration–time curve over a dosing interval (AUC(0–12 h)) was calculated by linear trapezoidal summation from 0 to 12 h. The concentration at 12 h was assumed to be equal to that measured before application (0 h) from the same profile. Values below the LoQ were treated as zero for the calculation of AUC. Because of the high proportion of non-quantifiable blood concentrations (measured below the assay LoQ), only a few pharmacokinetic parameters could be calculated in some individuals of study A. Therefore, no formal statistics were performed on the pharmacokinetic parameters.
Because of the broad paediatric age range covered by these studies (4 months to 14 years), a statistical analysis was performed to investigate influence of decreasing age on systemic exposure to pimecrolimus. A linear regression of concentrations against age was performed using the SAS system, version 6.12 under Windows NT. For that purpose, blood concentrations of all individuals were pooled together because it was known from a previous topical study in adult atopic dermatitis patients,12 that full blood concentration profiles displayed a plateau with no clearly identifiable peak. Blood concentrations below the LoQ were set to half the LoQ in an attempt to linearise the relation between concentration and age. The same approach was used to investigate the relation between pimecrolimus blood concentrations and the percentage of total BSA affected at baseline.
Safety and tolerability were evaluated by physical examination, vital signs (pulse rate, systolic and diastolic blood pressure, body temperature, and body weight), safety laboratory evaluations (biochemistry, haematology, urinalysis), and recording of adverse events throughout the study. Laboratory parameters, which included full blood count, urea and electrolytes, serum creatinine, liver function tests, calcium, glucose, creatinine phosphokinase, and magnesium, were measured at screening, and on day 4 and day 22 of treatment.
Efficacy was determined at each visit on days 1, 4, 10, and 22, and one week after the end of treatment by scoring the extent of lesions and by evaluating the clinical signs and symptoms of the disease (erythema, induration, excoriation, and lichenification), using the Eczema Area and Severity Index (EASI).18 An exploratory analysis of the pooled EASI scores was performed using the SAS system, version 6.12 under Windows NT. The change in EASI on days 4, 10, and 22, respectively, versus baseline (day 1) was analysed using a paired t test.
RESULTS
Patients
A total of 26 patients were enrolled in the three studies; 25 completed the study according to the protocol. These patients presented with 21–80% of their BSA affected at baseline. Table 1 shows the age range and extent of skin area affected. One patient in study A discontinued after 10 days of treatment due to a severe infective exacerbation of her atopic dermatitis. Since this child had experienced a number of similar episodes over a period of many years, this event was not considered to be related to study medication. In all three studies, the individual amount of pimecrolimus cream used per application ranged from 0.7 to 15 g.
Demographics at baseline
Blood concentrations
Blood concentrations were consistently low, typically (81%) below 1 ng/ml with more than half of the measurements below the assay LoQ in studies A and B. In all three studies, the concentrations were in the same low range (<LoQ to 2.6 ng/ml) in children and in infants (table 2). The highest blood concentration observed (2.6 ng/ml) was measured in a patient from study C on day 4, two hours after application of the cream. On day 22, the 2-h post-dose concentration for this patient was 0.94 ng/ml.
Distribution of pimecrolimus blood concentrations in paediatric atopic dermatitis patients treated with pimecrolimus 1% cream for three weeks
Two isolated high blood concentrations were observed in two patients: study B, >50 ng/ml, day 22, two hours post-application, value not quantifiable within the assay calibration curve (maximum calibration concentration being 50 ng/ml); study C, 36.6 ng/ml, day 4, two hours post-application. In these two patients, the other blood concentrations measured were 0.5 ng/ml on day 4 (study B) and 0.55–0.75 ng/ml on additional days (study C). Therefore, the high values were suspected to be a result of sample contamination during venipuncture. The associated sample of study C was further analysed for the major pimecrolimus metabolite concentration. The peak area ratio of metabolite:parent drug was determined and compared to those found in another study following oral administration of pimecrolimus (Floesser A et al., Novartis Pharma AG, unpublished data). The suspected contaminated sample from the topical study showed much lower metabolite:parent drug ratio (<0.008) than that found in the oral study (range 0.03–0.09). This analysis further supported the suspicion that the high concentrations of pimecrolimus were due to external contamination of the blood samples by the cream during venipuncture.
