Article Text

Abstract
Pica is defined as the persistent ingestion of non-nutritive substances for more than 1 month at an age at which this behaviour is deemed inappropriate. It occurs most commonly in children, in patients with learning disabilities and in pregnancy. The aetiology of pica is poorly understood and is probably multifactorial. Clinical assessment can be difficult. History and examination should be tailored to address potential complications of the substance being ingested. Complications can be life threatening. Pica often self-remits in younger children. In those with learning disabilities, however, pica may persist into adulthood. Management strategies should involve a multidisciplinary approach, and interventions are primarily behavioural in nature. There is limited evidence to support pharmacological interventions in the management of children with pica.
- Pica
- Geophagia
- Lead Poisoning
- General Paediatrics
Statistics from Altmetric.com
Introduction
Pica is the persistent ingestion of non-nutritive substances for more than 1 month at an age at which this behaviour is deemed inappropriate1 (see box 1). The term originates in the Latin word for magpie, a bird famed for collecting and hoarding unusual objects.2
DSM-V (The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) criteria for the diagnosis of pica
The eating of non-nutritive, non-food substances is persistent over a period of at least 1 month.
The eating of such substances is inappropriate to the developmental level of the individual.
The eating behaviour is not part of a culturally supported or socially normative practice.
If the behaviour occurs within the context of another mental disorder or medical condition, it is sufficiently severe to warrant independent clinical attention.1
Pica can be classified according to the particular substance ingested. Common subtypes are listed in table 1. Ingestion of non-food substances may also be associated with cultural practices. Geophagia, including the ingestion of kaolin (white clay), is seen in sections of the African-American population in the USA and is common practice in parts of Africa.3 Although often described as pica in the literature, these practices may actually be deemed to be socially normative practice and therefore do not fit the diagnostic criteria outlined in The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V).
Common subtypes of pica according to the substance ingested
Pica is most commonly seen in children aged 2 or 3 years old. It may persist into adolescence when it is usually associated with learning difficulties.4 Studies suggest pica can be present in between 5% and 25% of children with learning difficulties. Pica is also common in pregnancy, occurring in up to 28% of cases. It typically occurs in younger women in their first pregnancy.5 This article provides an overview of the possible causes and potential complications of pica. In addition, it discusses important aspects of the clinical assessment, investigation and management of a child presenting with pica.
Aetiology
The aetiology of pica is poorly understood and is probably multifactorial. Proposed mechanisms range from psychosocial to biochemical.
An association between pica and micronutrient deficiencies, including iron, calcium and zinc has been well described. A recent meta-analysis confirmed the association between anaemia, low plasma zinc levels and pica.6 Children with pica may ingest substances rich in the nutrients in which they are deficient. However, there has been limited success in preventing pica in cases where nutritional deficiencies have been identified and treated.
The higher incidence of pica noted in children with learning and developmental disabilities, including autistic spectrum disorder, was traditionally believed to result from an inability to differentiate between food and non-food items. However, current thinking suggests that this is more likely to be secondary to learned behaviours.4 7
Pica in children has also been associated with deprivation, parental neglect and malnutrition.2 It may present in the presence of a coexisting psychiatric disorder, and there is increasing evidence that it may be associated with conditions leading to malabsorption, poor nutritional status or anaemia. Recent literature, for example, has highlighted concerns regarding the increased incidence of pica among children with sickle cell disease.8 9
Clinical presentation
History taking
The clinical presentation of pica is highly variable and depends on the particular substance being ingested and the potential associated complications. History taking should focus on the substance ingested. If there is a risk of poisoning, the history should focus on the consequences of that poisoning. Enquire about symptoms of anaemia, such as pallor, shortness of breath, palpitations and lethargy. Ask about coexisting medical conditions that may predispose to pica. Take a thorough developmental and social history. Explore the patient’s living environment, for example, the risk of exposure to lead.
Challenges may arise in consultations with older children, who might deny pica or show reluctance to disclose information. This may limit the clinician’s ability to make an accurate diagnosis and prediction regarding potential complications.
