Article Text

Abstract
Background Paracetamol is the most commonly prescribed medicine for children. Age-based dosing guidelines can lead to inappropriate dosing.
Methods A review of age-based guidelines for paracetamol in the British National Formulary for Children (BNFC) 2011–2012 was undertaken. Single and cumulative daily doses of paracetamol for boys and girls at 9th, 50th and 91st centiles for weight were calculated for the age groups 1–3 months, 3–12 months, 1–6 years and 6–12 years.
Results For children at the 9th centile, aged 3 months and above, doses were above recommended single and cumulative daily dose therapeutic limits when given the highest dose specified for their age. For children at the 91st centile at all ages, doses were below recommended single and cumulative daily dose therapeutic limits when given the lowest dose specified for their age.
Conclusions Underweight and overweight children are at risk of inappropriate paracetamol administration based on BNFC age-based dosing instructions.
Statistics from Altmetric.com
Introduction
Paracetamol is the most commonly prescribed medicine for children, however it is often misprescribed.1 Age-based dosing guidelines for children have been found to be imprecise2 and result in inaccurate dosing due to marked variations in weight of children of the same age. To reduce the inherent risk, most paediatric texts and guidelines suggest prescribing paracetamol based on weight instead of age. However, the British National Formulary for Children (BNFC),3 the authoritative guide for prescribing medications to children in the UK, recommends age-based dosing for certain indications and age groups.
To address this issue, the authors compared the BNFC age-based dosing guidelines for single and cumulative daily doses of paracetamol for children at different weight centiles, with internationally recommended weight-based therapeutic dose ranges.
Methods
Paracetamol age-based dosing guidelines in the BNFC 2011–2012 were reviewed for children aged 1 month to 12 years. Paediatric growth charts were used to estimate the average weight of boys and girls respectively in the 9th, 50th and 91st weight centiles at the ages of 1 month, 3 months, 12 months, 6 years and 12 years. UK-WHO growth charts were used for children aged 0–4 years and UK90 charts for children older than 4 years.
Calculations were then performed to determine the range of potential doses (mg/kg) when following the BNFC guidelines. The upper doses were calculated by dividing the highest dose of paracetamol specified in the BNFC at each age, by the weight of a child in the 9th centile for weight. Average doses were calculated by dividing the average (middle) dose of paracetamol specified in the BNFC at each age, by the weight of a child in the 50th centile for weight. The lower doses were calculated by dividing the lowest dose of paracetamol specified in the BNFC at each age, by the weight of a child in the 91st centile for weight. As the BNFC uses the eldest age of the preceding age bracket as the starting age of the following age bracket, the upper dose derived in our calculations was the maximum dose advised in the higher age bracket, and the lower dose derived in our calculations was the minimum dose advised in the lower age bracket.
Assuming that a child was to be given ongoing doses of paracetamol over a 24 h period, the cumulative daily dose was also calculated. For children aged 1 month, a maximum of 8 hourly dosing is recommended by the BNFC, therefore the daily dose was calculated by multiplying the single dose by three. For children aged 3 months and older, a maximum of four doses in 24 h is recommended, and so the cumulative daily dose was calculated by multiplying the single dose by four. For children aged 12 years, no maximum daily limit is recommended in the highest age bracket, and therefore the cumulative daily dose was calculated based on the maximum frequency of dosing recommended (4 hourly dosing), therefore multiplying the single dose by six.
For a single dose, 10–15 mg/kg was used as the recommended therapeutic dose range, based on standard textbook recommendations.4 A recommended maximum daily therapeutic limit of 60 mg/kg/24 h was selected based on a summary of WHO policy regarding paracetamol.5
Results
The BNFC dosing guidelines are based on either age or weight according to route of administration, indication and age of the child.3 For the oral route of administration, guidelines are age-based for the indications of ‘pain; fever with discomfort’ and ‘post-immunisation fever in infants’ and weight-based for the indication of ‘severe postoperative pain’ up to the age of 12. The age-based guidelines for children aged 1 month to 12 years, for the indication of ‘pain; fever with discomfort’, are reviewed below.