In the three studies, blood concentrations of pimecrolimus on day 22 were in the same range as those measured on day 4, indicating that there was no drug accumulation during the three weeks of treatment (fig 1).
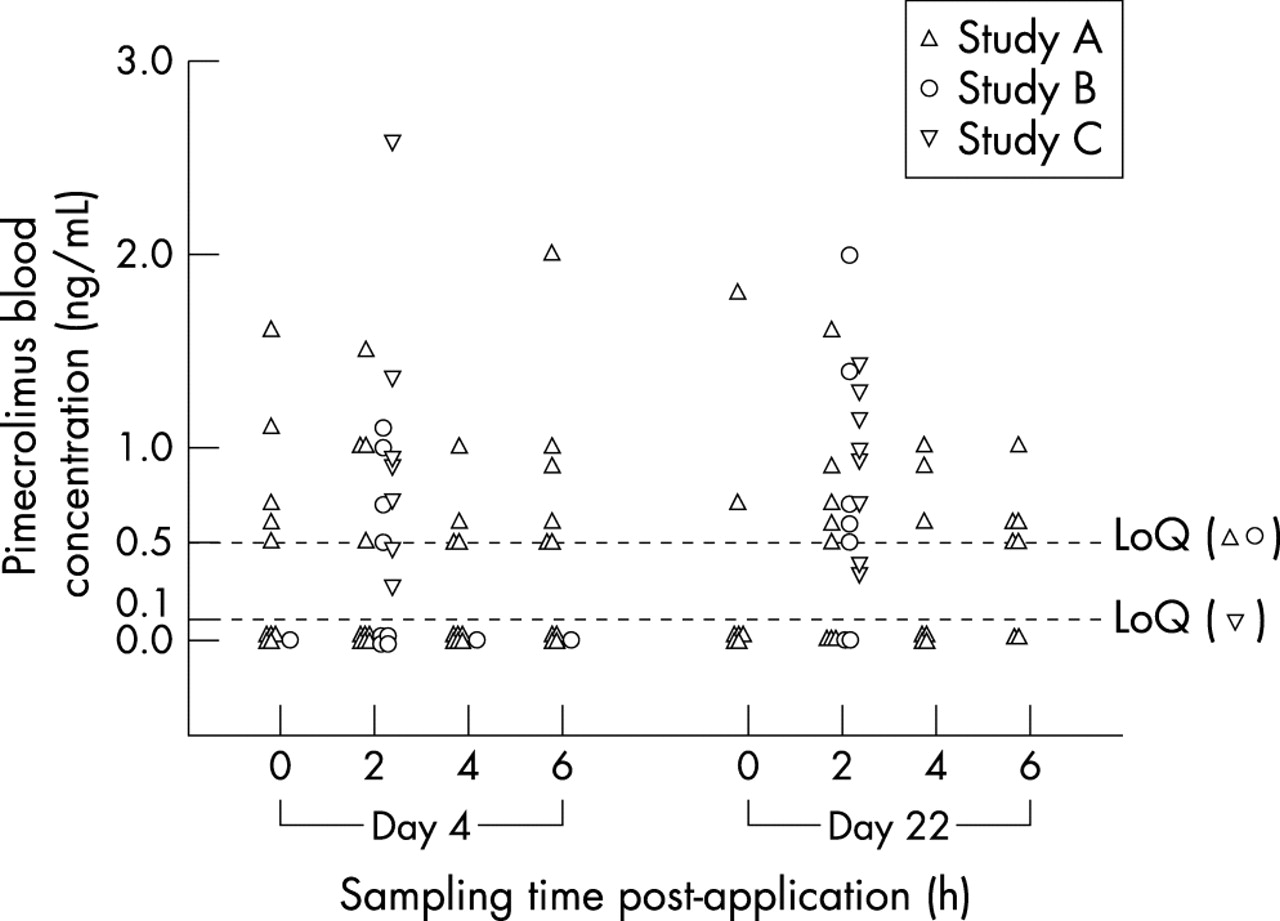
Pimecrolimus blood concentrations in children and infants on day 4 and day 22 of a three week treatment course.