Clinical examination
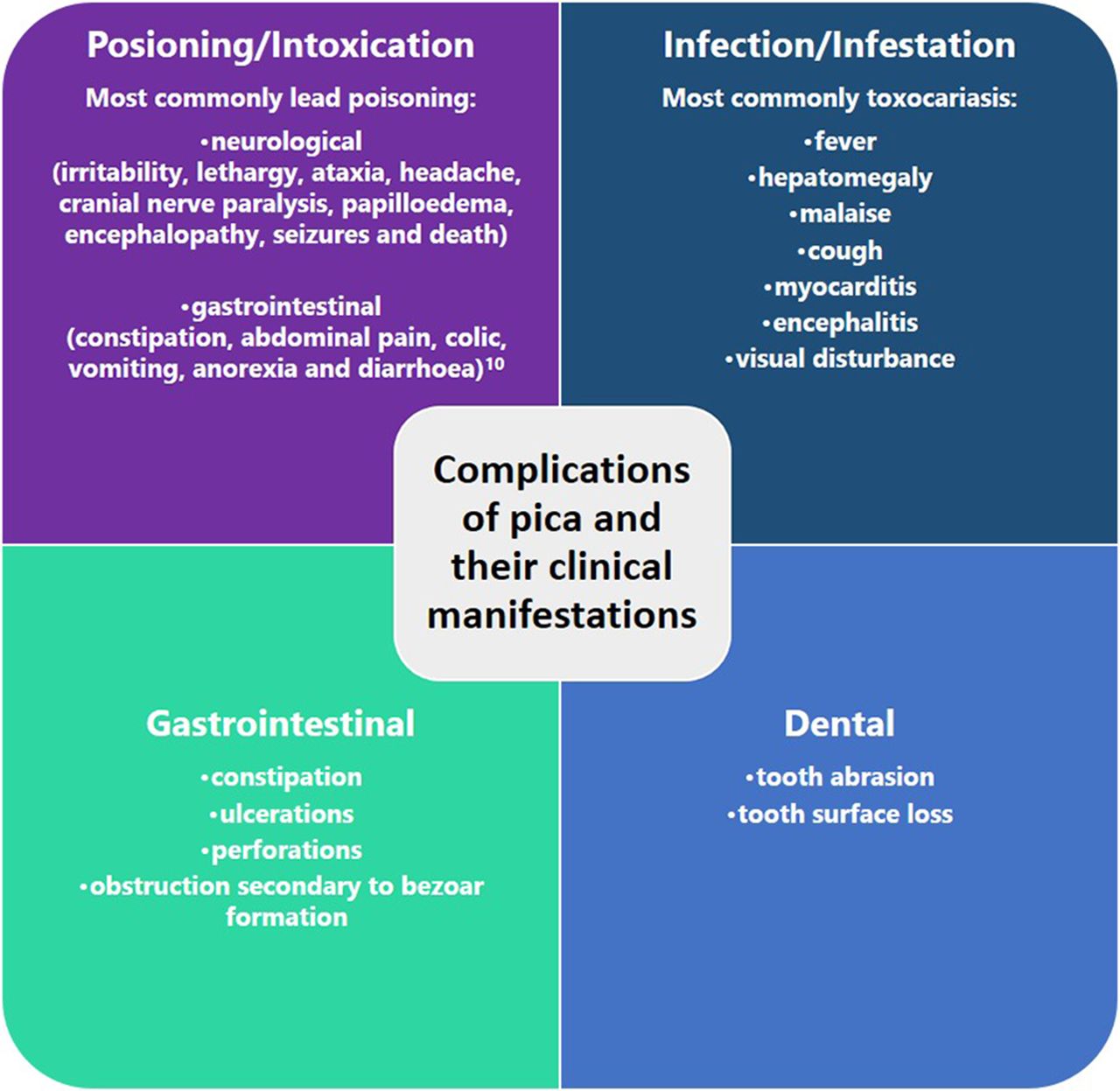
Examination will often be normal in children with pica. Clinical signs are usually secondary to complications of the substance