Article Text

Abstract
Anorexia nervosa (AN) is a common condition affecting young people. The medical management of AN on a general paediatric ward is challenging. It is important to identify young people who are at risk of medical complications, so early intervention can be instigated. This article aims to review the clinical practice and evidence supporting the current medical management of young people with AN. It provides a system-based approach to potential complications of the disease, guidance on feeding and the management of re-feeding syndrome. Approaches to legal and ethical challenges are also considered. While the importance of psychiatric treatment is recognised, the same is not discussed within this article.
Statistics from Altmetric.com
Introduction
Anorexia nervosa (AN) is a condition characterised by sustained deliberate weight loss or failure to gain expected weight with varying degrees of undernutrition and secondary endocrine or metabolic change.1 2 It is most common in adolescent girls occurring in up to 0.7% of this group.3 It may also affect males, younger children and adults.1 It is associated with significant morbidity and mortality. Most patients recover completely, however, 5% die as a consequence of AN and 20% progress to chronic eating disorders. Common causes of death are suicide and medical complications of the disease.3 Young people may not fit the full International Classification of Diseases 10 diagnostic criteria, however, medical risks remain similar, therefore management should be as for AN.
Initial assessment
The initial medical assessment should identify the extent of any physiological compromise and determine an approach to management. It should include a full history and examination, paying attention to associated signs and symptoms (table 1).
Signs and symptoms of anorexia nervosa
Height and weight history and degree of weight loss should be reviewed. Accurate admission measurements must be recorded and plotted onto standard World Health Organization growth charts.2 Bone age, mid-parental height ranges and stage of puberty may be helpful. Details of binges or purging, exercise and drug use, and current attitudes to food should be assessed. A detailed dietary history, including fluid intake, should be taken. Patient or family history of obesity, psychiatric disorders (particularly eating disorders) or substance misuse is important. Other conditions which may produce similar symptoms such as neoplastic, inflammatory or endocrine causes, should be excluded with appropriate investigations.2 4
Clinical examination should pay particular attention to the cardiovascular system, general body stability (eg, temperature, muscle strength), skin and signs of purging and self-harm. Vital signs should be measured and baseline investigations tailored to the young person's specific presentation.2 4 A suggested scoring system to aid identification of those particularly at risk is given in table 2. While such tables provide a useful framework for evaluation, care needs to be exercised when interpreting them in paediatrics due to variability of normative data in this population. In particular, use of age-appropriate blood pressure centile charts and local laboratory reference ranges is important.5
Scoring sheet for medical assessment (reproduced with permission from Professor Janet Treasure)
Admission to a paediatric medical ward should be reserved for patients with complications of extreme malnutrition, those deemed at risk of re-feeding syndrome (RFS), those in whom outpatient treatment is failing or younger children who do not meet the age criteria for specialist adolescent eating disorder units.
Most patients can be cared for on a general paediatric ward or adolescent unit. In extreme cases, critical care management may be required.2 4 Medical management should be undertaken alongside psychiatric treatment.
The National Institute for Health and Clinical Excellence recommends the following indications for inpatient hospitalisation in patients of 8 years or older2:
Body mass index (BMI) <13 kg/m2.
>1 kg weight loss over a week.
Below second centile on BMI centile chart.
Blood pressure <80/50.
Pulse <40.
Marked orthostatic hypotension (increase in heart rate of 20 beats per minute and drop in standing blood pressure of 10–20 mmHg).
Cold peripheries or hypothermia <34.5oC.
Unable to get up without using arms as leverage.
Electrolyte abnormalities (K <2.5 mmol, Na <130 mmol, phosphate <0.5 mmol).
Prolonged QTc interval on ECG.
There is debate regarding the use of BMI as a measure of significant undernutrition in younger children. Using a method that takes into account the relationship between weight, height and age may more accurately reflect severity of illness.2 Potential methods suggested include calculating percentage weight for height or percentage median BMI. The Royal College of Paediatrics and Child Health (RCPCH)recommends the use of the UK 90 BMI reference ranges as opposed to weight for height measures in the UK population.6 A local consensus should be identified.
