Article Text

Abstract
Guidelines are integral to reducing variation in paediatric care by ensuring that children receive the right care, every time. However, for reasons discussed in this paper, clinicians do not always follow evidence-based guidelines. Strategies to improve guideline usage tend to focus on dissemination and education. These approaches, however, do not address some of the more complex factors that influence whether a guideline is used in clinical practice. In this article, part of the Equipped Quality Improvement series, we outline the literature on barriers to guideline adherence and present practical solutions to address these barriers. Examples outlined include the use of care bundles, integrated care pathways and quality improvement collaboratives. A sophisticated information technology system can improve the use of evidence-based guidelines and provide organisations with valuable data for learning and improvement. Key to success is the support of an organisation that places reliability of service delivery as the way business is done. To do this requires leadership from clinicians in multidisciplinary teams and a system of continual improvement. By learning from successful approaches, we believe that all healthcare organisations can ensure the right care for each patient, every time.
- Paediatric Practice
- Evidence Based Medicine
- Multidisciplinary team-care
Statistics from Altmetric.com
Introduction
Recent years have seen the development of numerous, accepted, evidence-based guidelines for clinical practice. So why don’t clinicians follow them?
High-quality healthcare has many different domains, but at its core is the need to ensure that care is effective. It is therefore important that patients receive evidence-based care every time that they are treated. Unfortunately, studies have demonstrated that the delivery of evidence-based care is erratic and occurs only 50%–55% of the time.1 2
There is a growing body of literature that has looked at clinicians and guideline adherence. Common themes are that guideline complexity makes it difficult to follow or clinicians feel it is not relevant to their situation. Clinicians may not be aware of the guideline or be able to access it easily. There is also an uneasy relationship between guideline usage and professional autonomy. Strategies to improve guideline usage tend to focus on dissemination and education. These approaches, however, do not address some of the more complex individual and systemic factors that influence whether a guideline is used in clinical practice.
This paper explores the issues that need to be overcome if we are to move to the delivery of care that is the right care every time, and the practical approaches to achieving this.
Why doctors don’t follow guidelines
In order to consider approaches to improving clinician adherence to guidelines, it is important to understand reasons for non-adherence. Cabana et al 3 reviewed the literature for barriers to physician adherence to clinical practice guidelines and organised these into a framework.3 They argue that before guidelines can affect patient outcomes, they first affect physician’s knowledge, then attitudes, then behaviour (acknowledging that behaviour can be changed without a change in knowledge or attitude, but this is unlikely to be sustained) (table 1).
Barriers to physician adherence to guidelines
The awareness to adherence model is an alternative framework to understand why physicians do not follow guidelines.4 This model was based on adherence to US paediatric vaccine recommendations. It proposed that for physicians to comply with guidelines, they must first be aware of them, then intellectually agree with them, then decide to adopt them and then regularly adhere to them when appropriate.4 They suggested different factors may affect movement along this path; however, their model does not incorporate such complex behavioural constructs as Cabana et al’s review.
In our experience there is also a perceived conflict between professionalism, autonomy and guideline adherence.
Autonomy and professionalism
In a profession where autonomy is a cornerstone of professional identity (even enshrined in the Warsaw Declaration of Physician Autonomy),5 clinical guidelines and standardised care can be perceived as being in direct opposition to the very concept of professionalism. While there is a drive to make guideline compliance a key pillar of quality healthcare, many clinicians see guidelines as a poor alternative to autonomy and experience-based decision making. Online medical blogs and opinion editorials often call guideline-based medicine the end of the ‘art of medicine’ and say that it is at odds with individualised care. We can inform and educate and engage, but if clinicians feel that following guidelines undermines their professional identity, they will not do it.
Professionalism has to be understood in order for it to be influenced. Box 1 outlines the key characteristics of a professional as noted by Starr.6
Characteristics of a professional6
Distinctive competence (as society is dependent on the health professional)
Asymmetric competence (as more knowledge lies with the professional)
Specific attributes
Cognitive skills of science and technology
Moral commitment to do good, putting patients interests ahead of their own, resulting in trust
Collegial commitment to ensure competence by self-monitoring and discipline
Collective advocacy for social welfare
Professional autonomy with self-regulation
Since 1982, the role of the doctor has changed considerably. Patients have access to the internet so the asymmetry of knowledge has changed. It could also be argued that the vast expansion in medical knowledge over the past years has meant that the ‘cognitive skills’ required are no longer the retention of vast lists of medical facts but instead the skills to interpret evidence and put it into practice, something that evidence-based guidelines support.