that has been ingested. These can be classified into four main groups (see figure 1):
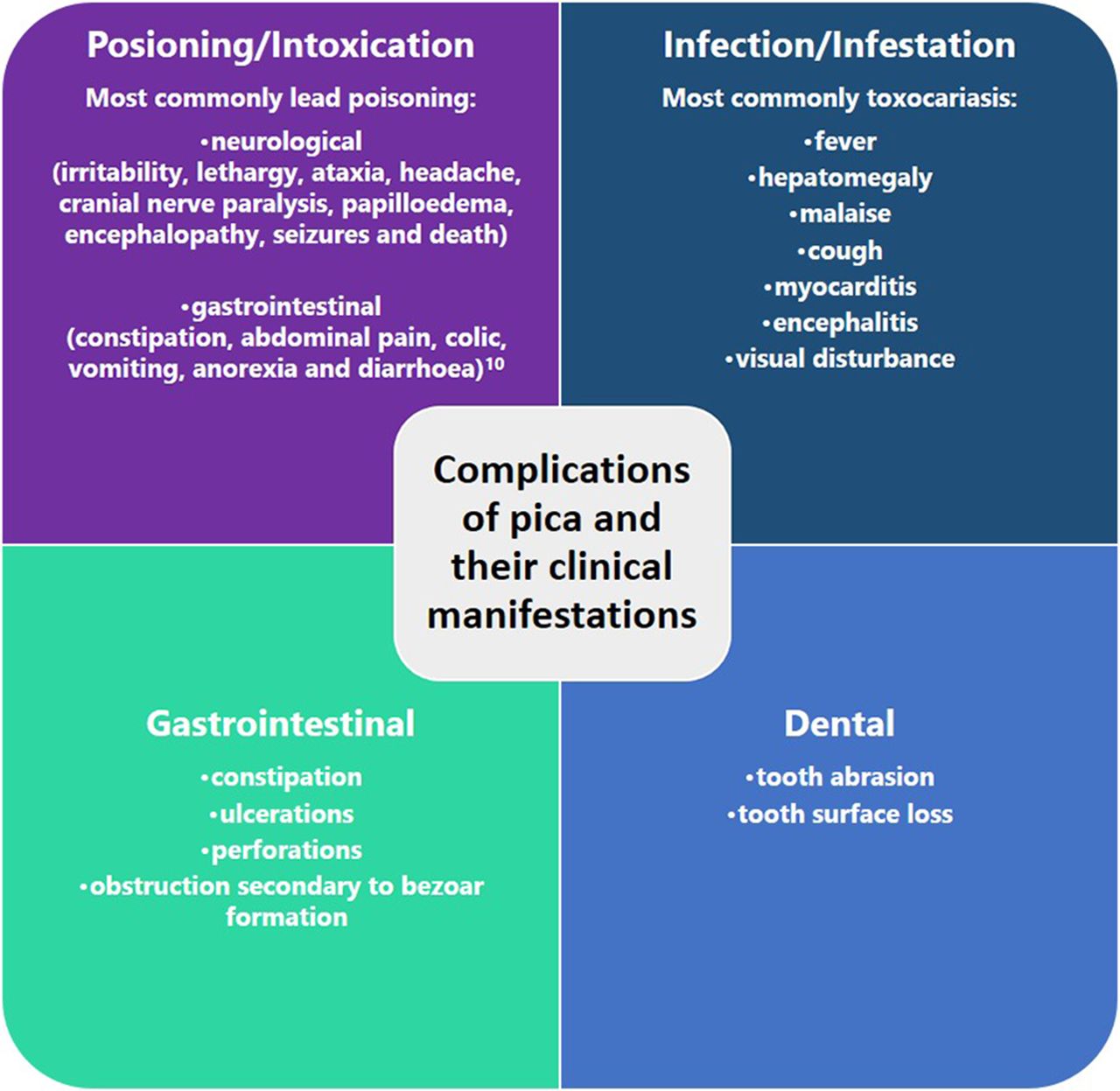
Potential complications of pica and their clinical manifestations.