Management
The goals of management are stabilisation of vital signs, electrolyte correction, nutritional rehabilitation and motivation for recovery.7
The medical care plan should address and record how these goals will be achieved. It is important to involve all members of the multidisciplinary team (paediatrician, nursing staff, dietitian, medical specialists, psychiatrist, psychiatric nurse, occupational therapist, physiotherapist, pharmacist, dentist, patient, family)and establish therapeutic alliances with patient and family. A lead clinician should be appointed to ensure continuity of care. The plan should be reviewed regularly and boundaries clearly set.
Medical complications of AN
The profound nutritional deprivation underlying AN can cause a number of significant physiological disturbances (table 1).8 Some of these are a direct consequence of AN and some are complications of its treatment, eg, RFS.
Cardiac
Cardiovascular compromise occurs early in AN in up to 87% of patients. It is the most common cause of death after suicide and is seen in proportion to nutritional deprivation.9 Malnutrition causes cellular changes within the cardiac muscle, leading to structural, functional or electrocardiological complications. Significant cellular changes include reduced protein synthesis, mitochondrial swelling, activation of calcium-dependent proteinases, reduced glycogen, oedema and myofibrillar atrophy.10
Cardiac muscle becomes hypotrophic leading to reduced cardiac output, preload and left ventricular function. Ejection fraction is often preserved.11 Reduction in cardiac muscle mass can cause mitral valve prolapse in 33–62% of patients. This is often asymptomatic, but sudden death is a known complication of this abnormality.12 13
Cardiac rhythm disturbances are common. The majority of patients develop a sinus bradycardia as an adaptation to the hypometabolic state. A tachycardia is therefore concerning. There is marked heart rate variability, possibly due to autonomic change. QT prolongation, seen in up to 15% of patients, has been associated with ventricular arrhythmias and death. Other ECG changes are common and include prolonged PR interval, first-degree heart block, prolonged QTc, ST segment changes, left shift of the QRS axis and diminished QRS amplitude. These are often related to underlying structural or electrolyte abnormalities and should be investigated at the time of presentation. Any reversible cause should be corrected.9 14,–,16 Blood sugar monitoring is important as hypoglycaemia can induce high blood catecholamine levels and potentially cause myocardial damage or arrhythmias.17
Orthostatic changes occur in 60–80% of patients, increasing their risk of syncope.18 Other cardiac complications include hypotension, peripheral oedema, pericardial effusions and congestive cardiac failure.19 In its mild form, peripheral oedema is simply dependent, but in severely malnourished patients, it can progress to hypovolaemia and circulatory collapse.9
Most cardiac complications improve with re-feeding.14 Due to their frequency and potential severity, close monitoring of heart rate, ECG, blood pressure and orthostatic changes is mandatory. Particular care should be taken in patients with prolonged QTc to avoid exacerbating the condition. Exercise should be avoided in severely compromised patients until cardiac function has normalised.16
Renal, fluid and electrolytes
Renal, electrolyte and volume disturbances occur in approximately 70% of patients. In extreme cases, renal failure can occur.9 20 Glomerular filtration rate falls, reducing the concentrating capacity of the kidneys. Blood urea rises but creatinine is low as a consequence of low muscle mass. Electrolyte abnormalities include hypocalcaemia, hyponatraemia, hypokalaemia, hypomagnesaemia and hypophosphataemia. The effects of these abnormalities are shown in table 3. Hypomagnesaemia is associated with hypocalcaemia and hypokalaemia, which may not resolve unless magnesium is concurrently replaced.9
Effects of electrolyte disturbance in anorexia nervosa
There is an increased risk of renal stones and acid–base disturbances, which can adversely affect both enzyme and metabolic systems.4 A persistent hypovolaemic state can also lead to disturbances of the renin–angiotensin–aldosterone pathway and relative hyperaldosteronism. Vasopressin release can be erratic leading to neurogenic diabetes insipidus.8
Gastrointestinal
Restricting food intake and purging can damage the gastrointestinal tract. There is a 16% rate of oesophagitis and commencement of appropriate medication, such as proton pump inhibitors, is advised. Mallory-Weis and Boerhaave's tears can occur after excessive vomiting. Superior mesenteric artery syndrome, pancreatitis, impaired gastric motility, liver enzyme abnormalities, constipation and ileus have all been reported. Large bowel abnormalities may occur, often with a similar clinical presentation to inflammatory bowel disease, particularly with inappropriate use of laxatives.2 9 21
Dental pathology is common with increased risk of caries and acid erosion, particularly in cases of purging. Erythema of the pharynx and enlarged salivary glands (mainly parotid) may be seen. Regular dental reviews are recommended.2 9 18
Respiratory
Respiratory complications are uncommon until late in the disease, when patients may need critical care. Pulmonary function tests often show reduced pulmonary volumes early in the disease, but this is rarely of any clinical significance.4
Neurological
Neurological changes include apathy, poor concentration, muscle weakness, pain, cramps and myopathy. Patients who are immobile for prolonged periods may be at risk of further muscle wasting and nerve compression.