Figure 2 shows blood concentrations of pimecrolimus versus percentage BSA affected at baseline. A linear regression analysis revealed a very small but statistically significant increase of concentration with increasing body surface area affected (p = 0.028). The difference in mean concentration between a patient with 90% affected BSA at baseline and a patient with 10% BSA was estimated to be 0.7 ng/ml.
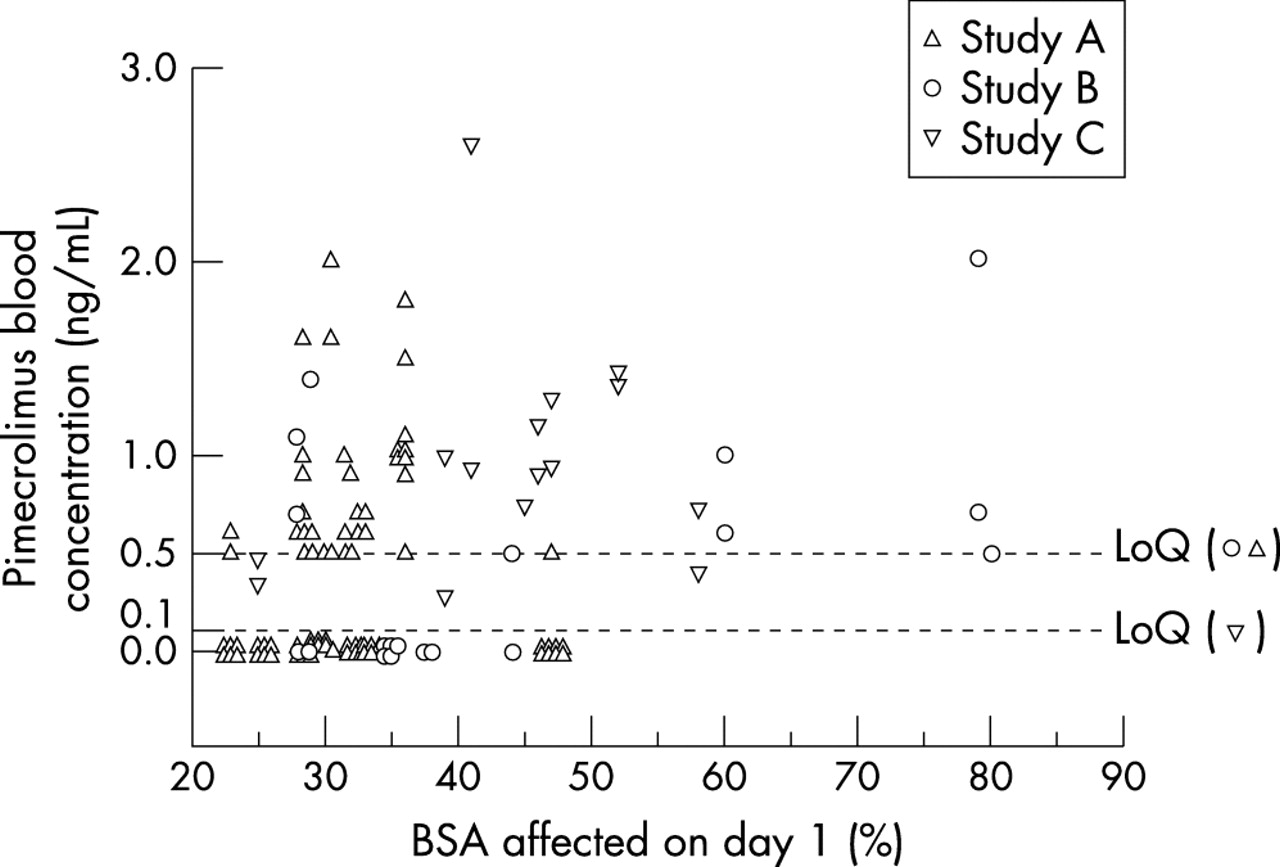
Blood concentrations of pimecrolimus versus body surface area at baseline (day 1).