A final and significant change to professional identity is the development of team working. The complexity of chronic care has meant that doctors are no longer sole providers of care. Doctors are now part of a complex teams with defined roles. This change has not been matched by a change in the concept of professionalism. Amalberti et al 7 have concluded that in order to work in the modern safe service, doctors will need to7:
Accept limitations on maximum performance
Abandon professional autonomy
Move from the mindset of being a craftsman to being equivalent actor
Accept system-level arbitration to optimise safety strategies
Simplify professional rules and regulations
In a study of adherence to National Institute for Health and Care Excellence guidance, it was identified that guideline adherence was influenced by ‘the degree to which decisions rest with an individual or requires team or organisational agreement’. In specialties with high levels of individual clinician autonomy (eg, surgery), adherence was low.8 This is perhaps unsurprising. Effective teams need shared goals and this includes consistency in clinical approaches and guidelines can provide this. Interestingly we are now seeing a shift in attitudes within highly autonomous specialties such as surgery, most obviously evidenced by the phenomenal uptake and impact of the WHO Surgical Checklist.9 We believe that standardising practice to ensure evidence-based care and reduce variation does not have to be at odds with professionalism.
Understanding barriers to guideline adherence is essential. However, it is important to understand that the relative contributions of these barriers differ with both the evidence-based practice (ie, the guideline itself), whether the guideline applies to common, high-volume conditions or those that are less common with lower volume, context of application (ie, general paediatric or specialist setting) and the local culture. In addition the number of staff may impact on how tightly the guideline is followed. In smaller teams, it may be easier to have agreement on how to treat a condition. It is crucial to truly understand local barriers since often interventions to overcome barriers are implemented without investigating the actual reasons for poor compliance. For example, if knowledge or awareness of a guideline is not the barrier, then educating the staff will be unlikely to improve adherence.
Solutions to improving guideline adherence
There are many strategies to improve adherence to clinical guidelines beyond the traditional approach of summarising the evidence in a document, and technology is now offering some innovative solutions. Strategies that are successful in one setting may be less useful in a different setting where barriers differ. Pronovost10 argues that guideline developers should ‘consider barriers, explore theories of change and suggest ways to implement guidelines at the bedside’ (p. 2501).10 They outline five specific strategies:
Include a checklist with interventions linked in time and space
Currently guideline developers summarise the evidence with many interventions listed in a long document and rarely prioritise key interventions. Pronovost10 suggests clearly outlining a checklist with interventions described as unambiguous behaviours linked in time and space (eg, on admission), and transparently defining levels of evidence so the benefit for patients is clear. Furthermore they propose that checklist developers obtain input from a diverse group of clinicians to gain insight to areas lacking strong empirical evidence.10
Care bundles are an example of an approach to improve guideline adherence by prioritising key interventions (see box 2). They should also encourage review of evidence and continual modification of guidelines, engendering staff education in best practice. Dellinger and Vincent11 suggest that care bundles should be used as performance improvement tools to standardise educational efforts and provide regular performance feedback.11 However, compliance with care bundles requires education and an understanding of the context in which they will be used.12
Care bundles to improve guideline adherence
A ‘care bundle’ is a group of (usually 3–5) interventions that, when executed collectively and reliably, produce better outcomes than when implemented individually. Care bundles have been very successful in the reduction of line infections, ventilator-associated pneumonia, pressure ulcers, falls, sepsis and VTE.13 24–27 Their aim is to create motivational user-friendly tools to accelerate the transfer of research from the bench to the bedside, while allowing concurrent data gathering to identify and track change in practice and clinical outcome.