Brain CT and MRI scans have demonstrated enlarged cerebrospinal fluid spaces with volume deficits in grey and white matter suggesting a degree of cerebral atrophy. The magnitude of these changes generally correlates with the degree of malnutrition. Although white matter changes are reversible with nutritional rehabilitation, grey matter volume deficits and blood flow disturbances can persist despite weight restoration.8
Haematological
The most common haematological changes are to white blood cells. Although overall white cell count is usually within the normal range, patients have lower counts than healthy matched controls and may develop neutropaenia and lymphopaenia. This may be associated with a 15-fold increase in relative risk of infection. Granulocyte activity, cell-mediated immunity and complement activity may be reduced. Correlations have been suggested between severity of AN and infection risk.22 23
Anaemia is seen in 9–36% of patients and is generally normocytic. Thrombocytopenia is usually mild with few patients showing signs of purpura on admission. Haematological abnormalities can be associated with concurrent bone marrow changes. Pancytopaenia may occur in severe cases. All these changes are associated with a low BMI and are reversible with weight gain.23
Other complications
Patients can develop significant pressure areas as reduced adipose, poor-quality dry skin, reduced healing capacity and prolonged immobility take effect. Stress fractures may occur.24 Good-quality nursing care is of extreme importance in preventing such complications. Rarely vitamin deficiencies may lead to patients showing signs of pellagra (niacin deficiency) or scurvy (Vitamin C deficiency).9 Other reported effects include impaired temperature homeostasis with a lack of shivering, vasodilatation and vasoconstriction that may reflect a hypothalamic disturbance.9
In the longer term, consideration should be given to the consequences of malnutrition, eg, endocrine disturbance (delayed/arrested puberty and secondary amenorrhoea) and bone health (osteopenia and osteoporosis). There is no evidence to support the use of bisphosphonates and oestrogen therapy should be avoided as it can precipitate premature fusion of epiphyses.25
Nutritional management and its complications
Golden and Meyer identify five goals to nutritional rehabilitation: metabolic recovery (changing from catabolic to anabolic state), weight restoration, reversal of medical complications, improved psychological functioning and improved eating behaviours.15
Re-feeding
Oral feeding is the preferred route for re-feeding. If this does not achieve the desired calorific intake, nasogastric feeding may be appropriate. A continuous infusion may be better tolerated than bolus feeds. Enteral feeding reduces the risk of bacterial translocation, line infections and metabolic disturbance seen with parenteral nutrition, the use of which should be limited to when no alternative is available.2 4 15 26
A multidisciplinary approach towards feeding is essential. Type, mode of administration, supervision and approach to non-compliance should be defined in advance. Consideration should be given to restriction of caffeine, excess fluid and salt, as well as the potential for concealment or disposal of calories. Weight should be regularly measured and patients monitored for signs of purging. Excessive exercise should be discouraged. If there is doubt regarding fluid intake, specific gravity of urine can be measured to ensure patients are not taking excessive fluids.4
The body adapts to low calorie intake by reducing basal metabolic rate. Resting energy expenditure falls and initial calorific requirements are low. These increase dramatically as rehabilitation occurs. There is debate about how fast weight gain should occur. Suggested target weight gain ranges from 0.5 to 1 kg per week. Independent of the type of nutritional rehabilitation, a balanced diet should be provided including 45–65% carbohydrates, 10–35% proteins and 20–35% fats. Calcium intake should be 1200–1500 mg per day. Patients should take a daily multivitamin and iron supplement.2 7 15
During the period of nutritional stabilisation, patients may show suicidal or depressive ideation as specific weights are reached or they notice changes in their body shape. Acne, breast pain, bloating, fluid retention, delayed gut motility and constipation can all occur. These can be distressing for patients who were previously pathologically in control of their own body. Psychiatric input is important during this period.