Blood levels were in a comparable range within the broad paediatric age range studied (3 months to 14 years). The linear regression of concentrations against age indicated a slight decrease of concentrations with increasing age, which was, however, not statistically significant (p = 0.11).
As many blood concentrations were below the LoQ, determination of AUC[0–12 h] was only possible in four patients of study A on day 4, and three patients of study A on day 22. AUC[0–12 h] ranged from 5.4 to 16.4 ng.h/ml.
Safety and tolerability
No study medication related serious adverse event occurred in any of the three studies. Overall, 11 of 26 patients who participated in the three studies did not experience any adverse event at all during the three week treatment course. One patient in study A developed a severe infective exacerbation of her atopic dermatitis requiring hospitalisation. She was treated with intravenous antibiotics and recovered rapidly. The investigator did not consider this event to be related to the study medication since this patient had had a number of similar exacerbations during the previous 10 years.
The most frequent adverse event, observed in five patients, was an initial discomfort at the site of application, described as transient stinging and rated as mild to moderate (table 3). Dry skin was reported in two patients and moderate pruritus in one patient. The infective exacerbation of eczema on the buttock observed in one patient (study B) was considered by the investigator to be most likely due to an interaction between cream and nappy area. Other adverse events were mostly mild in nature and not suspected to be drug related (table 3).
Summary of adverse events
There were no relevant and clinically significant deviations from normal in blood biochemistry, haematology, urinalysis, and in vital signs.
Efficacy
A marked decrease in EASI as early as day 4 was observed with pimecrolimus cream 1% in the three studies (fig 3), indicating therapeutic effect. On day 22, after three weeks of treatment with pimecrolimus cream 1%, the median reduction of EASI from baseline for the patients who completed the study was 55% in study A, 63% in study B, and 83% in study C (table 4). The analysis of the pooled data of EASI change from baseline showed a statistically significant reduction on days 4, 10, and 22 (p<0.0001 for all three timepoints).
Eczema Area and Severity Index (EASI)

{kind=link}
{kind=link}
{kind=link}
Median reduction (%) of EASI from baseline (day 1) during three weeks of treatment of paediatric atopic dermatitis patients with pimecrolimus 1% cream.
DISCUSSION
The development of a new drug for the long term treatment of chronic atopic dermatitis in the paediatric patient population requires a careful evaluation of all safety aspects. One of the primary objectives of the present studies was to measure pimecrolimus blood concentrations, and to confirm the minimal systemic absorption in infants and children, as observed previously in adults and in a different child age group with atopic dermatitis.12,13,15 With respect to their primary objective and because pharmacokinetic studies are difficult to conduct in young children, the studies were conducted open and non-controlled in order to facilitate the recruitment of paediatric patients. Since the ratio of skin surface treated versus body weight increases with decreasing age, it was of particular interest to study whether there would be differences in blood concentrations between children (>2–14 years) and infants (<2 years), and to compare this with data from pharmacokinetic studies in adults treated with pimecrolimus cream 1%.
Based on the extensive blood concentration profile data collected in adult patients,12 day 4 was chosen as the timepoint for blood sampling at which maximum exposure was most likely to occur, but before the lesions had fully improved. Samples on day 22 were drawn in order to verify that the drug did not accumulate during the three weeks of treatment.