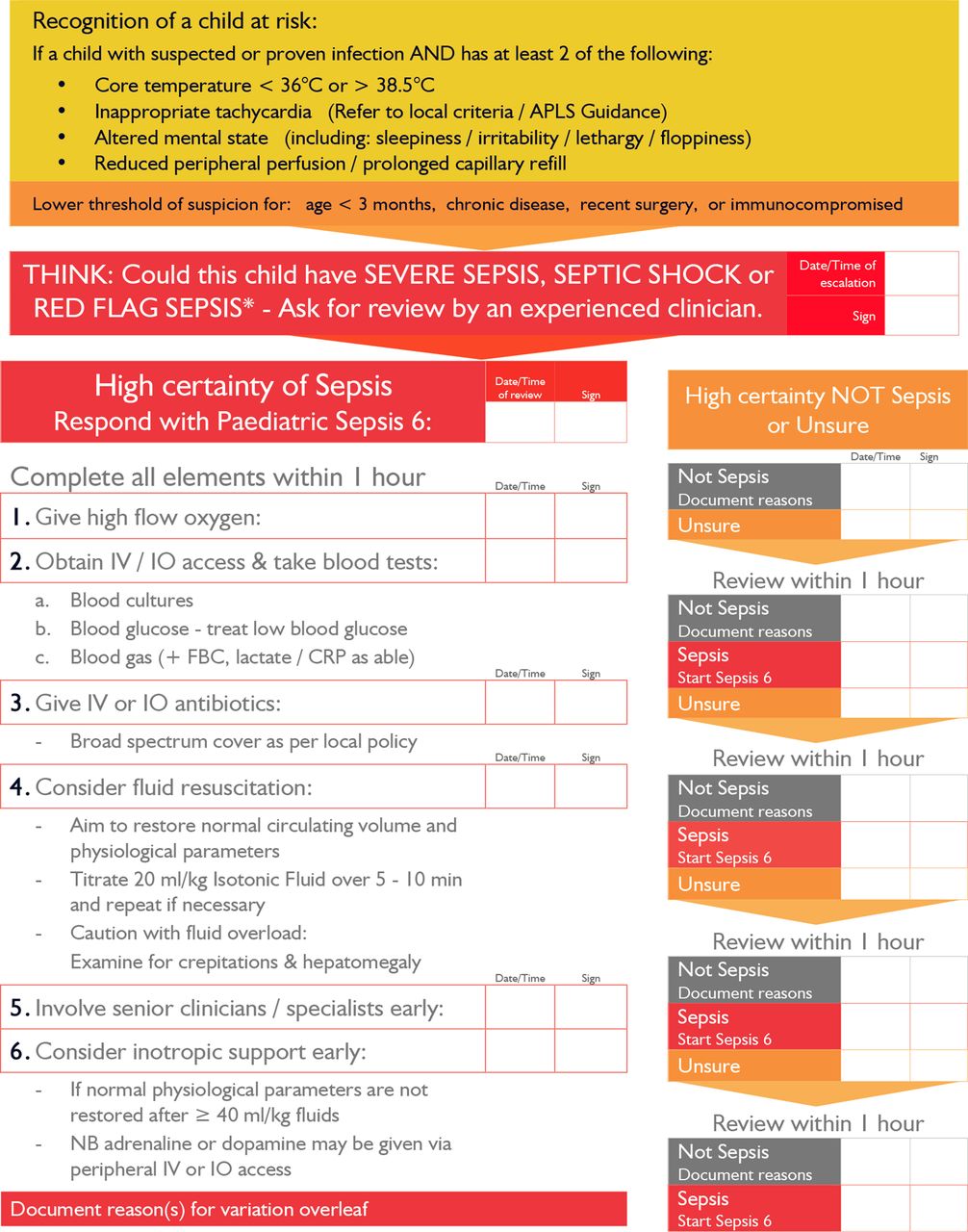
The Surviving Sepsis Campaign produced evidence-based care guidelines for the management of severe sepsis,28 and then created ‘sepsis change bundles’ for initial resuscitation and management, in collaboration with the Institute for Healthcare Improvement. The UK Sepsis Trust developed the Paediatric Sepsis 6 (figure 1), a simplified and easily deliverable sepsis bundle for children.29
{kind=link}
Paediatric Sepsis 6.
Guideline developers, clinicians and implementation scientists share successful implementation strategies
Guideline developers can help clinicians identify and mitigate barriers to adherence, and thus share successful implementation strategies. Each of the barriers outlined by Cabana et al (see previous section) has separate interventions, as outlined in table 2.
Barriers and interventions to improve guideline compliance
Researchers and implementation scientists need to engage with clinicians, looking to understand why they struggle and talking to them about their concerns. Pronovost10 suggests that these barriers should be summarised and interventions pilot-tested. This information can be shared with healthcare organisations so that they can select strategies that may work for them in their local context.10 Box 3 shows examples of collaborative approaches to guideline implementations that allow sharing of information and study of the different contexts.