Re-feeding syndrome
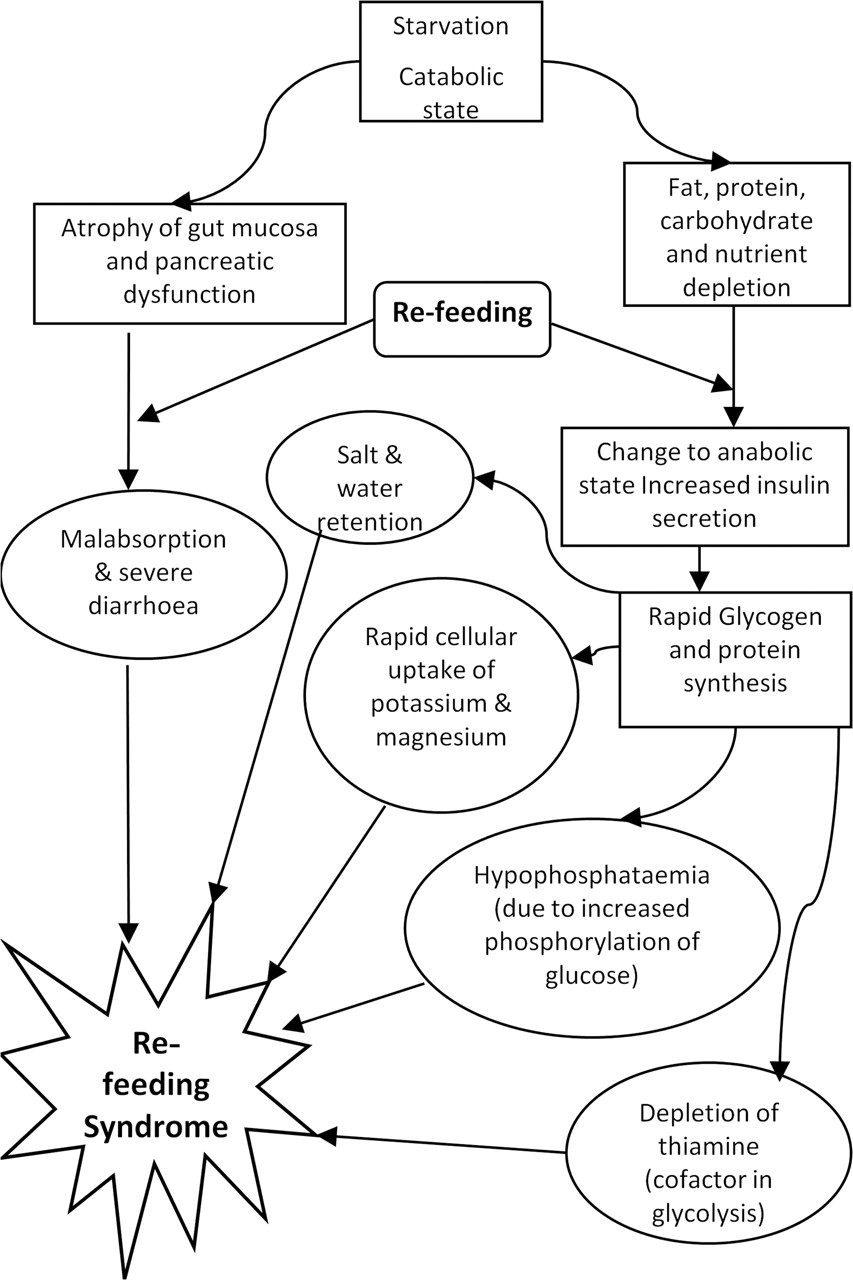
First described at the end of the Second World War, RFS is a potentially lethal combination of fluid and electrolyte shifts. It occurs acutely in severely malnourished individuals when feeding is re-started. The key biochemical abnormality is hypophosphataemia, but other derangements include hypokalaemia, hypomagnesaemia, acute thiamine deficiency, salt and water retention and hypoglycaemia. Re-feeding of grossly malnourished individuals can cause fatal diarrhoea, heart failure, coma and convulsions.12 15
Prolonged starvation causes protein breakdown with loss of skeletal and cardiac muscle mass. This is associated with loss of phosphate (the most abundant intracellular anion), potassium (which electrically balances negatively charged protein molecules) and water. The serum levels of phosphate and potassium may remain normal but the body as a whole may be depleted of these ions. When the malnourished patient receives a carbohydrate load, the body switches from catabolism to anabolism. This leads to a large increase in intracellular requirements for phosphate and causes hypophosphataemia. Phosphate is needed in many intracellular enzyme systems and to make adenosine triphosphate, 2,3-diphosphoglycerate and creatine phosphokinase. Requirements for potassium and thiamine also increase (Fig 1).