The blood concentrations of pimecrolimus measured in these paediatric patients, 2–6 hours after morning cream application, were consistently low, typically (81%) lower than 1 ng/ml (table 2). In all three studies, excluding two high values thought to be associated with contaminated samples, the highest concentration was 2.6 ng/ml, measured in one patient on day 4 of treatment, two hours after morning cream application. This patient was 8 months old and had 41% BSA affected at baseline. At the end of the three week treatment (day 22), the concentration measured in this patient was 0.94 ng/ml. Within the broad paediatric age range studied (3 months to 14 years), blood levels were in the same range (no statistically significant difference) as those observed previously in adults (<LoQ to 1.4 ng/ml)12 and in children aged 1–4 years (<LoQ to 1.8 ng/ml),15 treated under the same dosing regimen for three weeks. Absorption of pimecrolimus through skin thus appears to be similar in infants, children, and adults. As observed in previous studies, there was no evidence for accumulation of pimecrolimus in blood from day 4 to day 22. Although there was a small, but statistically significant, increase of pimecrolimus blood concentrations with %BSA affected at baseline, blood concentrations remained low (<LoQ to 2.6 ng/ml), even in patients with the highest %BSA (up to 80%). This supports use of the cream, with no limitation of the area of skin under treatment.
In all three studies, the twice daily application of pimecrolimus cream 1% for three weeks was well tolerated. Consistent with the very low systemic exposure observed in the paediatric patients, no systemic adverse effects were noted. The most common drug related adverse event was a mild to moderate stinging sensation at the site of cream application, in five patients. However, these events were reported as being transient and did not lead to discontinuation from study treatment. In addition, one incident of pruritus, two cases of dry skin, and one event of infected exacerbation of eczema on the buttock (suspected of being associated with nappy usage) occurred. All other adverse events were those seen typically in a young paediatric population and not considered to be drug related.
It is noteworthy that no manifestations of toxicity have been observed with pimecrolimus in man to date, either after topical or after oral administration. The maximum blood concentration (2.6 ng/ml) and AUC(0–12 h) (16.4 ng.h/ml) observed in the present studies are about 20 times lower than those observed in adult psoriasis patients at steady state following repeated oral administrations of a well tolerated 30 mg twice daily dose of pimecrolimus for four weeks (mean Cmax 54.5 ng/ml; mean AUC(0–12 h) 294.9 ng.h/ml).11 Up to and at this highest oral dose tested, no significant adverse events were reported in these patients. During the four week treatment course no significant changes in physical examination, vital signs, ECG, and laboratory parameters, including kidney function tests were noted.
In summary, these data were collected during a small pharmacokinetic study, the aim of which was to investigate blood concentrations before embarking on large paediatric clinical trials. They showed that the short term use of pimecrolimus cream 1% in children and infants with atopic dermatitis results in minimal systemic exposure and is well tolerated. Data from large, double blind, vehicle controlled, randomised clinical studies confirmed that pimecrolimus is safe when used in the paediatric population.19–22 Systemic exposure to and tolerability of pimecrolimus cream 1% in long term treatment (up to 1 year) is being further evaluated in children and infants with atopic dermatitis.
The efficacy of the treatment was assessed by using EASI for scoring of the lesions.18 Despite the fact that interpretation of efficacy in these studies is limited by the open, non-controlled study design and the small number of patients, a substantial improvement in the atopic dermatitis was noted for all patients, together with a rapid onset of action, usually within four days. The response was generally shown to be sustained throughout the entire treatment period. This suggests that pimecrolimus cream 1% is likely to be an effective treatment for atopic dermatitis in children and infants. Results from subsequent double blind, multicentre, vehicle controlled, randomised studies with pimecrolimus cream 1% in infants and children support these findings.19–22
Conclusion
In open label, non-controlled pharmacokinetic studies, topical treatment of children and infants with extensive atopic dermatitis lesions with pimecrolimus cream 1% for three weeks, twice daily, resulted in consistently low pimecrolimus blood concentrations, with no accumulation over time regardless of the extent of skin areas treated; the treatment was well tolerated and effective. Data from large double blind, vehicle controlled, randomised clinical studies confirmed that pimecrolimus is safe and effective when used in the paediatric population. These results therefore support the use of pimecrolimus cream 1% for long term management of atopic dermatitis in infants and children.