Quality improvement collaboratives
Quality improvement collaboratives are increasingly used to achieve rapid improvements in healthcare by spreading new knowledge and innovations, which are planned and tested by multiprofessional teams locally. Lessons from previous collaboratives have shown the importance of choosing a subject in which there is evidence of effective interventions and of gaps between best and current practice.30 Collaboratives can therefore be an effective way of implementing evidence-based practice, encouraging adherence to guidelines locally, by using improvement methodology.
The Vermont Oxford Network is an international non-profit voluntary collaboration of multidisciplinary healthcare professionals committed to demonstrating measurable improvements in quality and safety of neonatal care.31 iNICQ is a recent collaborative approach led by this network, focusing on evidence-based best practices to reduce the overuse of antibiotics on neonatal units.
Other paediatric collaboratives include Solutions For Patient Safety (http://www.solutionsforpatientsafety.org), a network of US children’s hospitals ‘working together to eliminate serious harm’, and Making it Safer Together (MiST) paediatric patient safety collaborative in the UK (http://www.mistuk.org/).
Integrate guidelines for conditions that commonly coexist
Current guidelines usually address a single condition or complication, yet it may be of benefit to re-create common scenarios, for example an intensive care unit patient is at risk of healthcare-associated infections, ventilator- associated pneumonia and other harms, each with its own checklist or recommended care practices (and therefore many interventions). By collating and integrating these interventions into a care pathway (see box 4) or daily workflow, the delivery of these practices may be more reliable.13
Integrated care pathways
A care pathway is a complex intervention for the mutual decision making and organisation of care processes for a well-defined group of patients during a well-defined period.32 Defining characteristics of care pathways described by European Pathway Association (EPA)32 include:
An explicit statement of the goals and key elements of care based on evidence, best practice and patients’ expectations and their characteristics;
Facilitation of the communication among the team members and with patients and families;
Coordination of the care process by coordinating the roles and sequencing the activities of the multidisciplinary care team, patients and their relatives;
Documentation, monitoring and evaluation of variances and outcomes; and
Identification of the appropriate resources.
Examples of paediatric integrated care pathways include the Royal College of Paediatrics and Child Health care pathways for children with allergies (http://www.rcpch.ac.uk/allergy), paediatric diabetes and paediatric cardiac catheterisation, described by Kitchiner and Bundred.33 They allow patient-focused care, incorporating evidence-based guidelines and checklists, and improve multidisciplinary communication (combining medical and nursing notes).
Pathways are usually unique to the institution in which they are developed, but exchange of information between health professionals using similar pathways may be valuable to extend and improve their use.33 The EPA is a not-for-profit organisation to conduct research into methods for coordination of care pathways and support the development, implementation and evaluation of care pathways.32
Rely on systems rather than individual clinicians
Guideline developers should consider the use of technology to ensure patients reliably receive interventions according to guidelines. An example is SIEGFRIED (System for Interactive Electronic Guidelines with Feedback and Resources for Instructional and Educational Development) developed by the University of Pittsburgh for Duke University Medical Center,14 which interactively presents guidelines at the point of care by following algorithms through a series of questions driven by the patient’s data (there is also added value for the clinician with educational resources and links to patient education). Pronovost10 describes an ‘information ecosystem’ based around an electronic medical record that could help predict which patients are at risk of harm and recommend evidence-based interventions.10 Box 5 outlines the approach by Intermountain Healthcare as an example of innovative use of technology.15
Use of technology to improve guideline adherence
Information technology (IT) systems can be designed to improve accessibility to updated guidelines, but also to understand why clinicians do not follow existing guidelines. Intermountain Healthcare is a high reliability integrated organisation based in Utah and Idaho that has applied Deming’s process management theory to drive quality and reduce cost. They aim to measure, understand and manage variation among clinicians using their data systems. A review in 1995 showed that 65 quality improvement interventions had reduced the cost of clinical care by improving patients’ clinical outcomes.15 One intervention was an evidence-based clinical practice guideline for managing ventilator settings for acute respiratory distress syndrome, which they blended into the flow of bedside clinical work, adding it to checklists, order sets and clinical flow sheets which track patient’s physiological information. The clinicians had to adapt the guideline to each patient, but they recorded these adaptations as variance and reported them back to the clinical team. The guideline could be modified in response, but also clinicians could modify their own practices to ensure they followed the evidence-based practice as closely as possible. Guideline variance was reduced from 59% to 5% within 4 months for a category of these patients, with the feedback loop providing 124 changes to the guideline in this period.15 As a result, Intermountain Healthcare has identified other clinical processes associated with specific clinical conditions for which they collect data on guideline adherence (and variation).