{kind=link}
Re-feeding syndrome diagram.
The development of RFS must be anticipated and prophylactic treatment given. The key features to identify are
Salt and water retention, fluid overload and cardiac failure. Even in cases that do not progress to RFS, oedema can be seen within a few days of re-feeding due to fluid imbalance.
Electrolyte imbalances.
Muscle weakness (due to depletion of myocyte ATP and possible sarcolemmal failure with rhabdomyolysis).
Diarrhoea.
Respiratory compromise (due to muscle weakness and diaphragmatic atrophy).
Delirium, hallucinations and decreased consciousness level.
Encephalopathy and seizures.
Delirium has been reported in the second week of re-feeding and may continue for several weeks, unaffected by correcting phosphate.27 Deficiency of thiamine can lead to Wernicke's encephalopathy, which may be irreversible. Re-feeding has also been linked with liver damage. There may be an increase in liver enzymes consistent with fatty infiltration, nutritional hepatitis or hypoperfusion.21
Re-feeding is central to the treatment of AN. Although many different feeding regimens have been suggested, randomised controlled trials have not shown any to be superior at avoiding the problems of RFS. Bearing this in mind, the following factors should be considered.
First, calorie intake should initially be kept low, at approximately the current level of intake and increases should be undertaken regularly but in a timely fashion with guidance from a dietitian. There is a temptation to give a very low calorie intake to avoid RFS but underfeeding can worsen symptoms as much as overfeeding can precipitate RFS.
Second, particular care should be taken regarding fluid and electrolyte balance. Serum electrolytes should be measured before re-feeding, six hours after commencing intake and then daily. Supplemental electrolytes may be required prophylactically, particularly phosphate, and these should be replaced in a timely fashion.7 Fluid balance should be closely monitored, particularly with regard to renal function. Fluid restriction may be appropriate in some patients but only after discussion with specialist teams.
Finally, vitamin supplements should be prescribed in the form of a multivitamin and thiamine preparation.3
Although the guidance shown in table 2 may be helpful in identifying high-risk patients, assessing the risk of RFS accurately is difficult. Incidence increases as BMI decreases and if weight loss is rapid. The greatest period of risk is within the first week of re-commencing nutrition. Observations and monitoring should therefore be continued until the patient shows signs of biochemical and cardiovascular stability.28 It is hard to set firm criteria because of normal variability of BMI, physiology and behaviour in patients of different ages.
Drug therapy in malnutrition
In malnutrition, care must be taken when prescribing medications.25 Particular consideration should be given to:
Drug absorption – if given orally is the drug being absorbed?
Low albumin and effect on drug binding – dose reductions may be required when drugs are highly protein bound.
Effect of abnormal electrolytes and malnutrition on drug function.
Drug metabolism – enzyme function, how is the drug metabolised? This can be affected by pH and electrolyte balance.
Renal and liver function – drug excretion and metabolism. Drug doses may need to be reduced to take account for this, especially antibiotics.
Drugs that affect QTc – long QTc is common in AN patients. Drugs that prolong QTc may lead to fatal arrhythmias.
Increased adverse reactions to certain medications in malnutrition.
Adverse reactions to monoamine-oxidase inihibitor (MAOI)and tricyclic antidepressants are more pronounced in malnutrition.
Bupropion should be avoided due to increased seizure risk in patients with eating disorders.
High risk of dependence on benzodiazepines – avoid where possible.
Legal and ethical issues in AN
When a young person presents with life-threatening complications of AN, the clinical team will be faced with legal, ethical and emotional challenges including
▶ Capacity and consent, including refusal of treatment.
▶ Use of coercion and restraint.
▶ Parental involvement and collaboration
▶ Avoiding collusion and manipulation.