Manifestations of toxic ingestion:
Lead poisoning is the most common poisoning associated with pica.
Most patients are asymptomatic, and the signs can be very subtle.10
Manifestations of infection or parasitic infestation:
Toxocariasis and ascariasis are the most common parasitic infections associated with pica.
The clinical manifestations relate to the number of larvae ingested and the organs to which the larvae migrate.11
Gastrointestinal manifestations:
Manifestations may be a result of mechanical bowel problems, perforations and intestinal obstructions caused by bezoar formation around indigestible substances.
Dental manifestations:
Manifestations may include severe abrasion and other mechanical damage to tooth substance.12
Investigations
Pica is a clinical diagnosis based on the DSM-V diagnostic criteria. Investigations may be useful in screening for potential causes and complications. The meta-analysis examining micronutrient status and pica noted a strong association between pica and anaemia.6 Check a full-blood picture and iron studies in all children.
Further investigations should be tailored according to the substance ingested and the clinical findings. The American Academy of Pediatrics recommends that routine screening of blood lead concentrations be performed in children who live in residential areas where at least 27% of the houses were built before 1950.10 The prevalence of lead piping in domestic water supplies in the UK has decreased significantly in recent years. However, it is still common in older houses, and knowledge of the local environment is important.13 Check blood lead concentration in children:
with signs or symptoms of poisoning (figure 1)
with a history of ingestion of lead based paints
when environmental exposure is suspected.
There is little evidence to suggest an ideal set of investigations in children presenting with faltering growth.14 Consider checking at least urea and electrolytes, liver function tests, calcium, phosphate magnesium and trace elements in these children.
Imaging studies may be useful if there is a suspicion that abrasive objects have been ingested or there are clinical signs of gastrointestinal obstruction. Plain film of the abdomen may show signs suggestive of trichophagia. However, if there is a palpable mass or signs of obstruction, a contrast study or CT are the investigations of choice.15
Management
Although pica in young children and pregnancy normally remits spontaneously, it is a potentially deadly self-injurious behaviour. This is particularly true when it persists into adolescence and adulthood. Social stigmatisation may also occur. Pica is best managed using a multidisciplinary team approach.16 The team may include physicians, social workers, dieticians, psychologists and dentists. When devising a treatment plan, consider the symptoms and complications that the child is experiencing. Parents and patients should receive education around sound nutritional practices and be made aware of the potential severity of the condition. Treat any nutritional deficiencies identified.
Additional treatment options can be divided into two main groups: behavioural interventions and pharmacological interventions. A variety of behavioural interventions exist (see figure 2):

Behavioural interventions for pica.
positive reinforcement if pica is not attempted;
discrimination training0 between edible and inedible substances;
visual screening, that is, eyes are covered for a short period, if pica is attempted;
aversive presentation if pica is attempted, for example, a bitter taste, such as lemon juice;
Physical interventions:
Self-protection devices that prohibit placement of objects in the mouth;
Time-out if pica is attempted.
Although studies in the existing literature are limited to small sample sizes, it is commonly believed that these methods can be highly effective treatments for pica.16–18
Pharmacological interventions are rarely indicated in pica. The use of selective serotonin reuptake inhibitors has been reported in three adolescents with pica and learning difficulties.19 A further case report describes resolution of pica following the use of methylphenidate to treat comorbid attention-deficit hyperactivity disorder.20

{kind=link}
{kind=link}
{kind=link}
Flow chart depicting literature search.
Key messages
Pica is the persistent ingestion of non-nutritive substances for more than 1 month at an age at which this behaviour is deemed inappropriate.
It occurs most commonly in children, in patients with learning disabilities and in pregnancy.
The aetiology is poorly understood.
History and examination should be tailored to address potential complications of the substance being ingested.
Complications can be life threatening.
Interventions should involve a multidisciplinary approach and are primarily behavioural in nature.
Footnotes
Contributors BM wrote the first draft. TB and AT reviewed the content and suggested amendments that BM incorporated. All authors approved the final version.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.