For boys at the 9th centile for weight in all age groups and girls at the 9th centile for weight at age 3 months and above, the upper single dose of paracetamol exceeded the recommended therapeutic range (10–15 mg/kg) with doses between 16 and 33 mg/kg (figure 1A,B). For boys and girls at the 50th centile for weight at all age groups the average single dose was between 9 and 13 mg/kg (figure 1A,B). For boys and girls at the 91st centile for weight in all age groups, the lower dose limit of a single dose of paracetamol was approximately one-third to one-half of the recommended therapeutic range, with doses of between 4 and 6 mg/kg (figure 1A,B).

Calculated paracetamol doses (mg/kg) based on British National Formulary for Children age-based guidelines for low (9th centile), average (50th centile) and high (91st centile) weights for boys (A) and girls (B), 1 month to 12 years, compared with recommended dose range.
 Lowest dose in age range/91st centile weight;
Lowest dose in age range/91st centile weight;  average dose in age range/50th centile weight;
average dose in age range/50th centile weight;
 highest dose in age range/9th centile weight;
highest dose in age range/9th centile weight;  hashed area represents recommended dose range.
hashed area represents recommended dose range.
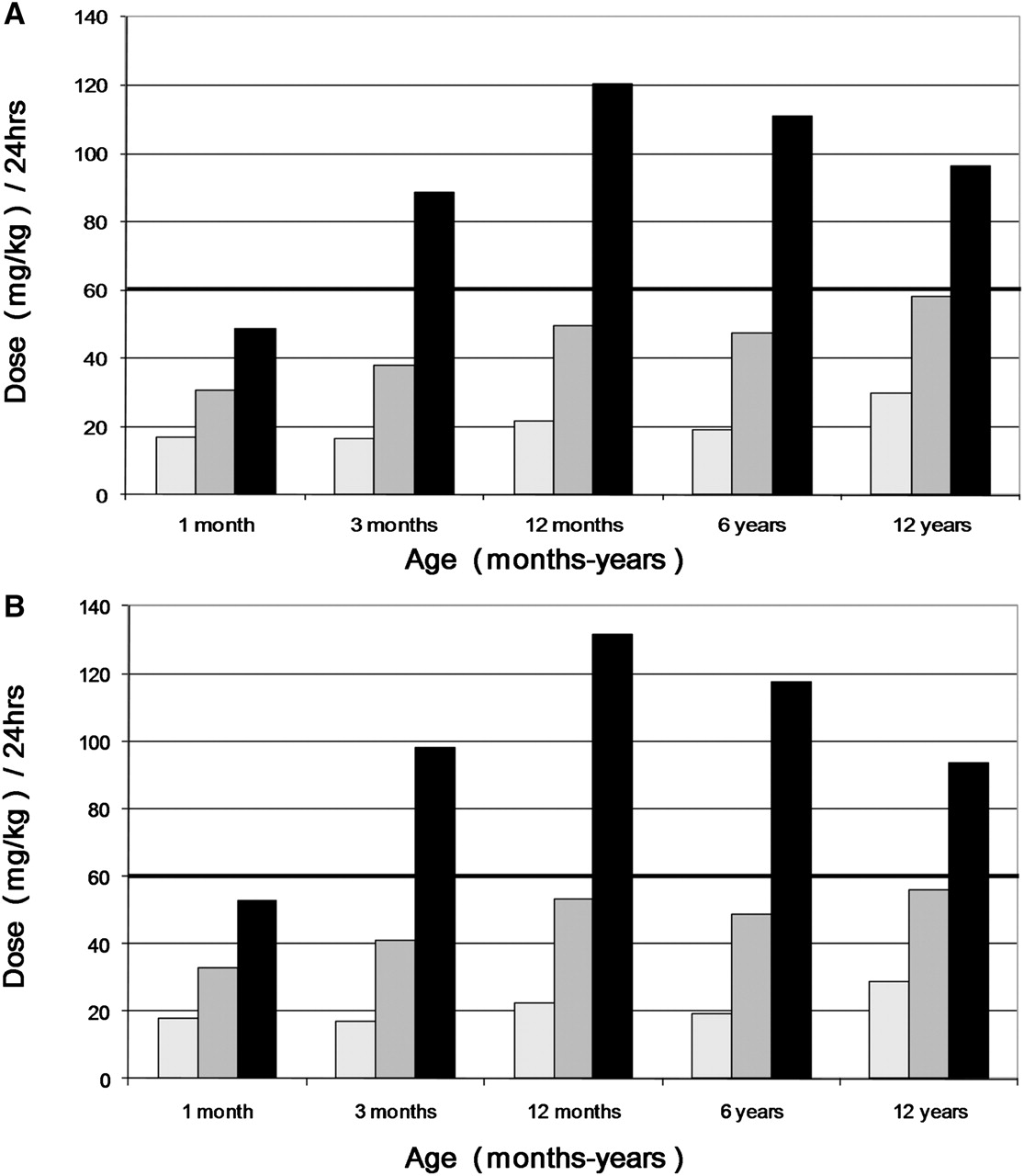
For children aged 3 months and above, all boys and girls at the 9th centile for weight had an upper cumulative daily dose well above the recommended maximum daily therapeutic limit of 60 mg/kg/24 h, with doses of between 89 and 132 mg/kg/24 h (figure 2A,B). Children at the 50th and 91st centile for weight in all age groups had cumulative daily doses below the recommended maximum daily therapeutic limit (figure 2A,B).