Several legal documents are relevant to this discussion, as well as standards in British Common Law. The fundamental principle underlying these legal frameworks is that care decisions must be taken in the best interests of the patient.
Capacity and consent
In some cases, young people may have become so unwell that they present to hospital ‘peri-arrest’. In emergency situations, current General Medical Councilguidance allows life-saving resuscitation, even when the patient's consent to treatment is uncertain.29
Once initial resuscitation has occurred, a patient in a critical care setting may express a wish not to be treated either verbally or non-verbally. If these actions put the patient's life at risk (eg, self-removal of central venous or arterial catheters), action must be taken to provide emergency stabilisation. Following this, a stepwise approach guided by the principles of good medical practice should be followed.30
The first priority is to establish the best interests of patients by listening to their concerns and thoughts around treatment. It is important to attempt to gain basic cooperation and make an assessment of patients' capacity and competence. If patients are younger than 18 years of age and competent, they can consent to treatment. However, even if patients are deemed competent, they cannot refuse treatment. Parents of a child younger than 18 can consent to treatment on behalf of their child. In most cases, communication between the clinical team, young person and family should result in a decision acceptable to all. Despite best efforts, this is not always possible. There are likely to be barriers to competence in a young person suffering from AN and the burden on parents to consent to treatment against the wishes of their child, can be difficult.
When neither young person nor parent will consent, there are three options available to the clinical team. The first utilises the principle of best interests to allow emergency treatment if needed. Alternative options are to use the mental health act31 or to apply for a court ruling under the terms of the Children's Act 1989.32 In the case of a young person in a critical care setting, it is probably more appropriate to apply to the courts, as treatment will focus on medical management. GMC guidance is to seek legal advice if competent young persons and/or their parents refuse to consent to treatment felt to be in the patients' best interests by the clinical team.30
Coercion and restraint
Coercion can include use of legal interventions, parental consent overruling the young person's wishes and techniques, such as rewards or withholding privileges.
While use of coercion can be controversial, there is general consensus to support its use in at-risk patients. There is debate about whether to use coercion in patients who retain capacity.33 The use of legal coercion tends to be associated with a high health risk (low BMI/increased risk of RFS), higher complexity condition (eg, other psychiatric co-morbidities) and a high number of previous admissions.34 There is evidence to suggest that young people who have had legally coerced treatment as opposed to voluntary treatment, have a higher mortality rate.35
The Mental Capacity Act36 has useful advice regarding use of restraint, however, it cannot be legally applied to people younger than 16 years. Under the terms of the Act, restraint is allowed only if the person using it reasonably believes it is necessary to prevent harm. The restraint must be proportionate to the likelihood and seriousness of the harm. These are useful guiding principles, to help decide if the use of restraint is appropriate. If deemed appropriate, it is sensible to seek legal advice and to discuss the use of restraint in the court application for treatment.
Parental involvement and collaboration
Dealing with complex family dynamics and history is beyond the scope of this article. An awareness of interfamily dynamics and potential effects on the patient are vital.37 It is important to include the family in the care of the patient while ensuring confidentiality and dignity are respected. This is especially important if there have been disagreements between the clinical team and the patient/family around treatment decisions or if the courts have been involved. As the team moves away from the resuscitation phase towards long-term rehabilitation, ongoing cooperation with the young person and parents is vital. Medical staff should guard against being pulled in to family conflict, and keep the patient at the heart of any decisions.
Collusion and manipulation
The desire for control and the ability to manipulate family, friends, teachers and clinicians is a well-recognised trait of AN.38 This can be challenging for medical, nursing and allied health professionals working with young people. In the critical care setting, there may be several specialists involved in the management of the patient. It is helpful to identify a lead professional and provide clear rules for nursing and medical staff, so that consistent messages are given. It is just as important to establish boundaries with the parents as the patient.
Conclusion
The medical care of patients with AN is a challenge likely to be faced by most general paediatricians at some stage of their career. Providing appropriate care requires attention to detail and should involve a multidisciplinary approach. If complications occur, specialists should be involved to give advice on medical management. A clear understanding of the ethical and legal challenges is essential. The development of departmental guidelines and clear channels of communication with the eating disorder team can help reduce morbidity, mortality and length of acute admission. We advocate forward planning before such patients require admission and the development of a lead clinician for overseeing patient care.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.