Other international healthcare leaders using IT for guideline adherence include:
The Royal Children’s hospital Melbourne—free web-based clinical practice guidelines
www.guidelines.co.uk—a resource to bring together all UK national guidelines for primary care use
UK primary care electronic patient records (eg, System One, EMIS) now incorporate clinical guidelines to support decision making
Create transdisciplinary teams
Teams that pool expertise from clinical epidemiology, implementation science and systems engineering may help develop guidelines with practice strategies. There has already been success in interdisciplinary basic science programmes, invested in by the US National Institute of Health.10 Pronovost10 proposes that guideline developers currently lack these essential skills and that this expertise is required to identify and automate guidelines in order to reduce preventable harm.10
To the five steps from Provonost’s team we would suggest adding the following:
Embed guidelines within IT systems to support access and review
Sophisticated use of IT systems can support many of the above solutions, and digital health is an expanding industry. The use of web-based guidelines and apps can help ensure the most up-to-date versions are available and that the guidelines are easily accessible to clinicians. They can also improve ease of guideline use with electronic algorithms, and links to decision making aides, reminders, patient and family information or early warning score systems. In some cases the guidelines can be incorporated into workflow, such as ordering appropriate investigations for common conditions or care pathways, and provide feedback on adherence for governance purposes or accountability. The use of digital health to provide decision support by integrating guidelines into clinical processes allows facilitation of correct decision making.16 Intermountain Healthcare collects valuable information on variance from clinicians, which can result in changes to guidelines to further enhance adherence (see box 5). IT systems can provide useful data for benchmarking for quality improvement collaboratives (see box 3). The ability for an organisation to learn more about guideline use and variance is increasingly recognised as an important use of IT systems.
Delivering the right care, every time
Key to success is the support of an organisation that places reliability of service delivery as the way business is done. The move to the application of evidence-based care all the time in the form of protocols, guidelines and integrated care pathways will need leadership from clinicians in multidisciplinary teams, reliable data, effective use of technology and a system of continual improvement.
Clinical guidelines and integrated care pathways are designed to ensure that the children we treat receive the right care, the first time, every time. This reliability is difficult to achieve if there is constant variation. We all try to provide the right care for our patients all the time. In an age where the complexity of clinical presentation, diagnosis and treatment continues to grow, we cannot rely on our own clinical acumen and decision making any longer. We believe that successful guideline adherence requires proactive engagement of clinicians in the development and review of guidelines and recognition of the role of professional role models. An effective example of this is the Choosing Wisely campaign, which aims to facilitate the adherence to guidelines through making ‘wise choices’.17
The benefits of guideline adherence are not limited to reduced variation. Patients can benefit from having access to guidelines in order to better understand the care they are receiving and to support informed decision making. This is particularly relevant with the development of digital health and the availability of apps on smartphones that can provide the clinical guideline in a readily accessible way. Individual clinicians can use guidelines to inform and improve their practice, and adherence to a guideline can be a support in medicolegal situations. Organisations may be able to translate guideline adherence and improved reliability into cost savings.18 Intermountain Healthcare has done this (see box 5)15 and a report from the New England Healthcare Institute suggests that US healthcare organisations could see combined savings of over US$600 billion.19
Guidelines need to be living documents, constantly revised and amended to ensure that they are able to deal with all possibilities. Intelligent use of technology can assist this. If a patient does not fit the guideline, deviance from the guideline should be studied so that the guideline can be improved. This will result in an enhanced learning environment in which clinicians are constantly studying, learning and improving their practice based on what works and what does not. The new professionalism is about understanding that standardised care is the goal with variation only as required by the patient’s condition and not by a clinician’s individual preference. Only through this will we be able to ensure the right care for every patient, every time.
References
Footnotes
Contributors JR, AR and PL all contributed to the ideas, writing and editing of this article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.