{kind=link}
{kind=link}
Calculated cumulative daily paracetamol doses (mg/kg/24 h) based on British National Formulary for Children age-based guidelines for low (9th centile), average (50th centile) and high (91st centile) weights for boys (A) and girls (B), 1 month to 12 years, compared with recommended maximum cumulative daily limit.
 (Lowest dose in age range/91st centile weight) × maximum number of doses daily
(Lowest dose in age range/91st centile weight) × maximum number of doses daily
 (average dose in age range/50th centile weight) × maximum number of doses daily
(average dose in age range/50th centile weight) × maximum number of doses daily
 (highest dose in age range/9th centile weight) × maximum number of doses daily.
(highest dose in age range/9th centile weight) × maximum number of doses daily.
Bold line denotes maximum cumulative daily limit.
Discussion
The age-based prescribing guidelines for paracetamol in the BNFC 2011–2012 do not take into account the large variation in body weight within each age category, leading to a substantial risk of inappropriate dosing. Our calculations demonstrated a risk of excessive dosing in underweight children, when the highest dose corresponding to their age group was used. Administration of such doses has the potential to cause harm, as supratherapeutic doses of paracetamol can cause hepatotoxicity, particularly in unwell children with high fever.6 However, overweight children would be prescribed on average only one-third to one-half of the recommended therapeutic dose, when the lowest dose corresponding to their age group was used. Such doses of around 5 mg/kg are ineffective,7 resulting in inadequate relief of pain and fever.
Some uncertainty exists regarding the safe maximum cumulative daily limit of paracetamol for children. However, our accompanying figures show that even if a higher cumulative daily dose limit were to be applied, many underweight children would still receive excessive doses that have the possibility to cause harm. Further, our calculations showed that there is an approximately threefold to fivefold difference in prescribed doses between underweight children given high doses of paracetamol, and overweight children given low doses.
As our calculations were taken from the 9th and 91st centiles for weight, the dosing variations described would become even more pronounced for children in the upper and lower 9% for body weight. While our calculations represent the outer bounds of dosing (low weight/high dose, high weight/low dose), paracetamol is often prescribed in a hospital setting by junior doctors who may lack the ability to recognise a child who is underweight or overweight for their age and, therefore, may prescribe paracetamol without consideration of the child's weight. Further, the numerous dosing instructions for various indications for and routes of administration of paracetamol in the BNFC are potentially another source of inappropriate dosing.
Conclusion
The age-based prescribing guidelines for paracetamol in the BNFC 2011–2012 do not account for the variations in body weight of children within each age category, leading to a potential risk of overdosing in underweight children and underdosing in overweight children. We recommend that the BNFC move to weight-based dosing guidelines for paracetamol when indicated for pain or fever with discomfort in children.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Contributors SE developed the concept for the study. SE, AE, KP and RB were involved with study design and data analysis. SE, AE, KP and RB were involved with the drafting of the manuscript. SE, JF, KP and RB were involved with manuscript revision. JF was involved with figure design and data-checking. SE is the guarantor.